INTRODUCTION
Tinnitus refers to the false sensation of a ringing or buzzing sound in the absence of external stimuli.1 The prevalence of tinnitus is 10-15% in the general population,2 with approximately one third of individuals with tinnitus experiencing distress and reduced quality of life.3 Tinnitus symptoms are often attributed to diverse causes, including hearing loss, Meniere's disease, and otitis media; however, in many cases, no cause is found.4 As subjective tinnitus generally involves complex symptoms, it is not always possible to fully eliminate.45 The clinical characteristics of tinnitus (e.g., duration of awareness, loudness, location) can vary widely,4 as can symptom severity, ranging from barely noticeable to unbearable and debilitating.4 Tinnitus is believed to have a complex etiology, including ontological and neuropsychological factors6; however, due to the subjectivity of its symptoms, what contributes to tinnitus symptom severity is poorly understood.
Hearing impairment is one of the auditory factors frequently accompanying tinnitus. Several epidemiological studies have shown that the occurrence of tinnitus is related to hearing impairment.78 However, not all (approximately 30%) of patients with hearing loss exhibit tinnitus symptoms.49 Neuroanatomical research has considered the role of neural plasticity followed by reorganization of the cerebral cortex as a cause of tinnitus.10 Hearing loss can lead to a reorganization of the central auditory system.10 However, only a few studies with small samples have used objective audiometric tests to examine hearing levels in patients with tinnitus.78 Therefore, despite its clinical importance, the relationship between hearing loss and tinnitus symptom severity remains unclear.
Other important etiologies of tinnitus are neuropsychological factors such as depression and anxiety.1112 Several studies have described tinnitus as a subjective experience associated with emotional and cognitive problems rather than objective auditory problems.1113 Additionally, the high prevalence of psychological symptoms, including depression and anxiety, in patients with tinnitus is well documented.14151617 Despite the strong correlations between tinnitus and psychiatric symptoms,17 a causal relationship has not been established because depressive and anxiety symptoms reflect a state, rather than a trait, before illness. Several reports have suggested that personality or trait factors such as neuroticism,18 temperament,19 and trait anxiety2021 might exacerbate tinnitus symptoms. Anxiety sensitivity is also considered a premorbid personal characteristic, defined as a tendency toward anxious responses to somatic perception.22 Several studies have shown that anxiety sensitivity is associated with tinnitus symptoms.2324 Andersson and Vretblad.23 suggested that anxiety sensitivity could be a causative factor for tinnitus-related distress. However, further research is required to evaluate the role of anxiety sensitivity as a predictor of tinnitus symptom severity in a large sample.
We presume that both hearing loss (i.e., reorganization of auditory nerves) and anxiety sensitivity (susceptibility to somatic sensations) are associated with tinnitus symptoms. Accordingly, these two factors must be considered important predictors of tinnitus symptom severity. The aim of the current study was determine the precise effects of anxiety sensitivity and hearing loss on tinnitus symptom severity in a large clinical sample of patients with tinnitus. Furthermore, we hypothesized that these associations differ according to the characteristics of tinnitus symptoms.
METHODS
Participants and procedure
We reviewed the medical records and self-reported questionnaire responses of 1,797 patients who presented with tinnitus symptoms as a chief complaint at the tinnitus clinic in Soree Ear Hospital between May 2015 and April 2016. Basic demographic data, self-report questionnaires and pure-tone audiometry results were obtained from patients' medical records. Patients underwent audiometry and completed a battery of self-report questionnaires during waiting period before clinic encounter. The Korean versions of the Tinnitus Handicap Inventory (THI), Hospital Anxiety and Depression Scale (HADS), and Anxiety Sensitivity Index (ASI), and visual analog scales (VASs) were used to examine tinnitus symptoms and psychological status as a part of medical care. This study was reviewed by the Institutional Review Board (IRB) at the National Center for Mental Health and was considered exempt from informed consent requirements (2015-04-13).
Measures
Information regarding patients' tinnitus-related symptoms (i.e., awareness time, loudness, degree of annoyance, and impact on life) over the preceding month was assessed using VASs. Awareness time of tinnitus was measured as the proportion of the day during which patients were aware of their tinnitus symptoms, with responses ranging from 0% (no awareness during the day) to 100% (full awareness all day). Responses regarding loudness of tinnitus ranged from 0 (inaudible) to 10 (intolerably loud). Degree of annoyance ranged from 0 (no annoyance) to 10 (extreme annoyance). Finally, the impact of tinnitus on life ranged from 0 (no impact) to 10 (incapacitation).
The Korean version of the THI was used to measure the severity of tinnitus-related handicap.25 This scale was originally developed by Newman et al. to measure the perceived disability caused by tinnitus and related distress. The Korean version of the THI was standardized by Kim et al.26 The questionnaire comprises 25 items that determine whether participants experience particular difficulties (e.g., difficulty concentrating, confusion, and anger) resulting from tinnitus. Possible responses include “yes,” “sometimes,” and “no” (yes=4 points, sometimes=2 points, no=0 points). Total scores range from 0 to 100, with higher scores indicating higher levels of perceived tinnitus-related handicap and distress.2526
The ASI2227 was used to measure fear of anxiety-related sensations and the belief that anxiety symptoms have negative consequences. The questionnaire comprises 16 items measuring the extent to which participants are concerned about the negative consequences of anxiety symptoms.22 Responses are provided using a five-point Likert scale ranging from 0 (very little) to 4 (very much). The total ASI score ranges from 0 to 64 and represents an individual's level of anxiety sensitivity.27 Note that the ASI score reflects responses to physical symptoms associated with anxiety rather than individuals' current levels of anxiety.22 Furthermore, anxiety sensitivity has been shown to be a comparatively stable characteristic.2829 The cutoff for high ASI was set at 21 or greater.
The HADS,3031 a measure of current anxiety and depressive symptoms among patients visiting general hospitals, was used to assess participants' anxiety and depression levels. The scale comprises 14 items divided between two subscales measuring anxiety and depressive symptoms, each with a cutoff score of 8 for clinical levels of anxiety/depression.3031
Pure-tone audiometric testing was performed in sound-treated booths (Sontek Company, Paju, Korea) using 2-channel pure-tone audiometers (Madsen Auricla/Astera2, Otometrics) equipped with TDH-49 earphones. Pure-tone air conduction thresholds were obtained for each ear at 500, 1,000, 2,000, and 4,000 Hz. Hearing loss was considered present if subjects' pure-tone average exceeded 25 dB. We also graded the severity of participants' hearing loss as follows: mild (25-40 dB), moderate (40-60 dB), and severe (>60 dB).
Data analysis
Analyses were performed using SPSS Statistics 21.0 for Windows (IBM Corp., Armonk, NY, USA). We compared the differences in demographic and clinical variables between four groups based on anxiety sensitivity level (AS) and severity of hearing loss (HL), including those with normal anxiety sensitivity and hearing level (AS-/NH), normal anxiety sensitivity and hearing loss (AS/-HL), high anxiety sensitivity and normal hearing (AS+/NH), and high anxiety sensitivity and hearing loss (AS+/HL). Comparisons were performed via analysis of variance (ANOVA) with Tukey's HSD post-hoc tests for continuous variables and Kruskal-Wallis H tests for categorical variables. To determine which variables (hearing level, anxiety sensitivity, current anxiety, and depressive symptoms) predict tinnitus symptom severity (awareness, loudness, annoyance, impact on life, and THI score), we performed multiple linear regression analyses after controlling for age, sex, duration of illness, and location of tinnitus. The significance level was set at p<0.05. We adjusted the p-values for each regression model for multiple comparisons using Bonferroni corrections.
RESULTS
Description of study population and the result of group comparisons
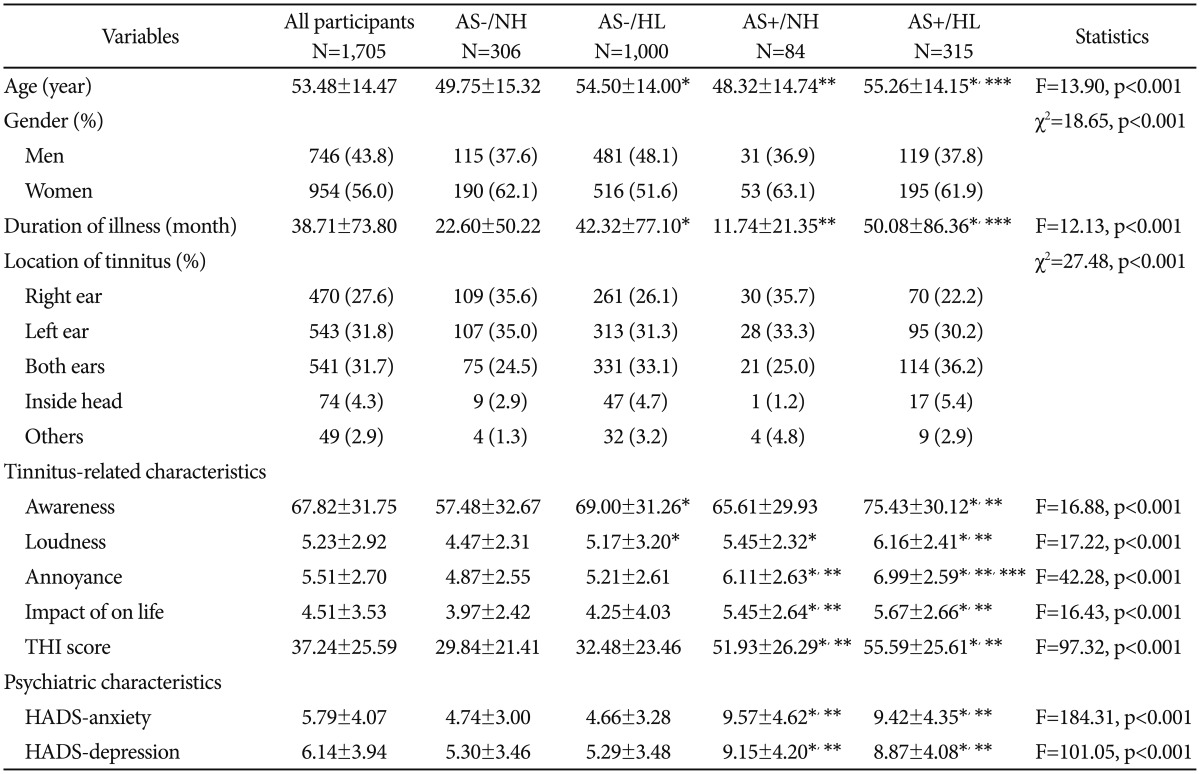
Participants' sociodemographic and clinical characteristics are summarized in Table 1. Of the 1,705 patients with tinnitus included in this study, 749 (43.8%) were men. Participants' mean age was 53.48±14.47 (range: 18-97) years, and the mean tinnitus duration was 38.71±73.80 (range: 0-696) months. Regarding the perceived tinnitus location, 470 (27.6%) patients reported it in their right ear, 543 (31.8%) in their left ear, 541 (31.7%) in both ears, 74 (4.3%) inside the head and 49 (2.9%) in other locations. The missing value was 28 (1.6%). The average proportion of the day during which participants were aware of tinnitus symptoms was 67.82±31.75%. The mean scores for tinnitus loudness, degree of annoyance, and impact on life were 5.23±2.92, 5.51±2.70, and 4.51±3.53, respectively. The mean total THI score was 37.24±25.59. Furthermore, the mean total ASI score was 13.56±12.47, and the numbers of participants whose anxiety sensitivity levels were categorized as normal and high according to the abovementioned cutoff were 1,306 (76.6%) and 399 (23.4%), respectively. The number of participants with normal hearing was 390 (22.9%). Of the patients with hearing loss, 308 (18.1%), 342 (20.1%), and 665 (39.0%) exhibited mild, moderate, and severe hearing loss, respectively.
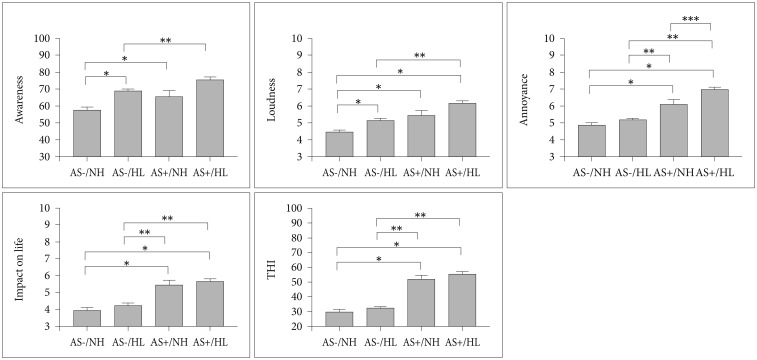
Table 1 also shows results of the comparison of the four groups. There were 306 (17.9%) participants in the AS-/NH group, 1,000 (55.6%) in the AS-/HL group, 84 (4.9%) in the AS+/NH group, and 315 (18.5%) in the AS+/HL group. We observed significant differences in tinnitus symptom severity between these groups [awareness: F (3, 1525)=16.88, p<0.001; loudness: F (3, 1556)=17.22, p<0.001; annoyance: F (3, 1565)=42.28, p<0.001; impact on life: F (3, 1557)=16.43, p<0.003; THI: F (3, 1701)=97.32, p<0.001]. The results of the post-hoc analysis of group differences are shown in Table 1, Figure 1.
Multiple regression analyses
Table 2 depicts the results of the multiple linear regression analyses. Among the independent variables (e.g., severity of hearing loss, ASI score), severity of hearing loss was the only predictor of awareness of tinnitus (β=0.19, t=6.23, p<0.001) and loudness (β=0.11, t=3.60, p<0.001). Annoyance and THI score were significantly predicted by both ASI score (annoyance: β=0.11, t=3.18, p=0.010; THI score: β=0.21, t=7.15, p<0.001) and severity of hearing loss (annoyance: β=0.09, t=3.33, p=0.005; THI score: β=0.10, t=4.27, p<0.001). Neither predictor had a significant relationship with impact on life.
DISCUSSION
Our study investigated the effects of anxiety sensitivity and severity of hearing loss on tinnitus symptom severity. In the group comparison, the AS+/HL group showed the most severe symptoms for each measure of tinnitus severity, including greater awareness, louder sound, greater annoyance level, worse impact on life, and higher THI scores than did the AS-/NH group. Furthermore, the groups with high anxiety sensitivity (AS+/NH and AS+/HL) showed more severe symptoms, including greater annoyance, impact on life, and THI scores, irrespective of their degree of hearing loss (i.e., compared to the AS-/NH and AS-/HL). Among the groups with low anxiety sensitivity, awareness and loudness of tinnitus were significantly greater among patients with hearing loss (AS-/HL) than among those with normal hearing (AS-/NH). Finally, the results of the multiple regression analysis showed that severe hearing impairment and high levels of anxiety sensitivity are significant predictors of tinnitus symptom severity, although the precise aspects of tinnitus severity to which they are related differ. Specifically, awareness and loudness of tinnitus were significantly related to hearing loss, but not anxiety sensitivity. Conversely, annoyance and tinnitus-related handicap were predicted by higher anxiety sensitivity as well as severity of hearing loss.
To our knowledge, this study examined the largest clinical sample of patients with tinnitus in which hearing levels (measured using pure-tone audiometry) and anxiety sensitivity to date. Due to the multidimensional nature of tinnitus, accurate assessment of tinnitus severity must be made using a variety of measures. In our study, tinnitus symptom severity was assessed in terms of awareness, loudness, degree of annoyance, impact on life, and tinnitus-related handicap. Awareness and loudness of tinnitus were presumed to be acoustical symptoms rather than subjective ones. However, degree of annoyance, impact on life, and tinnitus-related handicap were measures of the non-auditory symptoms of tinnitus, including psychological distress and low quality of life.3233 The current consensus is that tinnitus symptoms have multiple etiologies.34 As such, tinnitus might be related to not only dysfunction of the inner ear or auditory nerves but also to cognitive distortions of somatic sensations.634 Our findings further support the notion that auditory factors (i.e., hearing loss) are associated with the acoustical symptoms (awareness and loudness), whereas psychological traits (anxiety sensitivity) are linked with the non-auditory symptoms (annoyance, impact on life and tinnitus-related handicap).
Although previous studies have reported a significant relationship between tinnitus severity and psychiatric symptoms.1435 they did not establish causality-as such, their results indicated that high levels of anxiety and depression could result in tinnitus or vice versa. Therefore, we examined the effect of anxiety sensitivity, which is considered a premorbid trait, on tinnitus symptom severity. Anxiety sensitivity reflects emotional awareness and susceptibility to anxiety-related somatic symptoms, rather than individuals' current anxiety level, and has been identified as an individual characteristic or trait.22 Individuals with high anxiety sensitivity levels could perceive tinnitus as a life-threatening event, and this cognitive distortion might cause severe distress or tinnitus-related disability. Our findings suggested that anxiety sensitivity was predictive of tinnitus symptom severity, particularly degree of annoyance and tinnitus-related handicap. These associations remained significant even after controlling for demographic factors and hearing levels. Interestingly, in contrast to the results regarding hearing loss, anxiety sensitivity was not associated with awareness or loudness of tinnitus. This is likely because, as noted above, anxiety sensitivity is believed to predict subjective distress better than acoustical symptoms such as awareness and loudness of tinnitus. These results in part accord with several studies showing that anxiety-related temperament can influence tinnitus symptom severity.18202123 For example, Salviati et al.19 suggested that harm avoidance was associated with tinnitus symptom severity, and that individuals with high levels of harm avoidance tend to evade risky or harmful signals. Additionally, trait anxiety-defined as the tendency to react to situations that cause anxiety-was associated with tinnitus frequency in a sample of Korean patients aged 10-12 years.2036 However, anxiety sensitivity differs from trait anxiety in that it involves reaction to nonspecific somatic symptoms.2228 In fact, very few previous studies have evaluated the relationship between severity of tinnitus and anxiety sensitivity.232437 To our knowledge, this study is the first to establish a stronger link between anxiety sensitivity and subjective distress (e.g., annoyance, impact on life, tinnitus-related handicap) compared to auditory symptoms (e.g., awareness, loudness). Individuals with high levels of anxiety sensitivity might worry excessively about tinnitus or engage in negative cognitive appraisals of their experience of tinnitus. This implies that patients with high levels of anxiety sensitivity could benefit from a therapeutic approach that focuses on treating physical strain and irrational worry using cognitive behavioral or relaxation therapy. Additionally, cognitive behavioral therapy could relieve anxiety and depressive symptoms as well as tinnitus.3839
This study has some limitations. Because it was a cross-sectional study, no causality can be inferred from the findings. In addition, because the data regarding psychiatric symptoms were collected via self-report scales, we could not confirm diagnoses of psychiatric disorders. However, conducting structured psychiatric interviews with all patients with tinnitus would be time consuming in clinical settings. Further, as our sample comprised patients who had visited one otolaryngology clinic for treatment of tinnitus symptoms, it is possible that the proportion of patients with severe tinnitus or hearing loss was excessively high. However, the large sample size could have compensated for this bias to some extent. Finally, caution should be exercised in generalizing the findings to the general population of individuals with tinnitus.
In conclusion, the results indicated that high anxiety sensitivity and severe hearing loss were associated with increased tinnitus symptom severity. Furthermore, anxiety sensitivity was more likely to affect subjective distress and quality of life relative to awareness of tinnitus and symptom loudness. This finding implies that therapeutic approaches focusing on susceptibility to somatic sensation might help to alleviate tinnitus-related distress. Our findings also enhance our understanding of the multidimensional risk factors of tinnitus symptom severity, and thus could be taken into account in the management of patients with tinnitus.