INTRODUCTION
In our age, tools such as smartphones, computers and the internet have made technology a part of our lives, but the problems about using these tools can negatively affect the life of the user [1,2]. In relation to smartphones, effects such as inability to prevent excessive use, loss of importance of time spent without a smartphone, extreme irritability and aggression when not being with it, and progressive deterioration of the business, social and family life could be seen [3]. The excessive and psychosocially dysfunctional use of smartphones is increasingly emphasized in the literature, with aspects similar to behavioral addictions [1,4]. Although the concept of ŌĆ£problematic use of the smartphoneŌĆØ has been proposed on this subject, a terminological consensus has not yet emerged [5]. Various psychometric tools have been developed for smartphone addiction based on internet gaming disorder research in Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 [1,6]. Through these tools, the prevalence of smartphone addiction, especially among students, was found to be 12%-28% [7,8]. Based on these data, we preferred to use the concept of ŌĆ£smartphone addictionŌĆØ in our study.
On the other hand, internet gaming disorder, is defined by the World Health Organization (WHO)-2018 in International Classification of Diseases (ICD)-11 as lack of control over the game, increased priority given to the game, and continuation of playing despite its negative consequences. It is known that this disorder can have significant harmful effects on individuals such as depression, anxiety, stress, psychosocial problems, and low psychological well-being [9].
The most common reason for using smartphones of university students, who constitute the sample of our study, is to access internet-based applications [10,11]. Although smartphones provide easy access to large-scale information, excessive use can negatively affect young people psychologically, physically, academically, and socially. As a result, the early adult age group is exposed to a high risk of addiction [10,11]. Despite the completion of the intended use, inability to leave the phone, excessive time wasting and behavioral changes that develop together could be seen in relation to smartphone addiction, including changes in eating attitudes [10,11].
It was shown that excessive use or addiction of smartphones in this age group may lead to the problems such as depression and anxiety symptoms [12], decrease in sleep quality [10-12], deformation in emotional processing [13], signs of fatigue [14], and deterioration in academic performance [15]. Studies, which investigates the impairment of physical symptoms that may be associated with smartphone addiction, are limited [16,17]. Few studies of physical symptoms caused by smartphone overuse are about decreased physical activity and increased upper extremity pain due to use [17-19].
The typical characteristics of bad eating habits include irregular meals, snacks between the meals, dining out as a routine, and eating quickly. In general, it is known that these habits are affected by many factors such as family, peers, and media [20]. It has been determined that eating disorder behavioural changes were seen along with alcohol and drug using disorders, this has suggested that the neuro-biological pathways such as addiction-related medial prefrontal cortex (mPFC) and nucleus accumbens (NAc) may have an impact on eating attitudes [21]. Majority of the studies examining the behavioural addictions about the eating attitudes have focused on internet addiction [22,23]. Although there are limited studies examining the smartphone usage and bad eating habits [4,24] and addressing the eating disorders with internet and smartphone addiction together [25]. The results regarding the use of smartphones among university students in Turkey indicate that it has become a serious problem. The limited data of the few studies in Turkey on alters in eating attitudes, which can be considered as one of the negativities associated with behavioral addictions, have caused us to pay attention to this issue [26]. In this context, investigating the effects of smartphone addiction on eating attitudes seems to be an area worth studying.
Based on this information, we established the hypothesis that smartphone addiction and online game addiction may affect eating attitudes and pave the way for obesity. For this purpose, 358 university students who accepted to participate in the study filled the Eating Attitude Test (EAT), the Short Form of The Smartphone Addiction Scale (SF-SAS), and the Short Form Internet Game Disorder Scale (SF-IGDS9), results were statistically analyzed and discussed.
METHODS
Sample
The sample of this research in cross-sectional type, is consisted of the university students, who have been invited to the study between the months of June and December 2018, continued formal education among the students of University of Health Sciences and Marmara University regardless of departments. The study was carried out by Sultan Abdulhamid Han Training and Research Hospital Psychiatry Clinic. 680 persons, who have applied to our clinic with reasons other than psychiatric examination (as intern, medical board report, etc.) were invited to the study. 448 volunteer university students, who have accepted to participate in the study, were given the questionnaire form and requested to fill it. As a result, 358 patients, who have filled in the form completely, and whose consents have been obtained, are included to the study.
1) Being volunteer, 2) being smartphone user at least for the last six months, 3) completing the forms in full, and 4) being a formal university student currently, were determined as the criteria of being included in the study.
Process
The data was collected with standardized, no-name, self-report data collection questionnaires. Personal information and smartphone using information were questioned for all volunteers with socio-demographic form. SF-SAS was administered in order to examine the state of smartphone addiction and EAT was administered in order to determine the eating attitudes of all participants. In addition, SF-IGDS9 was administered to those participants playing games regularly. According to the participantsŌĆÖ EAT scores (if higher than 30), they were subjected to a mental examination and those with eating disorders were excluded from the study. Anthropometric measurements of the participants were made by the clinicians. Body mass index (BMI, weight/height2) was used in assessing the nutrition states of the persons. Those having a BMI below 18.5 were considered as ŌĆ£underweight,ŌĆØ having a BMI between 18.5 and 25 were assessed as ŌĆ£normal weight,ŌĆØ having a BMI between 25 and 30 were considered as ŌĆ£overweight,ŌĆØ and having a BMI above 30 were considered as ŌĆ£obese.ŌĆØ [27] In the study, the groups adjusted according to BMI were provided as ŌĆ£body weight groups.ŌĆØ The collected data were recorded into the data set and analysed duly.
The study was approved by Zeynep Kamil Training and Research Hospital Ethics Committee (IRB: 2018/215). All stages of the study and protection of the participants were carried out in accordance with Helsinki Declaration. All participants provided informed concent.
Data collection tools
Socio-demographic data of the participants including age, weight, height, BMI, gender (female, male), school year, faculty type (medical-dentistry, fac. of science and literature, fac. of economics administrative sciences, fac. of engineering, fac. of health sciences), economis status (low, medium, high), person living with (family, friend, hostel, single), smartphone usage information (age of having first mobile phone, monthly mobile phone invoice) were evaluated.
Short Form of Smartphone Addiction Scale (SF-SAS) was used in order to assess the state of smartphone addiction of the participants included in the study. The scale was consisted of 10 items in 6-point Likert type. The score range, which may be achieved from the scale, varied between 10 and 60. The Turkish validity and reliability study of the scale, which has been carried out by Noyan et al. [28], was developed by Kwon et al. [29] According to Kwon et al. [29], Ōēź31 and Ōēź33 were identified as the cut-off values of smartphone addictions respectively for male and female participants [28]. The Cronbach alpha value of the scale was found to be 0.854.
Eating Attitude Test (EAT) was used in order to identify the eating disorders of the participants. It was developed in 1979 by Garner and Garfinkel [30]. The Turkish validity and reliability study was carried out by Sava┼¤─▒r and Erol [31]. Cut-off point of the scale was determined as 30. The scale was consisted of 40 items in 6-point Likert type. Maximum 3 points can be achieved from each question in the scale (120 points in total). The cut-off point for eating attitude disorder was determined as 30 [30,31]. The Cronbach alpha value of the scale was found to be 0.877.
Short Form of Internet Game Playing Disorder Scale (SF-IGDS9) was used to question the participantsŌĆÖ state of playing games within the last one year. The scale, which is consisted of 9 items, is a 5-point Likert type self-report type scale. The The Turkish validity and reliability study of the scale, which has been carried out by Evren et al. [32], was developed in 2015 by Pontes and Griffiths [33]. The cut-off point was determined as 36. The Cronbach alpha value of the scale was found to be 0.846.
Statistical analysis
Data analysis was carried out by using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). The numerical variables were provided as average┬▒standard deviation, and the categorical variables were provided as frequency and percentages, after the descriptive analysis was carried out, in order to examine the socio-demographic characteristics (gender, age, education status) of the participants. In order to determine whether the parametric or non-parametric tests would be used or not, initially the conformity of the normal distributions was determined with Kolmogorov Smirnov Test. Student t test was used for the variables, which were in compliance with the normal distribution. Chi-square test was used in order to compare the difference of the categorical variables. In addition, linear regression model was developed in order to identify the predictors of Eating Attitude Test, considering the literature information and primary statistical data. The statistical significance p values were deemed as equal to 0.05 or less.
RESULTS
Our sample was consisted of 214 female (59.8%) and 144 male (40.2%) participants. The mean age of the participants was calculated as 22.27┬▒3.10 years, and average BMI was calculated as 22.34┬▒3.61 cm /kg2. A statistical difference was determined between the variables of BMI, body weight, faculty of the student, familyŌĆÖs economic status, and persons living with, between the groups with and without smartphone addiction (respectively; p values 0.047, 0.044, 0.017 0.001, and 0.030). There were no one, who has received eating disorder diagnosis, in the psychiatric assessment of the participants, who has achieved >30 points in EAT, carried out according to DSM-5. Thus, the diagnosis of anorexia nervosa was initially excluded. Any statistical differences were not found between the groups in terms of the variables of age, gender, height, and school year (duration of education) (p>0.05). Socio-demographic data of the participants and the comparison between the two groups are presented in Table 1.
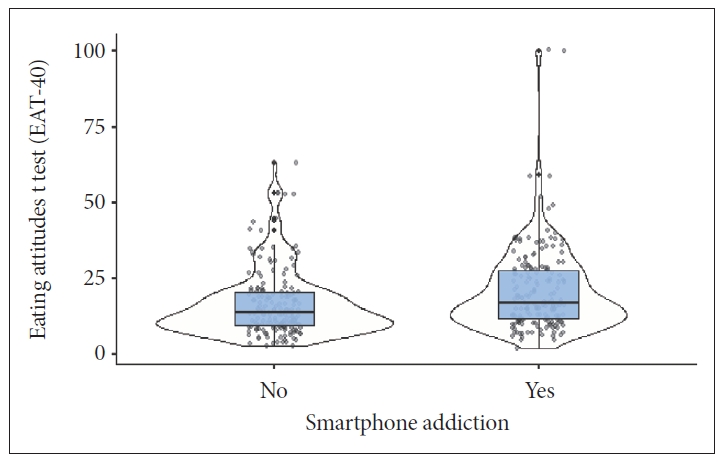
While a significant difference was determined between the monthly mobile phone invoices, EAT scores (Figure 1), and SF-SAS scores of the groups with and without smartphone addiction (respectively; p=0.004, p<0.001, and p<0.001); any statistical differences were not determined between the scores of age of first mobile phone and game addiction (p>0.05) (Table 2).
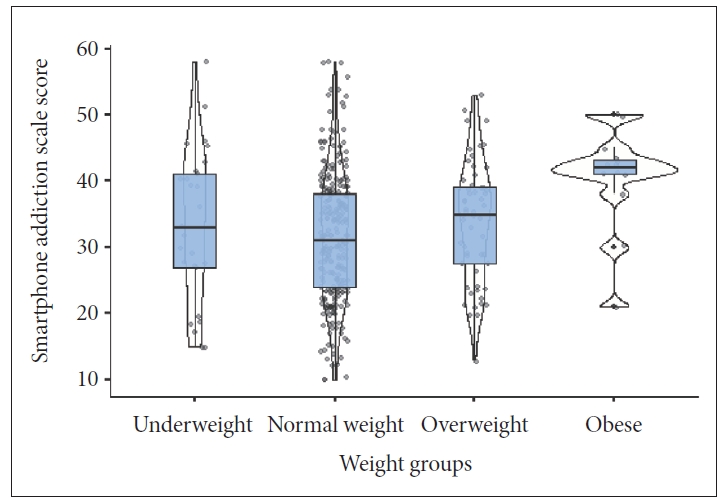
Statistical comparison of EAT and SF-SAS scores according to BMI of the participants are presented in Table 3 and Figure 1. Statistical difference was found between both EAT and SF-SAS scores between the groups. According to BMI, SF-SAS scores of the obese group were determined as higher compared to the normal group, furthermore, EAT scores of the overweight group were also determined as higher than the group with normal weight (respectively; p=0.004 and p=0.05) (Figure 2).
In addition, the EAT predictors were tested with the linear regression analysis in Table 4. In the linear regression model, in which the variables of age, gender, smartphone addiction, BMI weight groups, school year, age of first mobile phone, and familyŌĆÖs economic status were addressed together, the values were determined as F=3.551 and p=0.001. According to the model, variables of gender (p=0.038), smartphone addiction (p=0.005), and school year (p=0.010) were found as the predictors for EAT. However, variables of age, weight groups, age of first mobile phone, and familyŌĆÖs economic status were not determined as predictors.
DISCUSSION
In our study, the relationship of eating attitude behaviors with smartphone addiction and internet gaming addiction was investigated. The most important finding of our study, smartphone addiction brings about changes in eating behaviour and smartphone addiction would be a precursor of an eating disorder. Furthermore, we found a significant difference between BMI and smartphone addiction, is another important finding of our study. In addition, any relations were not found between online gaming addiction and eating attitudes. We think that the results of our study are important, as it reveals the physical consequences of smartphone addiction and as it is a guide for the measures to be taken in struggling with smartphone addiction.
Smartphone addiction causes various changes in eating attitudes, in addition to the psychological and social results. The vast majority of the researches on digital addictions and eating attitudes have addressed the internet addiction [25,34,35]; there are very few studies on smartphone addiction [25,36]. Our study showed that EAT score, body weight, and BMI were higher in the individuals with smartphone addiction, as supporting the limited information in the literature. Furthermore, it has been seen that smartphone addiction was a predictor of EAT score. In research supporting this result, the prevalence of smartphone addiction in obese individuals was found to be high [37], in addition it was determined that the increase in addiction rates was associated with the increase in BMI [36]. Among the possible causes, first of all, the relationship between smartphone addiction and behavioral changes such as fast eating and snacking should be considered [23]. Spending a long time with a smartphone leads to a relatively sedentary life. In order to prolong the time spent in front of the screen, behavioral changes occur such as turning to easily prepared, high-calorie foods or skipping meals with snacks [24,38]. This situation increases the amount of calories taken and decreases the amount consumed, which paves the way for weight gain and obesity. In addition, the decrease in eating awareness related to distraction is one of the reasons for the inability to regulate eating in individuals with smartphone addiction [25]. Today, especially in the young population, social relationships established through social media and the emotional consequences of these relationships such as excitement, anxiety and sadness can also affect eating behaviors. In addition, body image, which is considered important in the young age group, and the resulting social pressure may also cause changes in eating attitudes. A study conducted with university students in Korea found negative eating behaviors such as skipping breakfast frequently, preferring irregular diet and processed foods, overeating and skipping meals in those who use smartphones at a high rate [39]. It has been observed that students who reduce the time they use smartphones return to healthy food choices and eat regularly and on time [39]. A study conducted in the child age group found that students who spend more than 2 hours a day on a smartphone allocate more financial resources for snacks (ice cream, junk food and carbonated drinks) [4]. In another study, it was observed that physical activity decreased, sleep disorders and meal skipping rates were high in those with excessive use [16]. Considering the possible reasons, smartphone addiction might be deemed as a possible risk factor for impaired eating attitude, obesity, and excess weight. Here, when it is considered that smartphone usage is a dispensable part of life and how much the time allocated to it within the daily time, the necessity for taking precautions in order to be protected from obesity, which shall be an important health problem in future, is explicitly revealed.
In our study, online game addiction was not found to be high in individuals with smartphone addiction, this information has not been reported in the literature before as far as we know. This result may indicate that although the smartphone device has many functions, it is less used for gaming due to insufficient technical features [10]. Although there are similar points between internet addiction and game addiction behaviors in the literature, it has been shown that there are different types of behavior [40]. According to our results, it can be thought that online game addiction has different characteristics from smartphone addiction. The relationship between online gaming and smartphone use needs to be clarified.
Furthermore, it has been revealed in our study that smartphone addiction and being male and increase of education duration (school year) were precursors for eating attitude score. Internet addiction and BMI were also found to be higher in male gender [22]. Education duration (school year) is associated with age increase and the period spent in pupillage, for this age group, this result is ordinary.
In our study, it has been found that smartphone addiction of the students living with their families was lower. Addiction rates of those living alone, staying at the hostel, and particularly living with their friends, were higher. This result is consistent with the literature [41]. This may be explained with the low level of anxiety in individuals living with their family, and the thoughts that smartphones reduce loneliness concerns in individuals due to providing continuous connection to the social platforms and internet [42]. In our study, addiction rates might have been found low due to the social support providing and anxiety level decreasing aspects of living with family. In addition, our study has revealed that there was a difference between the faculty type, in which the participants receiving education, and smartphone addiction rates. The literature demonstrates contradictory results in this subject [10,35]. The relation of the education field with the behavioural technologic addictions is not known clearly. The relationship between the field of education and behavioral addictions is not clearly known, and the effect of education on behavioral addictions is an area worth examining.
The most important strength of our study is that it was conducted with a homogeneous group of two university students. The sufficient number of samples is another strength of the study. In addition, performing a psychiatric examination and anthropometric measurements by the clinician is another strength of the participants. The results of our study must be addressed within some limitations along with the strengths. First of all, the fact that the study was carried out on the university students is an obstacle for the generalization of our results. The studies, which shall be carried out with the individuals in different age groups and education levels, shall ensure the results be more reliable. Second, the fact that self-report scales have been administered to the participants, caused the results to be open to the manipulation of the participants. The fact that the height and weight of the participants are based on the information of the participants, may cause suspicion on some results.
As a result, smartphone addiction associated with eating attitude disorders, body weight, and obesity. It should be noted that the use of smartphones may lead to physical diseases, which we shall encounter in future, and struggling strategies should be determined. It is important to inform all age groups about the benefits and harms of smartphone use. Behavioral methods such as management of use, limiting the smartphone using, spending time with other objects that can replace smartphone could be used. Particularly, directing the youth to sports and arts activities, which increase self-confidence and provide motivation, may encourage them to establish face-to-face social relations. Programs that describe the harmful effects of smartphones in the media can be effective. In order to understand and manage the relationship between eating attitudes and behavioral addictions, there is a need for future technology-followed studies with samples covering a wide range of age and education levels.