INTRODUCTION
Disrupted-in-Schizophrenia 1 (DISC1) and DISC2 genes are located at the breakpoint of a chromosomal translocation at 1q42.1 (1;11) (q42.1;q14.3), which was firstly described to be linked to major psychiatric disorders, including schizophrenia, in a Scottish family.1 Subsequent studies on different ethnic populations provided further evidence supporting the role of DISC1 as a susceptibility gene for Schizophrenia spectrum disorders.2,3,4,5,6,7,8,9,10,11,12
The biological functions of DISC1 are not completely understood, and still there is no clear knowledge on how variations in DISC1 gene could increase the risk of schizophrenia. However there is growing evidence regarding the involvement of DISC1 protein in neurodevelopmental processes and neural cell signalling through its interaction with the binding protein complex known as DISC1 interactome; being FEZ1, NEDL1, PDE4, or PSD95 among the proteins included in this complex.13,14
During the last decade, the study of the relation between DISC1 and different schizophrenia endophenotypes (e.g., brain structure and function, cognitive abnormalities), has provided evidence of association between variations in several DISC1 polymorphisms and brain structure, altered brain function and impaired cognitive performance, both in schizophrenic patients and in healthy subjects.4,5,15,16,17,18,19,20,21,22 However, few studies have examined the relationship between this gene and the clinical presentation in schizophrenia.11,23,24,25 These studies have reported associations between different DISC1 polymorphisms and positive psychotic symptoms -hallucinations and delusions-,24,25 as well as psychosis-related traits both in schizophrenic patients and in healthy individuals.11,23 However none of these studies have examined a sample of first-episode patients, thus allowing to control the confusion effects derived from the treatment and chronicity of the illness.
Among all the numerous DISC1 polymorphisms which have been described, the Ser704Cys (rs821616) appears to be especially relevant as it has been previously related to different aspects of schizophrenia. Specifically, variations in this particular polymorphism have been associated not only to the risk of having schizophrenia,7 but also to several endophenotypes, such as brain structural and functional abnormalities,7,15,18 cognitive impairment,7,17,20 and even clinical presentation.23,25 All these studies have found that carriers of the Ser allele (or Ser/Ser genotype) have an increased risk for showing a higher severity of the different abnormalities mentioned above.
The aim of the present study was to examine, in a well-characterized and representative series of patients experiencing a first episode of a non-affective psychosis, whether an association between DISC1 Ser704Cys polymorphism and clinical presentation exists. We hypothesized that carriers of the Ser allele (or Ser/Ser genotype) will show a more deleterious illness onset, with an earlier age of onset and higher psychopathological severity.
METHODS
The sample for the present study consisted in 213 unrelated Caucasian subjects of Spanish origin. The subjects formed part of a large prospective longitudinal study on first episode non-affective psychosis (PAFIP).26 Those patients referred to the program presenting a first episode of non-affective psychosis were admitted to the programme if fulfilling the following criteria: 1.-aged 15-60; 2.-meeting DSM-IV criteria (by means of the Structured Clinical Interview for DSM-IV, SCID-I) 6 months after inclusion for a principal diagnosis of, schizophrenia, schizophreniform disorder, schizoaffective disorder, brief reactive psychosis, delusional disorder, or psychosis non otherwise specified; 3.-habitually living in the catchment area; 4.-no prior treatment with antipsychotic medication; and 5.-current psychotic symptoms of at least moderate severity, as assessed by one of the five items of the Scale for the Assessment of Positive Symptoms (SAPS). Patients were not admitted to the programme if presenting any of the following: 1.-mental retardation; 2.-neurological disorder; or 3.-drug dependence (DSM-IV criteria).
Clinical assessments were carried out with the Scale for the Assessment of Positive Symptoms (SAPS),27 Scale for the Assessment of Negative Symptoms (SANS),28 and the Clinical Global Impression-Severity scale (CGI-S), by a senior psychiatrist (BC-F), who was blind to genotype. The positive, negative and disorganized symptom dimensions were calculated from SAPS and SANS scales,29,30 and were used to measure the clinical severity of the illness. The positive symptom dimension is the sum of global scores for the SAPS items hallucinations and delusions. The negative symptom dimension is the sum of global scores of the following SANS items: alogia, affective flattening, avolition-apathy, and anhedonia-asociality. And the disorganized symptom dimension is the sum of the items: positive formal though disorder, disorganized/bizarre behaviour, and inappropriate affect.
All subjects gave written informed consent prior to their inclusion in the study, which was approved by the local ethics committee (University Hospital Marques de Valdecilla Ethics Committee).
The control group, which consisted in 303 subjects, was obtained from the Blood Bank of the University Hospital Marques de Valdecilla. All subjects in the control group gave consent for their blood to be genotyped for research purposes.
Genomic DNA was extracted from peripheral white blood cells obtained from each subject according to standard protocols. The Ser704Cys DISC1 polymorphism-rs821616-was genotyped using SNPlex technology (Applied Biosystems, Foster City, CA, USA).
All statistical analyses were carried out using the statistical software package SPSS 15.0 for Windows. For the analysis of categorical variables, Chi square analyses were carried out. For the analyses of the relation between Ser704Cys genotype and continuous variables, we used analysis of variance (ANOVA) tests. Statistical significance was established at p<0.05.
After completing the association analysis by genotype, and in order to facilitate comparison to previous studies, we conducted exploratory analysis of association clustering the patients into two groups according to being homozygous for the Ser allele or carrying the Cys allele.
RESULTS
Gender distribution was 123 males (57.7%) and 90 females (42.3%). Mean age of onset in our sample was 27.3 years (SD=7.8), higher than what has commonly been reported. The mean duration of untreated psychosis (DUP) at initial assessment was 14.5 months (SD=29.4, median=4).
Among the control group, 177 (59.8%) were male, and 126 (41.6%) were female. Due to the origin of the control sample, sex was the only socio-demographic variable available for the current study.
The diagnostic breakdown of the patients was: schizophrenia (n=121, 56.8%), schizophreniform disorder (n=52, 24.4%), schizoaffective disorder (n=5, 2.3%), brief reactive psychosis (n=18, 8.5%), psychosis not otherwise specified (n=15, 7.0%), delusional disorder (n=2, 0.9%).
Patients and controls were in Hardy-Weinberg equilibrium for the polymorphism studied. Rs821616 genotypic and allelic frequencies were as follow for patients and controls. Patients: AA=6.6%; AT=42.7%; TT=50.7% and A=0.28; T=0.72. Controls: AA=8.6%; AT=37%; TT=54.4% and A=0.27; T=0.73.
Gender distribution did not significantly differ between patients and controls (Ï2=0.21; p=0.35). Moreover, gender distribution both in patients and controls was similar in each of the genotype groups (Patients: Ï2=3.52; p=0.17; Controls: Ï2=4.13; p=0.13 respectively).
Allelic and genotypic distributions were not significantly different in patients and controls (Allelic: Ï2=0.09; p=0.76; Genotypic: Ï2=2.04; p=0.36). In the group of patients with psychosis, the statistical analyses failed to show any significant association between Ser704Cys genotypes and age of onset or DUP (Table 1).
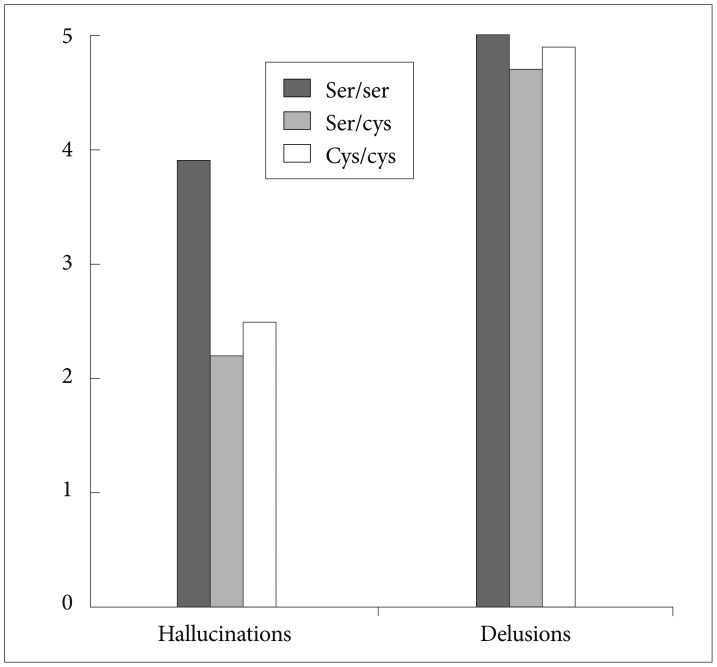
When the three commonly used dimensions of psychopathology (positive, negative and disorganised) were analysed, a significant association was found between Ser704Cys genotype and the positive dimension (Table 2); those patients homozygous for the Ser allele showed a higher severity of the positive dimension than Cys allele carriers (F=6.85; p=0.009) (Figure 1). In a further analysis we explored each of the symptoms included in the SAPS-SANS positive dimension, finding a significant association between Ser704Cys genotype and the item hallucinations (F=5.75; p=0.017) following the same direction as the previous result; patients with a Ser/Ser genotype showed a mean greater score than Cys carriers (Figure 2).
DISCUSSION
Our study detected a significant association between Ser704Cys genotype and severity of positive psychotic symptoms in a well-defined Spanish Caucasian population, measured by the total score in the SANS-SAPS Positive Symptoms dimension, and severity of the Hallucinations, at the onset of the illness. Thus, according to the results, a patient presenting a first episode of psychosis and being homozygous for the Ser allele will present more likely a worse clinical onset of the illness, with more severe positive symptoms and particularly hallucinations.
This finding is consistent with previous reports of an association between carrying the Cys allele and presenting lower delusional rating in psychotic patients,25 and lower rates in the schizoidia scale in healthy subjects.23
Other studies linked as well clinical presentation to different DISC1 polymorphisms; thus Hennah et al.11 described that a certain DISC1 haplotype (HEP3) displayed association to certain component-traits of Schizophrenia. And similarly another study found an association between the phe allele in leu607phe SNP and severity of hallucinations in a sample of Caucasian patients with a diagnosis of schizophrenia.24
Moreover, a recent study acknowledged the possibility that the severity of the psychosis could be the mediating factor in the observed association between a DISC1 rs3738401 variant and ultra-resistance to antipsychotic treatment.31
Although DISC1 gene has been postulated as one of the main candidate genes for Schizophrenia, to date there is no clear evidence supporting the Ser704Cys DISC1 SNP as a risk factor for psychosis. While Callicot and colleagues found the Ser allele over-transmitted to psychotic patients in a large family-based sample,7 a recent study found no association between this polymorphism and the risk of psychosis.25 In line with these results, our study showed no significant association between Ser704Cys polymorphism and risk of psychosis in the northern Spanish Caucasian population studied.
In addition, when studying the effect of this DISC1 genotype on the onset of the illness our study found no association between Ser704Cys polymorphism and age of onset or DUP. This last result is in agreement with a previous study in a sample of schizophrenic Japanese patients.42
The biological function of DISC1 is not completely understood, and yet still there is no clear knowledge on how variations in DISC1 gene could modify the clinical presentation of the illness. However, it is today established that DISC1 gene encodes for a scaffold protein that interacts with multiple proteins (DISC1 Interactome) involved in neurodevelopment and neuro-signalling processes.32,33,34,35
DISC1 protein is expressed in neurons in the brain, predominantly in the hippocampus and cerebral cortex.36 DISC1 expression has been shown to be lower in patients with Schizophrenia.37 And moreover, those schizophrenic patients Ser homozygous for Ser704Cys DISC1 polymorphism showed a lower expression of some of these partner proteins in these brain areas.38
Moreover, Ser/Ser genotype has been associated to a decrease in hippocampal grey matter and to abnormal hippocampal activity during cognitive tasks.7 And, in healthy subjects Ser/Ser genotype showed greater activation of the hippocampus15 and pre-frontal cortex16 during cognitive tasks, suggesting that these areas needed greater activation to achieve the same level of cognitive functioning of those Cys carrier subjects.
Interestingly, these two brain areas -prefontal cortex and hippocampus- showing structural and functional changes in relation to variations in DISC1 gene, play a central role in the genesis of psychotic symptoms according to the dopamine theory of Schizophrenia.39,40 Therefore a plausible explanation for the involvement of DISC1 in psychosis severity is based on its interaction with the dopamine system, perhaps through neurodevelopmental modifications in these brain areas derived from DISC1 gene variations which could ultimately lead to the functional and structural changes described in these two main brain areas as well as differences in clinical severity.
Indeed, a recent review on DISC1details the multiple findings relating DISC1 variations to dopamine system in knock-down mice and cell studies,41 in line with this explanatory hypothesis.
These results have to be taken into account with caution; the study should be replicated in larger samples and other DISC1 polymorphisms should be included in the study forming haplotypes to obtain a bigger representation of the DISC1 gene.
The sample used in this study, formed by a wide range of non-affective psychosis diagnosis might be a caveat in the study as the results obtained might be less specific of a core schizophrenia diagnosis sub-sample. However, this study aimed to identify associations between variations in DISC1 gene and clinical severity of the onset of psychosis in a wide scope, and not in a more restricted sample.
The genotype clustering (Ser homozygous versus Cys carriers) carried out in order to facilitate comparison to previous studies, formed two unbalanced groups, which may have influenced the subsequent statistical analyses, therefore representing a possible caveat. However, due to the exploratory nature of this analysis we have considered relevant to include it.
An additional flaw in our study could be the multiple tests done. After correcting for multiple testing the statistical significance didn't survive. However this might be explained by the sample size and it is likely that in a bigger sample the statistical significance would have survived multiple testing corrections.
In conclusion, this study showed a significant association between DISC1 gene Ser704Cys polymorphism and severity of the positive symptoms, in particular hallucinations, at the onset of a first episode of psychosis. Therefore, DISC1 gene variations may modulate the severity of the psychosis at the onset of the illness.