INTRODUCTION
The effect of religion on mental health has long been debated and remains controversial despite some positive findings in reviews of empirical research.1-4 The most plausible explanation of these mixed results is that the relationship between religion and mental health is not robust and is sensitive to the definitions adopted, the measures employed, and the samples studied.5
Although many studies have been conducted on mental illness among people with different religious affiliations, almost all have focused on Christian denominations. Therefore, few studies have explored the association between mental health and religiosity across a wide variety of types of religious believers.
Although the last Korean dynasty was based on Confucianism, which had been imported from ancient China approximately 700 years ago, most Koreans adopted Buddhist beliefs until the early 20th century. However, the Christian population, including Protestants and Catholics, has increased in the past several decades, and Christianity has now become the most popular religion in Korea. Nonetheless, the proportion of atheists remains substantial because religion is not obligatory in Korean society. Another factor affecting religious adherence is the negligible number of minor religious groups among Korean nationals, which reflects the ethnic homogeneity of the country.6
Spirituality can be defined as a personal quest for understanding answers to ultimate questions about life, meaning, and the relationship with the sacred. Because religious practices and rituals differ, spirituality may be associated with mental health, regardless of the type of religion.7
The aim of this study was to compare the rates of three psychiatric disorders (major depressive disorder, anxiety disorder, and alcohol use disorder) according to type of religion or spiritual values in a nationwide sample of Korea.
METHODS
Data collection
The Korean Epidemiologic Catchment Area study was conducted between June 1 and November 30, 2001 to collect mental health-related information about the Korean population aged 18-64 years living in private dwellings. This survey utilized the diagnostic definitions in the DSM-IV8 and the Korean version of the Composite International Diagnostic Interview 2.1 (K-CIDI 2.1).9 The frequencies of mental disorders were transformed by weighting and adjusting the data to approximate the national population contributors of age and gender in each catchment area, as defined by the Korean National Statistical Office's 2000 census.6 More detailed information on this epidemiologic survey has been previously described.10
Study measures
Past and current mental disorders
A current mental disorder was defined as the occurrence of an episode that met the diagnostic criteria of any mental disorder during the preceding 12 months. In addition, the term "past mental disorder" was used to categorize cases with a lifetime history of any mental disorder that fulfilled the diagnostic criteria but with no episodes during the preceding 12 months.
Type of religion and spiritual values
We asked the respondents two questions: "What is your major religion in most of your life?" and "How much have spiritual values played an important role in your life?" Spiritual values were evaluated using quartiles of one (none) to four (high).
Minor religions were excluded in the analysis due to cell sizes below five.
Statistical analysis
Group differences in the sociodemographic variables and the stated importance of spiritual values were computed using the chi-squared and ANOVA tests We also applied logistic regression models to determine the lifetime, one-year, and past odds of mental disorders based on the type of religion, using "atheist" as the reference category. Each mental disorder was analyzed separately and adjusted for age and sex. In addition, a series of logistic regression analyses derived odds ratios and 95% confidence intervals using the past or current mental disorders as the main outcome variables and DSM-IV SP and spiritual values as the predictor, after adjusting for age, sex, and type of religion. All statistical analyses were conducted using SPSS version 14.0.
RESULTS
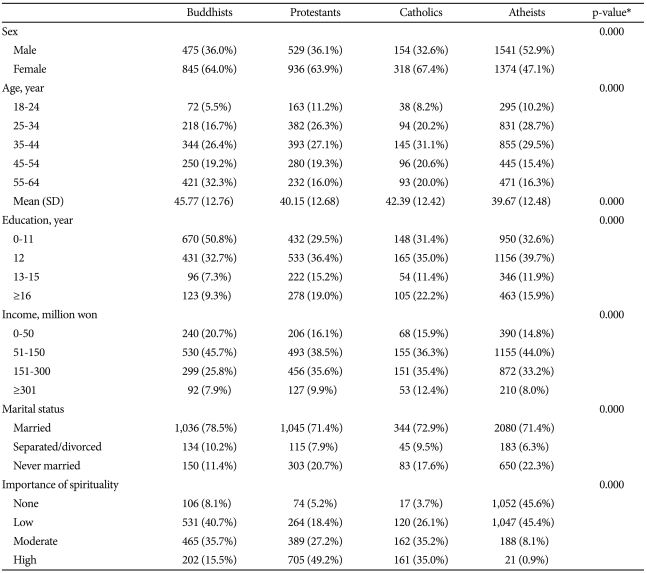
Sociodemographic profiles according to type of religion
Universally, females reported more religious affiliation across three religious groups (64.0% for Buddhism, 63.9% for Christianity, and 67.4% for Catholicism) than males. Buddhism was more popular among older, less-educated, and lower-income individuals.
Spiritual values were higher among Christians than among Buddhists (Table 1).
Prevalence of mental disorders by type of religion
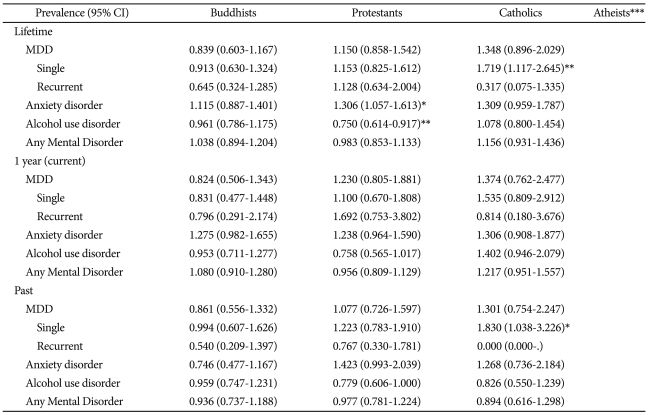
The lifetime prevalence of a single episode of major depressive disorder was higher in Catholics than in atheists. Moreover, the lifetime prevalence of anxiety disorder was higher in Protestants and Catholics than in atheists. In contrast, the lifetime prevalence of alcohol use disorder was lower in Protestants than in atheists. There were no significant differences between the types of religion in either the lifetime or the one-year prevalence of any mental disorder (Table 2). After controlling for sex and age, we compared the odds ratios for prevalence of lifetime, one-year, and past disorders according to type of religion, using "atheist" as the reference category.
Protestants had higher ORs for lifetime anxiety disorder and lower ORs for lifetime alcohol use disorder. Catholics had higher ORs for lifetime and past prevalence of single episodes of major depressive disorder but not for one-year prevalence (Table 3).
Association of current and past mental disorders with spiritual values
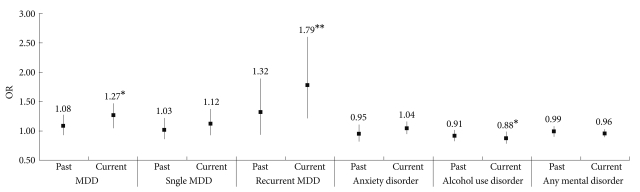
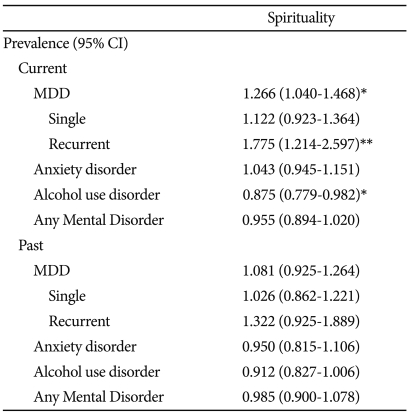
The results of the logistic regression analysis indicate that stronger spiritual values were associated with higher odds of suffering current depression (Table 4).
Conversely, there was a significant negative correlation between the odds ratio of alcohol use disorder and the reported importance of spiritual values. There were no significant differences in the prevalence rates of past mental disorders according to spiritual values (Figure 1).
DISCUSSION
This study revealed two important associations between mental disorders and spirituality. We confirmed that attaching high importance to spiritual values was associated with a higher prevalence of current depression, irrespective of causality. In contrast, a higher importance placed on spiritual values was also associated with less current alcohol use disorder. These results are similar to those of a previous Canadian study that analyzed mental disorder prevalence data using the CIDI.11 However, our study did not confirm any associations between spirituality/religion and past mental disorders or indicate any significant relationship between anxiety disorder and spiritual values.
Positive associations between mental disorders and spiritual values have been interpreted in two ways.12 The first perspective is that strong spiritual values are often associated with and may lead to a high prevalence of mental disorders. The other assumption is that mental illness leads individuals to seek spirituality and religion to help manage their psychological issues. To elucidate the causal relationship between mental disorders and religion/spirituality, we referred to individuals who had experienced one or more mental disorder episodes within the 12 months prior to the study but who did not meet the diagnostic criteria for a current psychiatric disorder as having a past disorder.11 Our findings that spirituality is associated with current depression, but not with past depression suggest that individuals with currently high levels of depression have a stronger tendency to place more importance on spiritual values, but the individuals who had overcome past depression does not. In other words, a depressive episode motivates patients to seek out God and religion as a way of coping with their illness. Several studies have suggested that religious activities, such as worship attendance, may play a role in combating depression.11,13
Because we did not include worship frequency, which is associated with different types of belief in God across religions, our study provides no information on how religious activity is related to depression. However, we can posit that current depression can result in people placing a high importance on spiritual values regardless of the frequency of their attendance at religious services. It is natural that a serious illness could cause an individual to seek spiritual support.11
Strong spirituality was associated with a significantly lower odds ratio of current alcohol use disorder. This pattern differs from those observed for current major mental disorders. These results are in accordance with prior studies indicating that a high level of religious involvement predicts a reduced risk for alcohol misuse.14,15 It is not difficult to understand that when individuals are currently under the influence of alcohol, it is unlikely that they are able to reframe what is happening to them in terms of spiritual values.11 Negative relationship between alcohol misuse and spiritual values is also supported by our finding that the highest levels of alcohol use disorder were in atheists.
The associations between religion/spirituality and anxiety disorders were insignificant and similar to those of prior studies.11,15,16 Though we did not analyze the data by dividing anxiety disorders into panic disorders, social phobias and similar categories as prior studies have, we found no significant association between spiritual values and anxiety disorder, both current and past. We do not know whether anxiety is unassociated with spirituality, but anxiety disorder might be regarded as less severe than depression in terms of prompting a search for meaning or an understanding of hardships through spiritual values.16 However, this interpretation should be approached with caution because of the overlap between depressive and anxiety symptoms.
There have been epidemiological observations that members of some religious groups appear to be at elevated risk for certain mental disorders.17 However, because almost all of these studies used a Christian population as their baseline, we cannot apply their conclusions to other countries that have different religious compositions. By using atheists as a reference point, our study revealed that religious affiliation is associated with the prevalence of mental disorders in several ways. The meaningful results are as follows: First, there were no significant differences in the rates of current mental disorders of religious affiliation group regardless of type of religion compared with the no affiliation group. Second, a past history of a single episode of depression was statistically meaningful only in Catholics. Third, Protestants presented a higher lifetime prevalence odds ratio for anxiety disorder and a lower odds ratio for alcohol use disorder compared with atheists.
The unadjusted prevalence data indicate that the highest lifetime prevalence for a single episode of depression was associated with Catholic religious affiliation. In contrast, the same group had the lowest lifetime prevalence of recurrent depression, though the difference was not significant in the logistic regression analysis. Because we have no information regarding the timing of the onset of depression and the entry into religious life, it is not clear whether depressed persons are eager to become Catholics. However, the significant association of Catholicism with past depression leads us to a particular interpretation. Catholic beliefs, for example, may have a healing effect on depression or may prevent a relapse. This hypothesis is supported by the absence of a significant current ethnic religion affiliation among Koreans, who are allowed to freely select their own religious beliefs. In other words, their religion might not be determined by their parents but rather by the individuals themselves; therefore, there is a tendency to become involved with religion with increasing age.
The lower odds ratio of lifetime alcohol use disorder in Protestants is relatively easy to explain18 in terms of the tenets of many Protestant religious beliefs that aim to restrain adherents from drinking alcohol, though the observance of this restriction may vary between individuals. This hypothesis is supported by a comparison with Catholics, who are relatively lenient toward drinking according to our results. Though the odds ratio for current alcohol use disorder in Catholics compared with atheists was not significant, the upper limit of the 95% confidence interval was 1.000. Studies that have defined "religious" as adherence to Christian tenets have unanimously found that religious individuals are less likely to abuse alcohol.4
The lifetime prevalence of anxiety disorder was higher among this survey's Protestant respondents compared with the atheists. People with anxiety disorder may attend church to relieve anxiety. In contrast, some Christian doctrines, such as the belief that people are born with original sin, may evoke anxiety among believers. Inconsistent with our results, a previous study has reported a high rate of anxiety disorder among young adults with no religious affiliation.16
Our study has several limitations. First, although we examined a large, nationally representative population using the K-CIDI 2.1, this was essentially a cross-sectional study. Therefore, our choice to divide lifetime prevalence into current and past prevalence was based on incomplete evidence used to infer temporal associations between mental health and religious beliefs/spirituality. More valid and rational explanations concerning directionality need to be explored in prospective studies of large, general populations. Second, we only evaluated spirituality in one survey question. Because of the different cultures and rituals across religions, we predicted that this method would provide a more tailored approach to elucidating the association between religion and mental health. Nonetheless, we question whether our study evaluated the correct "spirituality" because measures of spiritual values are not well established.19 Third, although we controlled for sex and age, many confounding variables were not explored, such as cultural factors, family experiences, and environmental factors.
The results of our study may reflect the possibility that a depressive episode motivates people to search for spiritual meaning or the power of God. Spirituality might not have been as highly regarded when the individual first became depressed, but over time, spiritual values may help an individual overcome depression or become less vulnerable to relapse. However, this interpretation fails to provide firm evidence for why a longing for God appeared to occur only among the surveyed Catholics. Thus, further research is required.