INTRODUCTION
Abnormalities in emotional functioning are a core feature of the negative symptoms in schizophrenia.1 The ability to express an emotional experience is impaired in many patients with schizophrenia.2 Remarkably, if asked for self-reports on their emotions during a number of emotion-eliciting tasks, patients mostly describe having the same extent of feelings as healthy controls34 or were found to experience more intense negative feelings than controls.56 Thus, a disconnect between the subjective experience and the expressive display of emotions seems to characterize patients with schizophrenia.1 Emotional inexpressiveness might evoke negative responses from interaction partners and foster patients' social isolation.78
A good deal of research has been dedicated to the inability of patients to discriminate among different facial emotions, as well as between neutral and emotional faces.91011 The deficit seems to be particularly pronounced for the recognition of fearful faces.912 It also extends to unaffected relatives13 and to high-risk populations,14 hinting that poor affect recognition might be a vulnerability marker of schizophrenia.
With respect to the neural underpinnings of facial affect processing in patients with schizophrenia, the amygdala has come to represent a core region of interest.15 Most studies report that patients in comparison to controls show under-recruitment in areas associated with affect processing, including the amygdala, hippocampus, fusiform gyrus and anterior cingulate gyrus.16171819 Conversely, some recent work has suggested amygdala overrecruitment.20212223
Various reasons might account for these heterogeneous results. First of all, differences between the functional magnetic resonance imaging (fMRI) paradigms seem to have a large impact on the outcome. Amygdala hyperactivation in patients is mainly found in studies using paradigms with minimal cognitive loads23 and depends on the baseline condition used.1523 Another cause may reside in within-group differences for samples of patients with schizophrenia. Specifically, the proportion of patients with flat affect might play an important role. Within-group analyses of patients have consistently found a correlation between amygdala activation and negative symptoms, particularly flat affect.2425 That is, patients whose emotional expressivity is impaired show higher amygdala activation than patients with adequate expressivity. The authors suggest that a reduced display of emotions might serve as a protective mechanism from emotional overstimulation. Thus, samples encompassing a large proportion of patients with affective negative symptoms would be more likely to reveal hyperactivation of the amygdala and other limbic regions.
Whereas most studies have focused on the controlled processing of facial affect, a strand of research has turned towards automatic affect processing in schizophrenia.262728 These studies measured perceptual sensitivity to emotional information without conscious evaluation. They applied priming paradigms where affective face stimuli were masked by neutral stimuli. As demonstrated in a seminal study by Murphy and Zajonc,29 affective primes bias the evaluation of subsequent mask stimuli. Höschel and Irle26 have shown that patients with schizophrenia are more susceptible to affective priming than healthy controls. Suslow and colleagues27 found that this heightened sensitivity to affective priming is especially prominent for patients with affective flattening.
As for the neural basis of patients' heightened sensitivity to affective priming, again the amygdala seems to play a crucial role. Rauch and colleagues28 have found that patients exhibit an increased amygdala response to sad and happy primes. Furthermore, the amygdala responses to the affective primes correlated positively with affective flattening.
The aim of the present study was to examine amygdala responsivity to fearful expressions at an automatic and a controlled processing level in patients with schizophrenia compared to healthy subjects. The perception of fearful expressions in schizophrenia is particularly intriguing, as patients report heightened experiences of fear in everyday life30 and seem to have a specific deficit in recognizing fear in others.9 The stimuli presented were pictures of facial expressions of basic emotions (fear, disgust, happy, and neutral). For the purpose of the present study, the paradigm was selectively analyzed, as we focused on fearful face stimuli. In order to test whether the effects generalize to other negative emotions, we performed the same analyses using disgustful face stimuli as a control condition.
In cognitive psychology, a distinction is made between mental processes that are controlled and those that are automatic.31 Controlled processes are voluntary, slow, effortful, and controllable and require attentional resources. Automaticity of processing can be assumed when processing occurs unintentionally, fast, efficient, uncontrollable, and with no or minimal attention.32 Automaticity is not a unitary construct but it can be diagnosed by considering the presence of single features or processing characteristics.3233 Thus, not all of these conditions have to be fulfilled to assume automaticity of processing. In our experiment, processing of masked facial emotions should have been automatic in the sense of fast and unintentional. The processes elicited by the emotional faces were fast because prime stimuli were presented only for a thirtieth of a second immediately followed by masking facial stimuli. It appears unlikely that subjects had conscious intent to process prime faces since they were not informed about the presence of prime stimuli but they were instructed to attentively watch and memorize the mask faces. Against this background it can be assumed that processing of the masked prime faces should have occurred, in general, under conditions of inattention or distraction in our study. However, since we did not administer an objective measure of prime awareness we cannot claim that presentation of our prime stimuli was subliminal, i.e. below the threshold of conscious perception.
Three research questions were addressed in the present study. Firstly, we investigated if patients exhibit abnormalities in amygdala activation during automatic and controlled processing of fearful expressions. Secondly, we clarified the impact of affective flattening on amygdala activation during automatic and controlled fear processing. Thirdly, we explored the interrelation between automatic and controlled affect processing, examining if the amygdala activation in response to masked fearful expressions was predictive of amygdala response to unmasked fearful expressions.
We hypothesized that patients with schizophrenia manifest heightened amygdala activation during the processing of masked and unmasked fearful expressions. Secondly, we hypothesized that patients with symptoms of affective flattening would show heightened amygdala activation in comparison to both controls and patients without these symptoms. Thirdly, we assumed that affective flattening would be positively correlated to amygdala activation during automatic and controlled processing of fearful faces and that this effect would not be confounded by other variables related to amygdala activation. As for the interrelation between automatic and controlled fear processing, we had no specific hypothesis. As a control condition, we used disgustful facial expressions and tested whether the group differences and correlations in the amygdala would also emerge for this negative emotion. To our knowledge, this is the first study to examine the relationship between automatic and controlled processing of fearful facial affect in schizophrenia.
METHODS
Subjects
The original sample encompassed 36 patients with schizophrenia and 42 healthy controls aged between 18 and 55 years. For all participants, exclusion criteria were a history of neurological disease, severe head trauma causing a loss of consciousness, substance abuse during the last six months and the usual magnetic resonance imaging contraindications. All subjects had normal or corrected-to-normal vision. Control subjects were thoroughly investigated by trained psychologists and were free of any lifetime history of psychiatric disorders, as diagnosed by the Structured Clinical Interview for DSM-IV, Axis I disorders (patient version).34 Patients' diagnoses were established by senior psychiatrists and confirmed by trained interviewers with the SCID interview. During the patient interview, special attention was given to affective disorders to exclude a current depressive episode in study patients.
In addition, all patients were administered a structured protocol of the Scale for the Assessment of Negative Symptoms (SANS)2 and the Scale for the Assessment of Positive Symptoms (SAPS).35 For all participants, depressivity was measured with the Beck Depression Inventory (BDI),36 and trait anxiety was measured with the State-Trait-Anxiety-Inventory (STAI, trait version).37 Verbal intelligence was estimated by the Mehrfachwahl-Wortschatz-Intelligenztest (Multiple-Choice-Vocabulary-Intelligence-Test, MWT-B).38
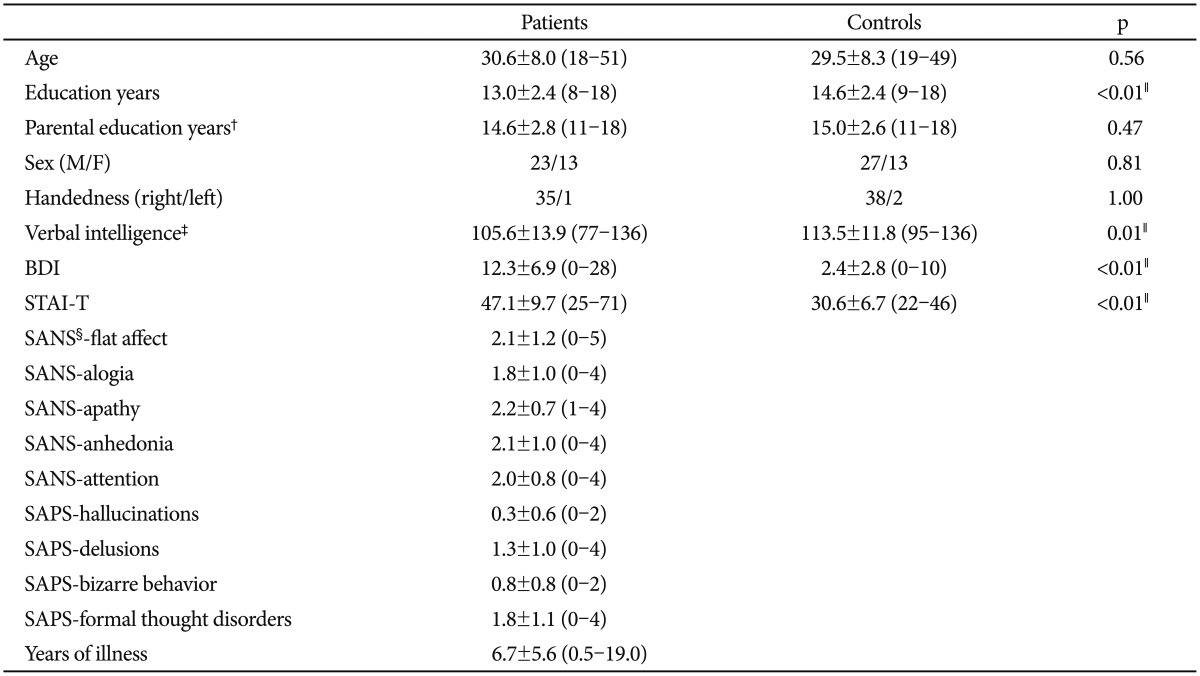
Table 1 lists the sociodemographic and questionnaire data of all participants and the clinical data of patients. Of the 36 patients, all received second-generation antipsychotics, and three received additional typical antipsychotics. Fourteen patients were taking concomitant antidepressant medication; three were taking anticonvulsants; and one was taking lithium.
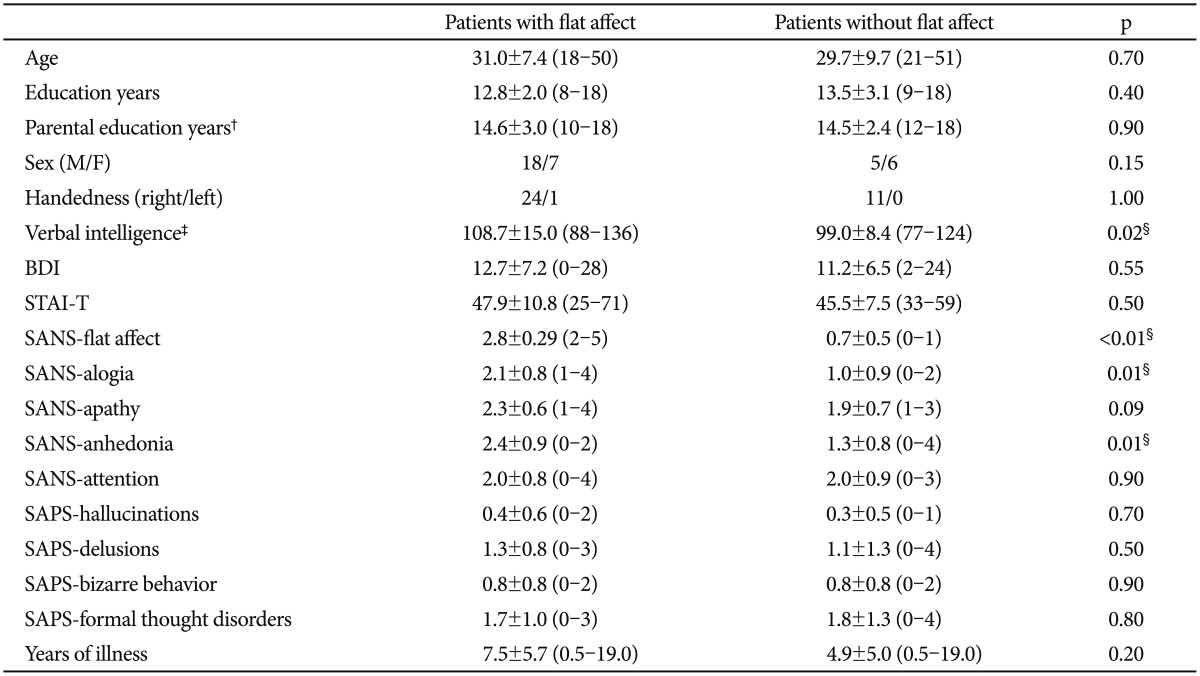
The patient sample was further divided into two subgroups of patients with and without affective flattening. The assignment was based on the SANS global rating of flat affect. Patients with a global flat affect score of at least 2 (mild symptoms of flat affect) were assigned to the flat affect subgroup. Table 2 compares the sociodemographic and clinical data of the two patient groups.
The study was conducted in accordance with the Declaration of Helsinki as revised in 1989 and was approved by the Ethics Committee of the University of Münster. After a complete description of the study, written informed consent was obtained. Patients received a financial compensation of 50 € and controls received 40 €.
Paradigm
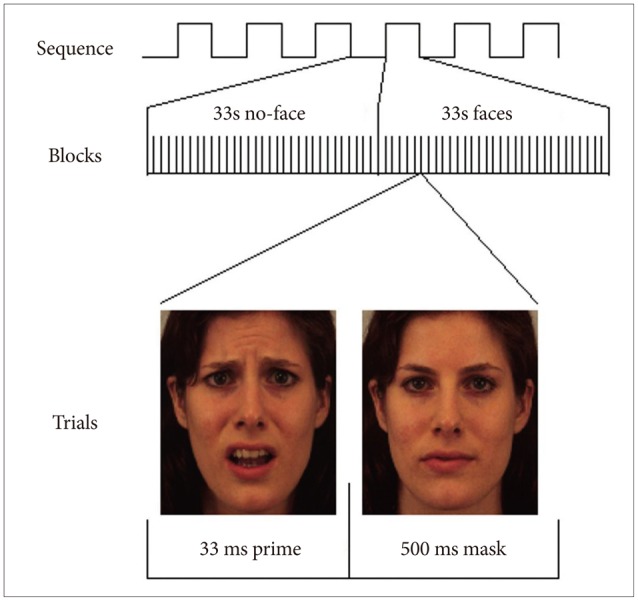
The viewing paradigm consisted of two sequences in which a sequence with masked emotional facial expressions was followed by a sequence with unmasked expressions. For the paradigm as a whole, the facial expressions displayed were fear, disgust, happiness and neutral. Facial stimuli consisted of images selected from the Karolinska Directed Emotional Faces (KDEF) catalogue.39 Stimuli represented the faces of male and female actors, and different actors were chosen for the two sequences (10 male and 10 female actors for each sequence).
In both sequences, subjects were instructed to attentively watch and memorize the facial stimuli. Subjects were presented with 33 s blocks of a facial expression category or a no-face stimulus (skin-colored semi-oval). In the first sequence (masked expressions), facial prime stimuli were presented for 33 ms and followed by a 500 ms mask depicting a neutral face of the same actor (Figure 1). In the second sequence (unmasked expressions), subjects viewed faces for 533 ms. Each emotion block was followed by a no-face block and presented twice, resulting in a presentation time of 8 min 48 sec per sequence (total time of 17 min 36 sec). The order of the blocks was counterbalanced across subjects according to a Latin square design.
fMRI methods
Images were projected to the rear end of the scanner [SharpXG-PC10XE with additional RF shielding (Covilex); Magdeburg, Germany]. T2* functional data were acquired with a 3-Tesla scanner (Gyroscan Intera 3.0T, Philips Medical Systems, Best, the Netherlands) using a single-shot echoplanar sequence with parameters selected to minimize distortion in the regions of central interest while retaining adequate S/N and T2* sensitivity. Volumes consisting of 36 axial slices were acquired (matrix 64×63, resolution 3.6×3.6×3.5 mm; repetition time=2.5 s, echo time=35 ms, flip angle=90°) 212 times in a block design.
Functional imaging data were motion-corrected, using a set of six rigid body transformations determined for each image, spatially normalized to a standard MNI space (Montreal Neurological Institute) with a voxel size of 2 mm edge length, and smoothed (Gaussian kernel, 8 mm FWHM) using Statistical Parametric Mapping (SPM5, Wellcome Department of Cognitive Neurology, London, UK). Statistical analysis was performed by modeling the different conditions (fear, happy, disgust, neutral) as variables within the context of the general linear model convolved with a standard hemodynamic response function. Fixed-effect analyses were performed at the individual level to generate individual contrast maps, and random effect analyses were performed at the group-level. On a single subject level, contrast images were calculated comparing each emotion's face block (fear, happy and disgust) with the neutral face baseline.
Due to excess motion, four subjects (2 patients, 2 controls) had to be excluded from the unmasked sequence, and two subjects (the same 2 controls) had to be excluded from the masked sequence. The final sample encompassed 40 healthy controls for both sequences as well as 36 patients for the masked sequence (patients with flat affect: n=25; patients without flat affect: n=11) and 34 patients for the unmasked sequence (patients with flat affect: n=24; patients without flat affect: n=10).
Second-level fMRI analysis
In the scope of the present paper, we focus on the fear versus neutral contrasts. The disgust versus neutral contrasts were used as a control condition for the between-group and correlational analyses. The two sequences (masked and unmasked) were analyzed separately. Standard univariate group-level statistics were calculated using SPM5. For all analyses, the amygdala was chosen as the a priori region of interest (ROI). The amygdala was defined according to Tzourio-Mazoyer et al.,40 and the amygdala mask was created by means of the WFU PickAtlas.41 To control for multiple statistical testing, we maintained a cluster-level false-positive detection rate at p<0.05 using an uncorrected voxel threshold of p<0.05 with a cluster extent (k Voxels) empirically determined by Monte Carlo Simulations (n=1000 iterations) for the bilateral amygdala. This was performed by means of the AlphaSim procedure, which accounts for spatial correlations between BOLD signal changes in neighboring voxels implemented in the REST toolbox (http://restfmri.net/forum/index.php), yielding an empirically determined cluster threshold of k=37 voxels. In addition to the ROI analyses, exploratory whole-brain analyses were performed at p<0.001 and a contiguity threshold of 15 voxels.
Between-group analyses encompassed the following: 1) comparisons between patients and controls, 2) comparisons between each of the two patient subgroups and the control group, and 3) comparisons between the two patient groups. Therefore, the contrast images were entered into separate two-sample t-tests, resulting in four between-group comparisons for each of the two sequences.
As the two patient groups differed (albeit not significantly) with respect to the duration of illness, we repeated all between-group analyses using duration of illness as a covariate. As between-group effects were not smaller using the covariates, we report only the results of the original analyses.
In the next step, the relationships between amygdala response to the masked and the unmasked fearful expressions and the patients' affective negative symptoms were investigated. We computed simple regression models as implemented in SPM5, using the SANS global score of affective flattening as regressor to the fearful versus neutral expression contrast images. Subsequently, the mean contrast values of significant clusters within the amygdala were extracted for each participant and further analyzed with SPSS 20 (IBM, Armonk, NY, USA). We constructed a multiple regression model predicting amygdala responsiveness by the SANS global score of flat affect, controlling for age, gender, verbal intelligence, duration of illness, trait anxiety and depression level. To explore which symptoms of flat affect would best predict amygdala responsivity, we correlated each of the six single items of affective flattening with amygdala responsiveness.
Next, we investigated the relationship between the amygdala responsiveness to both masked and unmasked fearful expressions. For each participant, the mean contrast values of amygdala activation to fearful versus neutral faces were extracted. We generated regression lines for the contrast values of the unmasked fear versus neutral contrast and the contrast values of the masked fear versus neutral contrast, and we compared correlations using Fisher-Z-test.
RESULTS
Between-group comparisons
In the unmasked sequence, a comparison between patients and controls revealed greater activation in both the left and the right amygdala for patients (right peak voxel xyz: 30 -2 -28, cluster size: 105, Z-score=4.33, p=0.000007; left peak voxel xyz: -30 -2 -22, cluster size: 69, Z-score=2.65, p=0.004). Both schizophrenia groups showed greater amygdala activation than the control group, and there was no significant dif-ference between patients with and without flat affect.
In the masked expressions sequence, no significant difference between the patient group and the control group emerged. Subgroup analyses revealed that patients with affective flattening showed greater activation in the right amygdala than controls (peak voxel xyz: 26 -8 -14, cluster size: 125, Z-score=3.02, p=0.001) and greater activation in both amygdalae than patients without flat affect (right peak voxel xyz: 26 -2 -22, cluster size: 171, Z-score=3.62, p=0.0001; left peak voxel xyz: -30 -4 -16, cluster size: 71, Z-score=3.11, p=0.0009). Conversely, patients without flat affect showed less activation in the right amygdala than controls (peak voxel xyz: 26 -2 -28, cluster size: 46, Z-score=2.58, p=0.005).
The complete results of the exploratory whole-brain analyses are listed in Supplementary Table 1 and 2 (in the online-only Data Supplement). With respect to the unmasked sequence, patients showed hyperactivation versus controls in several areas associated with face and affect processing. There was no anatomical area in the brain showing hyperactivation for controls versus patients. For the masked sequence, patients exhibiting flat affect showed increased activity in brain regions associated with face and affect processing, relative to controls and to patients without affective flattening. Relative to patients exhibiting affective flattening, controls showed no increased cerebral activity in any anatomical region.
Figure 2 presents an illustration of percent signal change in amygdala activation in response to fearful faces. The figure shows percent signal change of the two patient groups and the control groups for the masked and the unmasked face sequence.
For our control condition of disgustful faces, we found a difference between patients and controls in the unmasked sequence. Patients showed greater activation in the bilateral amygdala than controls (right peak voxel xyz: 30 -2 -26, cluster size: 108, Z-score=3.33, p<0.001; left peak voxel xyz: -28 -4 -20, cluster size: 117, Z-score=3.01, p=0.001). Both schizophrenia groups showed greater amygdala activation than the control group, and there was no significant difference between patients with and without flat affect. In the masked expressions sequence, we found no differences between the two patient groups and the control group with respect to amygdala activation.
Correlational analyses
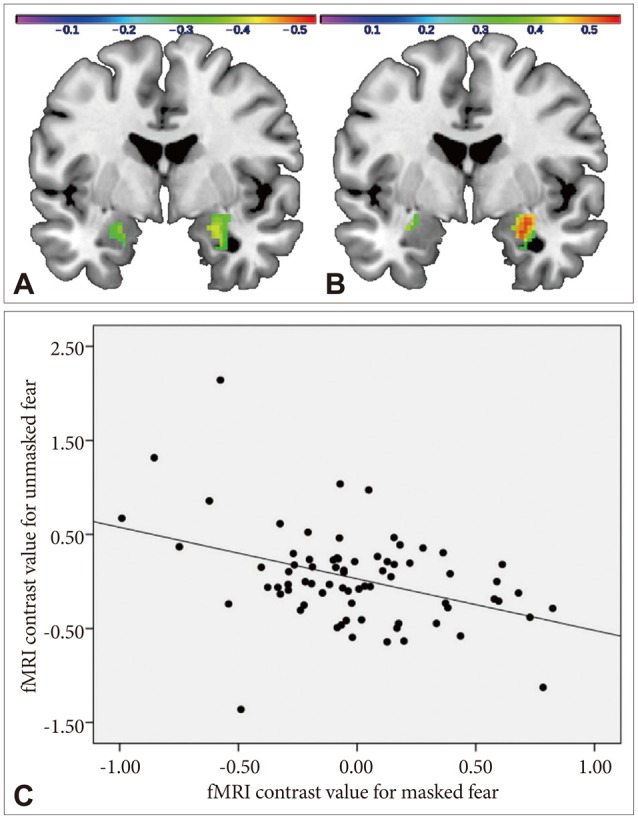
For the unmasked sequence, the regression analysis conducted with SPM5 yielded a significant negative correlation of the SANS global score of flat affect and bilateral amygdala responsiveness to fearful versus neutral faces (right peak voxel: 26 -6 -16, cluster size: 119, Z-score=3.22, p=0.0006, r=-0.40; left peak voxel: -26 2 -26, cluster size: 75, Z-score=2.57, p=0.005, r=-0.42) (Figure 3A). In the subsequent multiple regres-sion analysis predicting the mean activation of the significant clusters by the SANS global flat affect score, Beck Depression Inventory score, State-Trait-Anxiety-Inventory trait score, duration of illness, verbal intelligence, age and gender, the SANS global flat affect score was the only significant predictor (right amygdala: β=-0.48, t=-2.47, df=33, p=0.020; left amygdala: β=-0.44, t=-2.28, df=33, p=0.031). No other predictor had a significant effect on amygdala activation (all p>0.20). Thus, the negative correlation between amygdala responsiveness and affective flattening was not confounded by depressivity or anxiety symptoms, duration of illness, verbal intelligence, age or gender. From the six specific flat affect symptom items (unchanging facial expression, decreased spontaneous movements, paucity of expressive gestures, poor eye contact, affective non-responsivity, lack of vocal inflections), 'lack of vocal inflections' (r=-0.40, p=0.02) and 'unchanging facial expression' (r=-0.39, 0.02) were the only significant predictors of amygdala responsiveness.
Conversely, for the masked sequence, the regression analysis conducted with SPM5 yielded a significant positive correlation of the SANS global score of flat affect and the responsiveness of the right amygdala to fearful versus neutral faces (peak voxel: 30 0 -14, cluster size: 165, Z-score=3.52, p=0.0002, r=0.52) (Figure 3B). In the subsequent multiple regression analysis predicting the mean activation of the significant cluster by the SANS global flat affect score and the covariates described above, the SANS global flat affect score turned out to be the strongest predictor (β=0.58, t=3.26, df=34, p=0.003). Furthermore, a significant positive association between amygdala responsiveness and the duration of illness emerged (β=0.38, t=2.24, df=34, p=0.03). Other predictors had no significant effect (all p>0.20). From the six flat affect symptoms, 'unchanging facial expression' was the strongest predictor (r=0.47, p<0.01), followed by 'lack of vocal inflections' (r=0.44, p<0.01), 'poor eye contact' (r=0.42, p=0.01) and 'decreased spontaneous movements' (r=0.39, p=0.02). The predictive effects of 'affective non-responsivity' (r=0.35, p=0.038) and 'paucity of expressive gestures' (r=0.35, p=0.034) were less prominent.
The complete results of the exploratory whole-brain analyses are listed in Supplementary Table 3 and 4 (in the online-only Data Supplement). For the unmasked sequence, the SANS global score of affective flattening correlated negatively with activity in a number of areas related to face processing, and there was no anatomical region in the brain that showed a positive association with the global score of affective flattening. Conversely, in the masked sequence, affective flattening was positively correlated with activity in various face-processing areas, and no anatomical region showed a negative association with the global score of affective flattening.
For the patient group, the right amygdala response to masked fearful expressions was negatively correlated with the right amygdala response to unmasked fearful expressions (r=-0.55, p=0.001) (Figure 3C). This correlation was also close to significant for the left amygdala (r=-0.33, p=0.06). For the control group, none of the correlations reached significance (right amygdala: r=-0.30, p=0.06; left amygdala: r=-0.13, p= 0.44), but the correlation was close to significance for the right amygdala. Fisher's Z-test showed that the difference of the correlation coefficients between patients and controls was marginally significant for the right amygdala (z=-1.27, p=0.1) and not significant for the left amygdala (z=-0.87, p=0.19).
As for our control condition, the correlational analysis yielded no significant results. We found no positive or negative correlations between amygdala responsiveness to masked or unmasked disgustful versus neutral faces and patients' SANS scores.
DISCUSSION
The present study has revealed a number of interesting findings which add to our understanding of limbic functioning abnormalities in schizophrenia. First of all, as hypothesized, we found that patients show a clear hyperactivation of the amygdala relative to healthy controls during their processing of unmasked fearful faces. This result is in conflict with a number of prior studies reporting amygdala under-recruitment in patients during fear processing.174243 A reason for this might reside in the task we utilized, a viewing task requiring rather low cognitive effort. Remarkably, Holt et al.23 also reported that patients with schizophrenia exhibit heightened amygdala activation in response to fearful faces using a viewing task. In patients with schizophrenia, cognitive load might impair the controlled processing of facial affect and attenuate limbic responsivity as subjects focus on task requirements.23 Contrary to our hypothesis, patients with symptoms of affective flattening did not show increased amygdala activation relative to patients without these symptoms during the controlled processing of fearful faces. This result suggests that amygdala hyperactivation at a controlled processing level might be characteristic for patients with schizophrenia as a whole. Interestingly, patients also showed amygdala hyperactivation in response to unmasked facial expressions of disgust. This indicates that a limbic overrecruitment in patients is not specific for the viewing of fearful faces but might characterize the processing of negative emotions in general.
Our hypothesis postulating that patients show increased amygdala activation during the processing of masked fearful faces was only partially confirmed. In this case, amygdala hyperactivation was found merely for a subgroup of patients with symptoms of affective flattening. Patients exhibiting affective flattening showed increased amygdala activation during automatic fear processing in comparison to both healthy controls and patients without these symptoms. This adds further evidence to the hypothesis that affective flattening is related to specific abnormalities in automatic affect processing.27 In our control condition of masked disgust faces, we did not find amygdala activation differences between the two patient groups, indicating that this effect does not generalize to all negative emotions.
Correlational analyses revealed that the degree of affective flattening was positively correlated with amygdala response to masked fearful faces and negatively correlated with amygdala response to unmasked fearful faces. These associations were not confounded by depressivity, trait anxiety, verbal intelligence, age, gender, or duration of illness. Yet, there was also a positive association between amygdala responsiveness to masked fearful faces and the duration of illness, hinting that abnormalities in automatic affect processing might worsen in the course of the disease. Among the SANS single symptom items, 'unchanging facial expression' and 'lack of vocal inflection' were the strongest predictors of amygdala responsiveness. As we did not find correlations between SANS scores and amygdala activation in response to disgustful faces, these results do not seem to generalize to all negative emotions. Future research should clarify whether similar results patterns emerge for other negative emotions like anger or sadness which were not examined in this study.
The finding of a positive association between amygdala responsiveness to masked facial expressions and affective flattening is in line with that of a prior study.28 Two other recent studies have found a positive association in paradigms using unmasked emotional face stimuli.2425 In these studies, the positive association is generally interpreted that affective flattening might represent a type of compensatory mechanism for faulty signaling from the amygdala.24 Our finding of a negative correlation between amygdala responsiveness to unmasked fearful faces and affective flattening is in contrast with these two studies. Notably, both studies used decision tasks (gender and emotion identification) requiring active reactions from the subjects. In experimental paradigms where the sole task consists in attentively viewing emotional face stimuli, symptoms of affective flattening might be associated with attenuated amygdala responsiveness.
The most innovative result of this study may be the strong negative association between amygdala activations during automatic and controlled fear processing in patients. According to the trend line, this negative correlation was also present in healthy subjects, but it was stronger within the patient group.
Taken together, our data suggest a complex relationship between limbic responsiveness during fear processing and affective flattening. Amygdala over-recruitment during the viewing of overt fearful expressions might characterize patients with schizophrenia as a whole. On the other hand, amygdala overrecruitment in response to brief fearful expressions might be specific for patients exhibiting affective flattening. Tentatively, we assume that the flattening of expressivity might constitute a learned behavioral mechanism to attenuate limbic hyperarousal in response to threatening stimuli. Our data show that this mechanism works during the controlled processing of fearful expressions, as affective flattening is in this case negatively correlated with limbic activation. Paradoxically, affective flattening seems to have an inverse effect with respect to the processing of brief facial expressions. The avoidance of overt facial expressions might lead to a sensitization of automatic affect processing. Thus, even brief threat expressions could take on a character of alarming signals. Plausibly, this increased sensitivity might prompt a further reduction in emotional expressivity and social functioning, leading to a vicious cycle of negative symptoms in the course of the disease. Meehl4445 has coined the notion of an "aversive drift" characterizing the course of schizophrenia, as patients come to experience increasingly negative feelings in many everyday activities. We suggest that the neural basis of this aversive drift might consist in a heightened limbic sensitivity for brief threat stimuli.
Certain limitations need to be acknowledged. Firstly, our findings of a negative correlation between the amygdala responses to masked and unmasked faces as well as the findings of a differential association with affective flattening are so far singular and need to be replicated. Replication studies could also provide more evidence for another interesting finding in our study. All correlations seem to be rather lateralized to the right amygdala. This is interesting, as emotional face processing in healthy persons has been shown to be rather lateralized to the left amygdala.46 It would be thinkable that right amygdala responsiveness to emotional faces is particularly associated with pathological conditions. Nevertheless, this result should not be overrated, as lateralization findings in the amygdala in individual studies might be also influenced by fMRI artifacts.46
Secondly, only prospective studies can clarify whether affective flattening down-regulates limbic overstimulation during controlled affect processing and whether this mechanism leads in turn to a limbic sensitization during automatic affect processing. Additional studies should investigate the influence of affective expressivity on limbic responsiveness. In particular, a more general and solid operationalization of emotional expressivity would be desirable, as the SANS score of affective flattening used here is a clinical rating that only applies to patients. For example, a recent study using electromyography found that patients with schizophrenia show abnormal patterns of rapid facial mimicry.47 In the future, this method could be combined with functional imaging to investigate the relationship between emotional expressivity and neural activation in different patient groups and in healthy controls.