INTRODUCTION
The coronavirus disease-2019 (COVID-2019) pandemic has led to many changes worldwide. Following the increased number of infections and deaths, public health measures such as lockdowns, social distancing, self-quarantine, online schools, and remote work have been implemented in many countries [1]. These changes significantly affected the global economy, leading to job loss and increased economic uncertainty, which subsequently had great impacts on the mental health of the general public [2,3]. Studies have shown that the COVID-19 pandemic tended to increase depression, anxiety, stress, suicide risk, and post-traumatic stress [4], and a meta-analysis study also shows that the prevalence of depression and anxiety disorder increased by 27.6% and 25.6%, respectively during the COVID-19 pandemic [1-5].
The COVID-19 pandemic has greatly increased the unemployment rate in many countries. In South Korea, 1.1 million jobs disappeared nationwide in April 2020 because of the pandemic [6,7]. Along with the opinion that unemployment is a risk factor for poor mental health, there is also the argument that poor mental health can affect unemployment [8]. Unemployment is associated with adverse psychological and physical health outcomes, including suicide, substance abuse, psychological distress, and mortality [9]. In addition, job loss owing to COVID-19 is mostly caused by external factors rather than vulnerable factors, such as individual health problems. Therefore, job loss due to the COVID-19 pandemic may help understand the effects of employment on mental health [6-10].
The effects of COVID-19 on health may also vary depending on socioeconomic status (SES): individuals with lower resources for indicators of inequality, such as income, education, sex, and employment status, experience higher COVID-19 severity and mortality due to underlying clinical risk factors such as hypertension, diabetes, obesity, and smoking [11,12].
Conversely, social support—defined as psychological and material resources for an individual—can reduce the negative psychological effects of unfavorable events on mental health [13]. Previous studies have shown social support to regulate the relationship between risk perception of COVID-19 and mental health symptoms in the general population [14], and act as a protective factor for mental health [13-15].
In this study, we investigated the association between job loss during the COVID-19 pandemic, depressive and anxiety symptoms, and suicidal thoughts in economically active South Korean adults using a nationally representative sample. We also investigated whether SES potentially moderates the association between job loss since the pandemic outbreak and mental health status. Furthermore, we explored whether perceived social support mediated the association between job loss during the COVID-19 pandemic and mental health status.
METHODS
Study participants and the survey
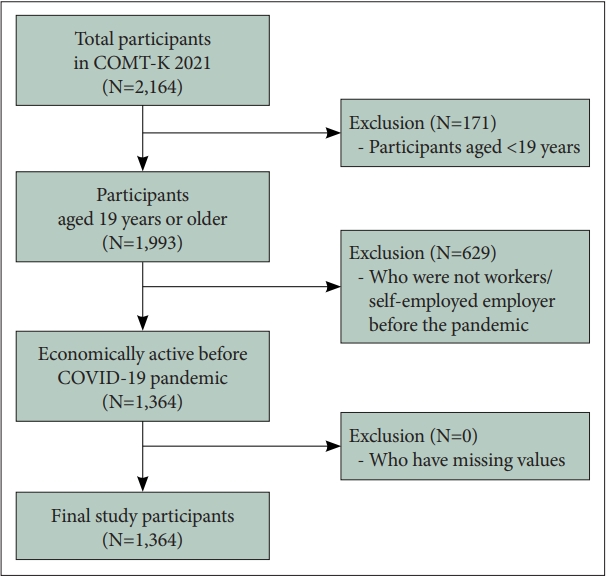
We obtained the data from a nationwide, online, cross-sectional survey called the “Coronavirus Disease National Mental Health Survey in Korea (COMT-K),” conducted in South Korea. This survey investigated the impact of the COVID-19 pandemic on the general population of South Korea regarding mental health status and psychological perspectives. The online survey was commissioned by Korea Research International and was conducted over two periods: between March and April 2021 and between June and July 2021. Participants were selected from more than 17 metropolitan cities and provinces, accounting for the proportion of the population by city and age. The survey was conducted on a website (http://covidmentalhealth.or.kr) using semi-structured self-administered questionnaires to investigate mental health, psychological status, quality of life, and socioeconomic and physical health-related determinants. A stratified multi-stage cluster sampling design was adopted to obtain a representative and systematic sample. A total of 2,164 community-dwelling people aged 14-69 years completed the first (n=1,150) and second (n=1,014) surveys (Figure 1). Among respondents aged 19 years or older (n=1,993), this study used the data of 1,364 respondents who were economically active before the COVID-19 pandemic (i.e., standard or non-standard wage workers, non-paid family workers, or self-employed/employers) and excluded the data of non-economically active respondents (n=629) before the pandemic. We confirmed that none of the participants (n=1,364) in the total sample had missing values. All respondents provided informed consent before participating in the study. The study protocol was approved by the Ethics Committee of Kangwon National University (IRB approval number: KWNUIRB-2020-03-004-001).
Assessment of job loss during the COVID-19 pandemic
Respondents’ experience of job loss due to COVID-19 pandemic was investigated using the following single-item question: “Have you ever experienced job loss since the COVID-19 Pandemic outbreak?” (response: yes or no). All the respondents in the sample answered the question, and we classified respondents who answered “yes” as those who had experienced job loss during the COVID-19 pandemic.
Psychometric measurements
In the survey, depressive symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9), which is a self-reporting scale and has been most-widely used both in primary care settings and psychiatric epidemiological studies [16]. This questionnaire evaluates depressive symptoms during the most recent 2-week period based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) for a major depressive disorder [17,18]. The PHQ-9 uses a 4-point Likert scale. It comprises nine items and measures the frequencies of depressive symptoms from 0 to 3 (0=not at all; 1=several days; 2=more than half the days; and 3=nearly every day) [17]. The Korean version of the scale was reported to have excellent internal consistency and validity [19,20]. The present study determined PHQ-9 scores of 10 or above as significant depressive symptoms according to previous psychiatric epidemiological studies on the COVID-19 pandemic [21-23]. For the prevalence of suicidal thoughts, we used the ninth item of the PHQ-9, “How often have you been bothered by thoughts that you would be better off dead or hurting yourself in some way?” and we determined a response of 1 or above as the presence of suicidal thoughts [24-26]. This assessment of suicidal ideation has been widely adopted in previous studies [27,28].
Anxiety symptoms were evaluated using the General Anxiety Disorder-7 (GAD-7), which is one of the most-widely used self-reporting scale based on the DSM-IV criteria for generalized anxiety disorder [29]. The GAD-7 comprises seven items and measures frequencies of anxiety symptoms during the most recent 2-week period using a 4-point Likert scale with responses ranging from 0 to 3 (0=not at all; 1=several days; 2=more than half the days; and 3=nearly every day) [29]. The Korean version of the GAD-7 showed excellent validity and internal consistency [30,31]. We used a cutoff score of 10 or above as a prevalence of significant anxiety symptoms based on previous epidemiological studies on the COVID-19 pandemic [21-23].
For the assessment of perceived social support level, in the survey, we adopted the Duke-UNC Functional Social Support Questionnaire (FSSQ) [32], which has been widely used in psychiatric studies [33-35]. We used an 8-item version of the FSSQ owing to its excellent validity [36]. The FSSQ uses a 5-point Likert scale with eight items that assess perceived amount and type of individual social support, with responses ranging from 1 (much less than I would like) to 5 (as much as I would like) [36,37]. The Korean version of the FSSQ was validated and showed high internal consistency [38]. The FSSQ assessed respondent’s perceived level of social support at the time of response to the survey.
In the present study, the Cronbach’s α of the PHQ-9, GAD-7, and FSSQ scores were 0.902, 0.924, and 0.928, respectively.
Covariates
We included the following sociodemographic and health-related characteristics as covariates in the analyses: age, gender, education level (middle school graduation or below, high school graduation, college degree, university degree, and graduate school or above), marital status (e.g., never married, married, widowed, divorced, and reconciliation after divorce), religion (e.g., Protestant, Roman Catholic, Buddhism, and none), monthly household income level (<1,500,000 South Korean Won [KRW]; ≥1,500,000 & <3,000,000 KRW; ≥3,000,000 & <5,000,000 KRW; ≥5,000,000 & <8,000,000 KRW; and ≥8,000,000 KRW), job status (standard wage workers, non-standard wage workers, non-paid family workers, and self-employed/employer), prevalence of any chronic diseases (yes, no), alcohol consumption (past or never; <1 drink/month; 2-4 drinks/month; 2-3 drinks/week; and 4 or more drinks/week), and cigarette smoking (never; former; and current), as shown in Table 1.
Statistical analyses
A chi-square test was used to investigate the difference of socioeconomic and health-related variables between individuals with and without experience of job loss during the COVID-19 pandemic. A logistic regression analysis was conducted including job loss during the COVID-19 pandemic as the independent variable (IV), depression, anxiety, and suicidal ideation as the dependent variables (DVs), and all socioeconomic and health-related variables as covariates (i.e., age, gender, education level, marital status, religion, monthly household income level, job status, chronic diseases, alcohol consumption, and smoking).
Then, logistic regression analyses were performed in subgroups determined by household income and education levels to explore the moderating effect of SES (i.e., income and education level). The subgroup analyses also included the aforementioned socioeconomic and health-related variables as covariates. Subgroups were determined as follows: 1) low income (<5,000,000 KRW) and high income level (≥5,000,000 KRW); 2) low education (college degree or below) and high education level (university degree or above).
We also explored the potential mediation effects of perceived social support in the association of job loss during the COVID-19 pandemic with depressive and anxiety symptoms using the mediation analysis method by Hayes and Preacher [39]. In the mediation model, job loss (yes, no) was included as IV, the PHQ-9/GAD-7 scores as DV, and the FSSQ score as a potential mediator. The aforementioned socioeconomic and health-related variables were also included as covariates. We used the PROCESS macro program (ProcessV2.16.3; http://www.processmacro.org/download.html) developed by Hayes and Preacher [39] for mediation analyses, which automatically calculates indirect effect of mediators using a nonparametric resampling bootstrapping procedure in a regression model. The mediation analyses using the non-parametric bootstrapping method with 5,000 resamples provide a 95% confidence interval (CI) of the mediation effect [39]. The mediation analyses were performed in the total study participant and subgroups determined by income and education level as indicated above. All statistical analyses in the present study were performed using IBM SPSS Statistics for Windows Version 24.0 (IBM Corp., Armonk, NY, USA), and statistical significance was considered at p<0.05.
RESULTS
Socioeconomic and health-related characteristics of the sample
Among 1,364 adults (aged ≥19 years) of the total sample, 309 (22.7%) had experienced job loss during the COVID-19 pandemic (Table 1). A significantly higher proportion experienced depression, anxiety, and suicidal thoughts during the 2 weeks prior to the assessment in the chi-squared test (all, p<0.001) (Table 1). Individuals who experienced job loss during the COVID-19 pandemic had significant differences with regard to age, gender, education level, marital status, monthly household income, job status, and perceived social support compared with those did not (all p<0.05) (Table 1).
Association between job loss due to COVID-19 pandemic and mental health status in total sample
Adults who had experienced job loss during the COVID-19 pandemic were more likely to have depressive (odds ratio [OR]=1.63, 95% CI=1.16-2.29) and anxiety symptoms (OR=1.92, 95% CI=1.28-2.88) and suicidal thoughts (OR=1.86, 95% CI=1.31-2.66) than those who did not (Table 2), (Supplementary Table 1 in the online-only Data Supplement). We performed the Hosmer-Lemeshow test to evaluate the goodness-of-fit of the logistic regression model in the total sample and found that the model has a sufficient goodness-of-fit (χ2=4.384, p=0.821).
In the subgroup analysis according to household income level, job loss during the COVID-19 pandemic was associated with depressive (OR=1.75, 95% CI=1.21-2.54) and anxiety symptoms (OR=2.02, 95% CI=1.28-3.20) and suicidal thoughts (OR=1.96, 95% CI=1.33-2.89) among those with low income level, while job loss was not associated with increased odds of depressive and anxiety symptoms and suicidal thoughts among those with high income level (Table 2).
In the subgroup analysis according to education level, adults who experienced job loss during the COVID-19 pandemic were more likely to have depressive (OR=1.89, 95% CI=1.14-3.14) and anxiety symptoms (OR=3.02, 95% CI=1.61-5.64) and suicidal thoughts (OR=2.66, 95% CI=1.55-4.58) than those who did not, within the low education level group, while job loss did not significantly increase the odds of depressive and anxiety symptoms and suicidal thoughts among those in the high income level group (Table 2).
Mediation of perceived social support in the association between job loss due to COVID-19 pandemic and mental health status
In the mediation analysis, we observed significant partial mediation pathways between job loss during the COVID-19 pandemic and the PHQ-9 and GAD-7 scores through the FSSQ score in the total sample (Table 3). We confirmed the significance of the mediating effects of the FSSQ score by checking that the 95% CI of both indirect effects did not contain zero, as shown in Table 3. In the subgroup analyses by income and education levels, the FSSQ score had a significant mediation effect in the association of job loss with both the PHQ-9 and GAD-7 scores only within the low income group. no significant mediation effects were found in high income group, low education group, and high education group (Table 3). The ratio of mediation effect to total effect was higher in the low income group than that in the total sample with regard to PHQ-9 and GAD-7 scores (Table 3).
DISCUSSION
The prolonged COVID-19 pandemic has led to a global economic crisis, and the resulting job uncertainty and stress have caused various mental health problems, such as depression, anxiety, panic attacks, and post-traumatic stress disorder [40,41]. Compared with studies on the physical and psychological effects of COVID-19, a relatively small number of studies have investigated the effects of increased unemployment during the pandemic on mental health [42]. In the present study, we observed that job loss during the pandemic affected poor mental health outcomes, such as depression, anxiety, and suicidal thoughts, with significantly higher risks, especially in individuals with low income and education levels. The level of social support had significant mediating effects on the association between job loss and mental health status [40-42].
In one study conducted in the United States, mental health was assessed according to changes in employment status during the COVID-19 pandemic. Those who worked from home during the pandemic showed no changes in mental health indicators. In contrast, those who had lost their jobs showed more severe symptoms of depression, anxiety, and stress [43]. In another study in the United States, young adults who had lost or had been expected to lose their jobs because of COVID-19 were at higher risks for anxiety, worry, loss of interest, and depression [44]. In a study on the relationship between job loss and mental health during the COVID-19 lockdown period in South Africa, the depression score was significantly lower in those who had maintained their job than in those who had lost their jobs, and paid leave positively affected the mental health of adults [10]. These previous findings are in line with our results indicating that job loss was associated with negative mental health outcomes [10,43,44].
A study that investigated a representative sample of the Australian population during the early acute period of COVID-19 reported that work and social functioning impairments caused by the pandemic were associated with depression, anxiety, and decreased psychological well-being. Furthermore, financial difficulties, rather than job loss, were associated with worsening mental health [45]. Although we did not directly assess the effects of financial difficulties, another study conducted during the COVID-19 pandemic in the United States showed that both financial concerns and job loss during the COVID-19 pandemic were associated with greater anxiety symptoms [45,46].
During the COVID-19 pandemic, individuals with low SES were at high risk of losing their jobs and contracting COVID-19, which indicates that the vulnerability to mental health risks due to economic difficulties varies according to SES [47]. In studies conducted during the COVID-19 pandemic, those with low SES experienced greater COVID-19-related anxiety [48], and individuals with lower education levels experienced more depression and anxiety [49]. In addition, students with high or stable income reported less anxiety than those with low or unstable income [50,51]. A national survey of 100,000 adults in Norway reported that depressive symptoms increased in all SES strata after the onset of the COVID-19 pandemic; in particular, women with lower education levels and men with lower incomes had relatively more severe depression symptoms than those with higher education and income levels [52]. These were consistent with the findings of our study that individuals with low income and low education are more likely to have poor mental health outcomes due to job loss during the COVID-19 pandemic [47-52].
In a previous study that modeled the effects of unemployment on suicide, job loss increased the risk of suicide by 20%-30% [53], and a follow-up study based on this model showed that the global unemployment rate increased by 0.708% owing to the COVID-19 pandemic, predicting an increase by about 9,570 suicide cases [54]. South Korea has the highest suicide rate in the world, and a systematic review study identifying socioeconomic risk factors for suicide in this country reported that low income, unemployment, and financial difficulties were risk factors for suicide and were associated with low educational achievement [55]. Contrary to experts’ predictions, COVID-19 has not led to an evident increase in suicide rate [56]; however, as unemployment may be associated with increased suicides, public health sectors must prepare countermeasures [53-56].
Our findings showed that the level of social support is a mediating factor for the association between job loss due to COVID-19 and depression, anxiety, and suicidal thoughts. This is supported by the findings of previous studies, according to which social support after job loss buffers the negative effects on mental health in all age groups [57]. Additionally, in studies conducted during the COVID-19 pandemic, social support for the vulnerable groups alleviated the aggravation of mental health problems and economic concern-related anxiety [58], and increased social support during quarantine reduced the risk of depression and improved sleep quality [59]. As the effects of the COVID-19 pandemic have prolonged, increasing social support can enhance psychological resilience to stress, thereby mitigating the emotional pain caused by job loss [57-59]. Social support promotes a higher level of psychological flexibility, which indirectly reducing psychological distress. Social support and psychological flexibility can have important implications for solving the mental health problems caused by COVID-19 [60].
Several limitations must be considered in the interpretation of this study’s findings. First, we adopted a cross-sectional design and were thus unable to determine a causal relationship between job loss during the COVID-19 pandemic and depression/anxiety in South Korean adults. Future studies with a longitudinal design are required to investigate this causal relationship. Second, the survey adopted well-validated and widely used assessment tools for depressive and anxiety symptoms [16,29]; however, as these psychiatric symptoms were not confirmed by a psychiatrist, they may be affected by retrospective bias. Further studies must be conducted to evaluate the impact of economic crises (such as job loss) on the mental health of the general population during the spread of infectious diseases. Third, we did not adopt an equivalent household income as a variable regarding income level. Thus, household income level may be influenced by the household size of individual participants in the sample, possibly affecting our results. There is a possibility that this may affect our results. Lastly, for significant moderating effects of the income and education level, we cannot be free from the possibility that no association between the job loss and mental health outcomes in specific subgroups may be derived from low statistical power due to small sample in the subgroups.
The COVID-19 pandemic has led to an unprecedented increase in unemployment, significantly damaging the mental health of the general public. As job loss can affect not only the individual but also other members of the family, the effects of job loss due to COVID-19 may be greater than that suggested by the statistics. Those with low income and education levels are at high risk of negative mental health outcomes caused by job loss due to the COVID-19 pandemic. As social support is a significant mediator that can alleviate the severity of such negative outcomes, countermeasures should be prepared to provide social support to those losing jobs during the pandemic. The findings of this study are expected to be used as basic data for national health policies to prevent the worsening of mental health after job loss due to the COVID-19 pandemic.