INTRODUCTION
Self-injurious behavior, which one in six adolescents has done at least once in their lifetime, is a major social concern worldwide [1] because it substantially impacts families and communities and causes social costs [2,3].
Despite the seriousness of the impact of self-injurious behaviors, studies to elucidate the neurobiological mechanisms underlying these behaviors are sparse, especially in adolescents. Among neuroimaging studies of adolescents with self-injurious behavior (ASI), studies have reported structural alterations using the prefrontal cortex (PFC) [4,5], anterior cingulate cortex [4,6], insula [2,7], amygdala [4,5], and hippocampus [4,5] as regions of interest, and studies using functional tasks such as interpersonal self-processing [8], social reward processing (Cyberball task [9,10], card guessing task [11], monetary incentive delay task [12]), emotional processing (emotional and self-injuring images task [13], emotional face matching task [14], masked emotional face task [15]), and pain processing (electrical stimulation task [16] and cold stimulus task [17]).
Although extensive research has been conducted, there are no definite findings. These studies mainly used magnetic resonance imaging (MRI) or functional MRI (fMRI), which is highly infeasible for use in clinical practice, and there is also a limitation that the studies were mainly performed on the Western population. In Korea, studies that examine clinical characteristics and psychosocial correlates have been published sporadically, but there are no studies on the neurobiology of self-injurious behavior [18,19].
Self-injurious behavior (regardless of suicidal intent) was the focus of this study. Based on the results of recent studies, Huber et al. [20] reported that the clinical group (bipolar disorder and suicide attempters) showed reduced left orbitofrontal cortex volume and bilateral orbitofrontal cortex thickness than the healthy control group. Brunner et al. [21] reported that female adolescents with borderline personality disorder had reduced gray matter in the dorsolateral PFC bilaterally and in the left orbitofrontal cortex compared to healthy controls. Therefore, it is plausible to assume that the PFC is the recent focus of the brain region for both non-suicidal self-injury (NSSI) [4,5], suicidal thoughts and behavior [20,22], and makes a difference in this region. In studies using functional techniques, significant results have been reported in areas related to the PFC, especially in studies using emotion processing tasks [23]. Therefore, we hypothesized that the comparison of the activity and connectivity of the PFC between adolescents with and without self-injurious behaviors, especially using tasks related to emotion processing, might show the differences and add somewhat uncover the neurobiology of self-injurious behavior.
It is well known that not only biological factors, but also various environmental factors, such as child abuse and peer victimization, are involved in self-injurious behaviors [24,25]. Considering that the unique developmental period of adolescence is related to neural diathesis and stressors [26,27]. childhood adversity was included as a mediating factor in this study.
The near-infrared spectroscopy (NIRS) device applied in this study to measure the activation and connectivity of the PFC is superior in several respects compared to existing devices such as MRI, fMRI, diffusion tensor imaging, single-photon emission computerized tomography, positron emission tomography, and electroencephalogram. It is non-invasive, has a high spatial and temporal resolution, is free of radiation exposure, and can be performed in a comfortable position and in a short amount of time without a preparation process. It is one of neuroimaging modality that can measure the hemodynamic and metabolic responses associated with neuronal activity as well as measure neuronal activity directly. Once meaningful outcomes are derived through this tool, it is expected to be used practically in the clinical field because of the many advantages mentioned above.
This study aimed to investigate the difference in prefrontal activation and connectivity with a clinically feasible instrument, functional NIRS (fNIRS), during an emotion recognition task (ERT) between ASI and psychiatric controls (PC). Furthermore, we investigated the difference in activation between groups according to childhood adversity.
METHODS
Participants
Participants were recruited from the outpatient clinic of the Child and Adolescent Psychiatry Department of Myongji Hospital. The study was approved by the Ethical Committee of Myongji Hospital (no MJH. 2020-04-010-002). Written informed consent obtained from all participants and their caregivers before participating in this study. The recruitment period began in June 2020 and ended in October 2021. An experienced child and adolescent psychiatrist conducted clinical interviews and a trained assessor performed the assessments. The inclusion criteria for the clinical group were the following: 1) aged 12-19 years and 2) any self-injurious behavior (e.g., cutting, biting, burning, carving, pinching, pulling hair, severe scratching, etc.) within a month regardless of suicide intent. The exclusion criteria for the study participants were as follows: 1) any unstable comorbidities (e.g., uncontrolled diabetes), neurological (e.g., active seizures), or mental disorder (e.g., active psychosis) and 2) serious medical conditions that require continuous treatment. The psychiatric control group was defined as who had never engaged in any self-injurious behavior with aged 12-19 years. They were recruited from the same sources and from the local community through advertisements. All participants received monetary compensation of 20,000 won (approximately $15).
Psychological assessment
Adverse Childhood Experiences
Adverse Childhood Experiences (ACE) is a self-report questionnaire that asks about emotional abuse, physical abuse, sexual abuse, emotional neglect, physical neglect, separation or divorce of parents, being treated violently, substance abuse in the household, mental illness in the household, and incarcerated household members [30,31]. The score range of the 10 items was 0-10.
ERT
The ERT was adopted to measure participantsŌĆÖ sensitivity to facial expressions of emotion. In this task, participants were asked to identify the emotion category experienced by the person in the picture. Each picture with an emotion facial expression was presented on the screen one at a time and participants were given six options to choose from (ŌĆ£disgusted,ŌĆØ ŌĆ£sad,ŌĆØ ŌĆ£happy,ŌĆØ ŌĆ£angry,ŌĆØ ŌĆ£surprised,ŌĆØ and finally, ŌĆ£afraidŌĆØ). In each trial, with a mouse click, the participants chose one of the six categories of emotion that they believed best corresponded to the one that the person in the picture was experiencing. Each picture was presented for approximately 6 s, and if no response was made within the 6-s response window, it automatically proceeded to the next trial. The task consisted of a total of 48 trials, lasting approximately 6 min for each participant, including a 30-s baseline measurement period before the task. Three practice trials were conducted before the baseline measurement to familiarize the participants with the task requirements. The accuracy and reaction time for each trial were recorded.
Forty-eight images from the Korea University Facial Expression Collection (KUFEC) [32] were selected for this task. The ŌĆ£correct answerŌĆØ for the ERT was determined by the emotional expression instruction that was given to the amateur actors during the photoshoot. Eight images (four male and four female faces each) were chosen from the six emotion categories, and the order of image presentation was randomized for each participant. Stimulus presentation and response collection were conducted using an experiment program written in Python with the PsychoPy3 [33] toolbox (https://www.psychopy.org).
fNIRS measurement
We used a portable fNIRS device (NIRSIT LITE; OBELAB Inc., Seoul, Korea) to collect hemodynamic responses from the PFC of each participant during the ERT. The device is equipped with five dual-wavelength (780 and 850 nm) laser diodes and seven photodetectors comprising 15 channels, where each source and detector composing a channel are approximately 30 mm apart [34]. The sampling rate of the device is 8.138 Hz. The device collects signals mainly from the frontopolar cortex and roughly covers the adjacent prefrontal regions, including the dorsolateral and ventrolateral PFC and orbitofrontal cortex (Figure 1).
fNIRS data preprocessing and analysis
The preprocessing steps for the data collected during ERT are as follows: first, the raw signal was filtered through bandpass filters with a discrete cosine transform with a low-pass cut-off frequency of 0.1 Hz and a high-pass cut-off frequency of 0.005 Hz to filter out physiological noise and slow drift. After the signal was log-transformed to yield the delta optical density, it was converted to the HbO and HbR concentration values using the modified Beer-Lambert law [35,36]. Subsequent analyses were performed to determine the HbO concentration signal.
Hemodynamic responses during emotional recognition were captured via a general linear model using the onsets of each trial as an event-related regressor. Within the model, in addition to the task regressor, an additional regressor capturing the onset of the baseline period, temporal derivatives of each regressor, three motion regressors to account for the head movement (gyroscope and accelerometer signals converted to movement angles), and a constant regressor were included. For the contrast vector, 1 was assigned to the task regressor and 0 to every other regressor, rendering them regressors of no interest. Therefore, channels with positive beta values that differed significantly from 0 would be considered active during the task trials.
In addition to task activation, the connectivity between channels during the entire experimental duration was also calculated to capture any task-related coordination between regions. Although activation can summarize the overall level of taskrelated responses in amplitude, the correlation, which is statistically independent of the calculation of activation, is expected to indicate whether one or more regions of the PFC showed more or less active communication with other regions in the presence of the cognitive task. The correlation between the responses of a channel pair was initially calculated using the PearsonŌĆÖs correlation, and then Fisher transformation before any statistical tests.
Statistical analysis
Statistical analysis was conducted using R [37] and RStudio [38]. Statistical significance was set at p<0.05. First, inclusion criteria were primarily based on the presence of self-injurious behavior within a month, and participants in the clinical group were recruited. Participants were divided into two groups: ASI group and adolescents without any psychiatric disorder (PC group). The Žć2 test or independent t-test was performed to explore differences in demographic and psychiatric characteristics of participants.
RESULTS
Demographic and psychiatric characteristics
A total of 37 adolescents participated (PC=14, ASI=23), and the demographic characteristics of the groups and psychiatric test results are presented in Table 1 and Supplementary Figure 1 (in the online-only Data Supplement) .
PFC activation
The overall changes in oxy-Hb concentration in the PFC during the ERT in both groups are presented in Figure 2. There was no statistically significant difference between the ASI and PC groups (all n.s) before outlier removal, but after within-group outlier removal based on interquartile range, channel 6 (p=0.047) and channel 13 (p=0.02) reached significant differences, and channel 5 (p=0.089) and channel 9 (p=0.06) were marginally significant. However, none of the comparisons were found to be significant after family-wise correction. Overall, although not statistically significant, the activation patterns shown in Figure 2 suggest that the ASI group showed greater prefrontal activation than the PC group during the ERT.
fNIRS connectivity
Channel-wise connectivity analyses were performed within the PFC. In the ASI group, channel 6, located in the right dorsolateral PFC, showed significantly higher connectivity with other channels than the PC group during the ERT (Figure 3 and Supplementary Figure 2 in the online-only Data Supplement).
The greater correlations between channel 6 and every other channel in the PFC were significant only before the multiple comparison correction. However, correction performed on pairwise connectivity is rare, and the singularity of channel 6, if any, would be penalized, resulting in null results. Therefore, we report the non-corrected statistics here, which require caution when interpreting the results.
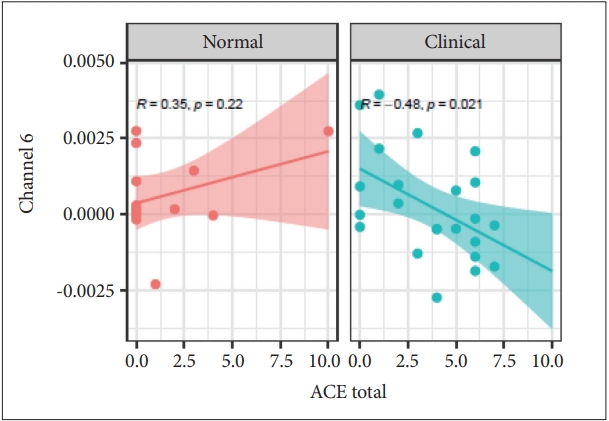
Relationship between channel 6 and ACE total score by groups
The interaction between channel 6 and the ACE total score showed statistical significance between the two groups(t[33] -2.61; p=0.014). The PC group showed no correlation with channel 6. The ASI group showed a negative correlation with activation, according to the ACE total score (PearsonŌĆÖs r=-0.48; p=0.021) (Figure 4).
DISCUSSION
This is the first study to investigate PFC connectivity, showing the extent of hemodynamic responses between channels during ERTs in ASIs. In terms of activation, showing the extent of the hemodynamic response of each channel, some channels reached statistical significance after removing outliers, but in terms of connectivity, only a single channel (channel 6) showed a greater correlation with other channels. Despite being a null finding considering multiple comparisons, it is meaningful to report it because a challenging study was conducted in ASI.
Consistently reported research results indicated that areas involved in facial expression recognition were the anterior medial PFC, posterior cingulate cortex, and adjacent temporoparietal junction [39,40]. The lateral PFC and anterior cingulate cortex are known to modulate the activity of the above-mentioned region [41]. Although the tasks used were different, a study of female adults with self-injurious behavior showed increased activity of the dorsolateral PFC [42]. Nakamura et al. [43] suggested that the right lateral PFC is involved in the processing of emotional facial expressions. Although there was a gap in the areas identified in our findings, a study showed cortical alterations in female adolescents with NSSI using emotional stimulation [13]. Due to the limitations of NIRS, it was not possible to accurately identify the interplay with the area within the deep brain but considering that it is involved in emotional processing and is the target of neuromodulation, it seems to be a plausible finding. It is believed that the interplay with deep brain structures, such as the amygdala and insula, should be seen to interpret the connectivity relationship in a more detailed manner. To explain this at a hypothetical level, it appears that the ASI group uses more brain by increasing connectivity in processing emotional recognition compared to the control group.
Interestingly, there was a significant negative correlation between ACE and channel 6 activation among the ASI group. That is, ASI showed decreased channel 6 activities as the number of ACE increased, apart from the control group. This is consistent with previous findings that have shown differential frontal brain activity in vulnerable trauma-exposed, nontrauma-exposed, and resilient trauma-exposed patients [44,45].
There are several limitations to this study. First, the sample size is small. Therefore, a larger design should be considered in future research. Second, consideration of psychiatric comorbidities and structured interviews of participants was absent. Sex discrepancy in the sample is another limiting factor of this study.
Despite these limitations, there is a clinical implication that a novel attempt to reveal neurobiological differences among ASI using fNIRS, a tool that can be practically used in the clinical field after its validity is confirmed. Regarding fNIRS, only one study has examined resting-state activation in youths with NSSI [46]. In addition, cultural differences are believed to be reduced by applying ERT developed and standardized in Korea. This study is expected to contribute to future self-injurious behavior research as the first to investigate the differences in the connectivity of the PFC in Korean adolescents.