INTRODUCTION
Acute respiratory distress syndrome (ARDS) is known as one of the most fatal and pathologic syndromes in an intensive care unit (ICU) [1]. Although the mortality rate is high among patients with ARDS from 11% to 87% [2], several patients survive ARDS. Thus, the quality of life among ARDS survivors is a crucial issue because they suffer from sequelaes of ARDS treatment [3,4]. One of the important sequelaes of ARDS that might worsen the quality of life was psychiatric illness among ARDS survivors [5,6]. We recently reported that a lot of ARDS survivors in South Korea have been suffering from newly developed depression and insomnia disorder [7,8]. These psychiatric morbidities in ARDS survivors can lead to self-harm or suicidal tendencies, which may result in death by suicide [9].
As the 11th leading cause of death worldwide, suicide is a major public health issue [10]. Suicide is especially critical in South Korea, with a suicide rate of 24.6 per 100,000 persons in 2019— the highest among the Organisation for Economic Co-operation and Development countries [11]. In addition, suicide comprised 5.26% (84,934 deaths by suicide/1,615,288 total deaths) of total deaths in South Korea from 2011 to 2016 [12]. Fernando et al. [13] recently reported that 0.2% of ICU critical illness survivors died by suicide in the Ontario province of Canada. They also suggested that preexisting psychiatric morbidity and receipt of invasive life support were significant risk factors for suicide among ICU survivors [13]. However, studies have yet to examine the suicide rate and its associated factors in ARDS survivors.
Therefore, using a nationwide administrative data registry in South Korea, we investigated the prevalence of suicide and associated factors among ARDS survivors.
METHODS
Study design, setting, and ethical consideration
As a nationwide and population-based cohort study, this study followed the guidelines outlined by Strengthening the Reporting of Observational Studies in Epidemiology, and the protocol for the research project is conformed to the provisions of the Declaration of Helsinki. The Institutional Review Board (IRB) of Seoul National University Bundang Hospital approved the study protocol (X-2008-630-903), and National Health Insurance Service (NHIS) permitted data sharing after approval of the study protocol (NHIS-2021-1-424). The IRB waived the requirement for informed consent because we used anonymized, retrospectively extracted data for analysis.
Data source (National Health Insurance Service and statistics Korea)
We used the NHIS database, which contains all disease diagnoses and prescription information regarding drugs and/ or procedures in South Korea as the sole public health insurance system. Individuals can receive financial support from the government after registering all disease diagnoses and prescription information. The disease diagnosis was registered in the NHIS database using the 10th revision of the International Classification of Diseases (ICD-10) codes. Additionally, we used the Statistics Korea database to extract death dates and main causes of death through December 31, 2019. Physicians must register the main cause of death (primary disease) for all patients in the Statistics Korea database in South Korea.
Acute respiratory distress syndrome survivors (study population)
We initially screened all adult patients who were 18 years of age or older and admitted to the ICU between January 1, 2010 and December 31, 2019 (10 years) with a diagnosis of ARDS. The ICD-10 code J80 was used to extract ARDS data from the NHIS database. As ARDS is a clinical syndrome that occurs with other pathological conditions such as sepsis or pneumonia1, both the main and secondary diagnosis cases of ARDS were included in this study. Thus, patients with a primary diagnosis of pneumonia and a secondary diagnosis of ARDS were included in this study. The main diagnosis was determined by the NHIS, following the end of hospitalization or death, as a disease in which the patient’s demand for treatment or examination was the greatest during hospitalization. If a patient with ARDS was admitted to the ICU twice or more, only the first episode of admission was considered in this study. Among the patients with ARDS, this study defined ARDS survivors as those successfully discharged from the hospital.
Study endpoint
The primary endpoint in this study was suicide within 1 year of receiving an ARDS diagnosis. Suicide was determined to be death by attempted suicide or self-harm (X60-X84 and Y870), as a previous study recently reported [13]. Only patients who died by suicide were considered to be the suicide group in this study.
Covariates
Physical information collected included age and sex. To reflect the socioeconomic status of ARDS survivors, the household income level served as a covariate, and the patients were divided into four groups using a quartile ratio of household income level. The results of hospital admission for ARDS treatment were collected and classified into three groups: discharge and follow-up in the same hospital, transfer to another long-term facility center, and discharge with outpatient clinic follow-up. The admission department of ARDS survivors was classified into two groups, internal medicine (IM) and non-IM. The length of hospital stay (days) and total cost of hospitalization (United States Dollar [USD]) were collected as covariates. Since hospitals with higher case volumes were associated with decreased mortality in patients with ARDS [14], we calculated the annual case volume of ARDS treatment in each hospital. All ARDS survivors were assigned into four groups using a quartile ratio, based on the hospital to which patients with ARDS were admitted, such as Q1 ≤4, Q2: 5-14, Q3: 15-28, and Q4 ≥29. The diagnoses of shock (R57), sepsis (A40, A41, and R65.2), and cases of the main diagnosis of ARDS were covariates. If a patient with ARDS received a main diagnosis of sepsis, it was classified as “sepsis-associated ARDS.” Related factors categorized as covariates included extracorporeal membrane oxygenation, neuromuscular blockade use, continuous renal replacement therapy (CRRT), and cardiopulmonary resuscitation (CPR). To reflect comorbid status, we calculated the Charlson comorbidity index (CCI) using ICD-10 codes of individual underlying diseases registered within 1 year of admission for ARDS, as shown in Supplementary Table 1 (in the online-only Data Supplement). As mental illness is a known risk factor for suicide [15], concurrent mental disorders such as depression (F32, F33, F34.1), anxiety disorder (F40, F41), substance abuse (F10-19), insomnia disorder (G47.0, F51.0), post-traumatic stress disorder (PTSD) (F43.1), and history of attempted suicide or self-harm (X60-X84, and Y870) among ARDS survivors were collected as covariates. We once more used ICD-10 codes registered within 1 year of the diagnosis of ARDS to extract these mental disorders.
Statistical analysis
The clinicopathological characteristics of total ARDS survivors are presented as mean values with standard deviations (SDs) for continuous variables, and numbers with percentages for categorical variables. To compare the clinicopathological characteristics between the suicide group and other ARDSsurviving patients, a t-test and chi-square test were used for continuous variables and categorical variables, respectively. Next, we fitted a multivariable Cox regression model for death by suicide within 1 year following the diagnosis of ARDS. The multivariate adjustment model included all covariates. In this time-to-event analysis, the duration from the date of ARDS diagnosis to death by suicide was set as time, and suicide was determined as an event. There was no multicollinearity between variables in the multivariable model with a variance inflation factor less than 2.0. A log-log plot confirmed that the central assumption of the Cox proportional model was satisfied. The results of the Cox regression analysis are presented as hazard ratios (HRs) with 95% confidence intervals (CIs). All statistical analyses were performed using R software (version 4.0.3, R packages, R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p<0.05.
RESULTS
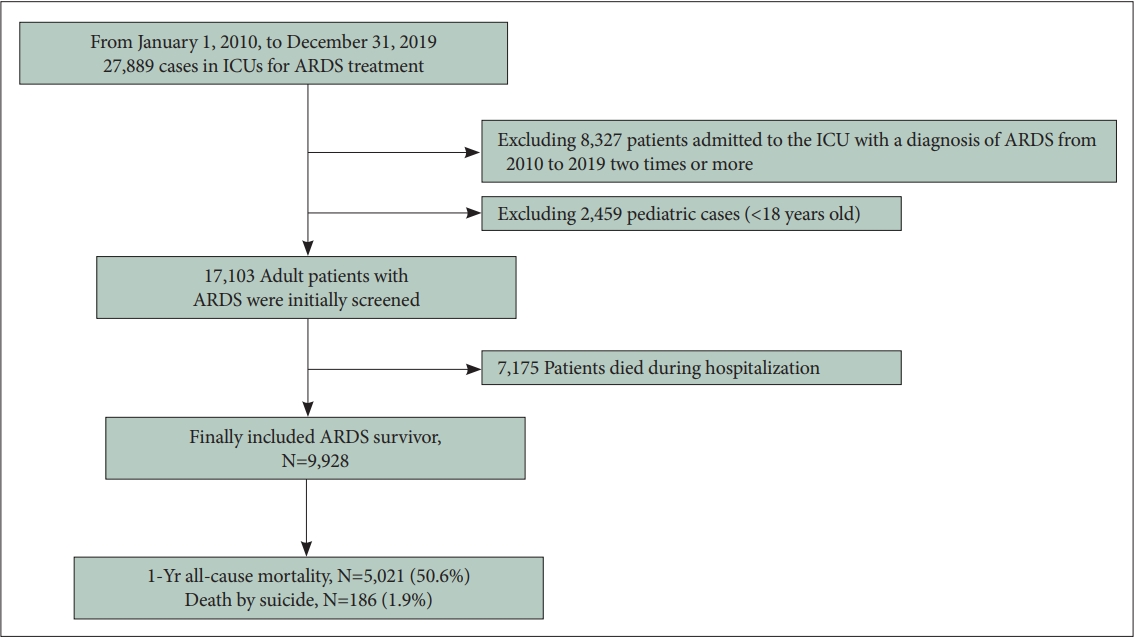
From January 1, 2010 to December 31, 2019, 27,889 cases admitted to ICUs received an ARDS diagnosis in South Korea. After excluding 8,327 cases of patients with ARDS admitted to the ICU for the second time or more during the study period (2010-2019, 10 years), only first episodes of ICU admission and 2,459 pediatric cases (aged <18 years old), 17,103 adult patients with ARDS were initially screened. Of those, 7,175 patients died during hospitalization, and 9,928 patients were included in the analysis as ARDS survivors. 1-year allcause mortality occurred in 5,021 ARDS survivors, and 186 (1.9%) died by suicide within 1 year following an ARDS diagnosis (Figure 1). Table 1 shows the clinicopathological characteristics of the ARDS survivors. The mean age was 68.7 years old (SD: 16.5 years), and 61.3% (6,089/9,928) of the studied population were male. The mean duration of hospitalization was 17.9 days (SD: 15.0 days) and the total cost was 9,735.5 USD (SD: 12,380.8 USD). Of the ARDS survivors, 7 (0.1%), 448 (4.5%), 3,278 (33.0%), 2,618 (26.4%), 2,530 (25.5%), and 12 (0.1%) had a history of self-harm or suicidal attempt, underlying substance abuse, underlying anxiety disorder, underlying depression, underlying insomnia disorder, and underlying PTSD. The 448 survivors with substance abuse comprised 410 (F10: alcohol-related disorders), 1 (F11: opioid-related disorders), 16 (F13: sedative, hypnotic, or anxiolytic-related disorders), 1 (F15: other stimulant-related disorders), 1 (F16: hallucinogen-related disorders), 6 (F17: nicotine dependence), and 13 (F19: other psychoactive substance-related disorders), respectively.
Table 2 shows the results of the comparison between the suicide group and other patients among ARDS survivors. The proportion of patients with a history of self-harm in the suicide group (3/186; 1.6%) was higher than that in the other patients (0/9,742; 0%) (p<0.001). Furthermore, the proportion of concurrent substance abuse in the suicide group (18/742; 9.7%) was higher than that in the other patients (430/9,742; 4.4%) (p=0.001).
Table 3 shows the results of the multivariable Cox regression model for death by suicide within 1 year among ARDS survivors. Older age (HR, 1.01; 95% CI, 1.01-1.03; p<0.001), CRRT use (HR, 2.00; 95% CI, 1.05-3.82; p=0.035), CPR incidence during hospitalization (HR, 2.58; 95% CI, 1.45-4.58; p= 0.001), history of self-harm or attempted suicide (HR, 41.03; 95% CI, 11.82-142.48; p<0.001), concurrent substance abuse (HR, 2.46; 95% CI, 1.47-4.10; p=0.001), and depression (HR, 1.42; 95% CI, 1.02-1.96; p=0.037) were associated with a higher risk of death by suicide in patients diagnosed with ARDS. The survival plots derived from the multivariable Cox regression model for death by suicide within 1 year among ARDS survivors according to household income level at ARDS treatment and annual case volume of hospital admission for ARDS treatment are presented in Supplementary Figures 1 and 2 (in the online-only Data Supplement), respectively.
DISCUSSION
This study showed that 1.9% of ARDS survivors died by suicide within 1 year following a diagnosis of ARDS in South Korea. History of self-harm or attempted suicide, concurrent psychiatric illness (substance abuse and depression), CPR incidence, and CRRT use were associated with a higher risk of death by suicide. Our results suggest that ARDS survivors are at a higher risk of death by suicide than other survivors of critical illness.
The prevalence of suicide (1.9%) from 2010 to 2019 among ARDS survivors in this study was much higher than that in the general population of South Korea in 2015 at 26.5 per 100,000 [16]. The old age and physical, social, and psychological burden of ARDS might affect the differences between the prevalence of suicide in ARDS survivors and the general South Korean population. Moreover, the prevalence of suicide (1.9%) among ARDS survivors in this study was approximately ten times higher (0.2%) than the suicide rate among total ICU survivors in the Canadian province of Ontario [13]. Meanwhile, patients with ARDS were known to have a higher mortality rate of 40% in a previous study [17], suggesting that our cohort (ARDS survivors) comprised more severe cases than general ICU survivors. Therefore, the sequelae or complications after hospital discharge might be more significant in ARDS survivors than in other ICU survivors, resulting in a higher risk of suicide.
In this study, older age was associated with a higher risk of suicide among ARDS survivors. A recent study reported that old age was a risk factor for suicide among Chinese adults [18], and suicide in elderly people is an important public health issue in many countries [19]. The mean age in our study population was 68.7 years (SD: 16.5 year), suggesting that most ARDS survivors were older, whose risk of suicide was higher than that of younger people. As both physical illness and the high overall burden of illness were strong risk factors for suicide among elderly people [20], we showed that ARDS can be a significant antecedent to suicide among survivors [21]. However, we also showed that CCI at hospital admission for ARDS was not associated with the prevalence of death by suicide among ARDS survivors. A previous study reported that although both physical and psychiatric comorbidities constituted risk factors for suicide, their relative timing of onset in individuals with comorbidity significantly differentiated the associated risk of suicide [22]. As we focused on ARDS survivors, psychiatric morbidities and disease severity of ARDS in addition to sequelae of treatment for ARDS might affect the risk of suicide instead of underlying physical comorbidities of ARDS survivors.
The HR of history of self-harm or attempted suicide for suicide risk was the highest (41.03) among ARDS survivors. Previous studies reported that a prior history of self-harm or attempted suicide was an important factor associated with both re-attempted suicide and death by suicide [23,24]. According to our study, ARDS survivors who experienced self-harm or suicidal tendencies before ICU admission might be at higher risk of re-attempt and death by suicide. Concurrent psychiatric illness (substance abuse and depression) was also an associated risk factor for suicide among ARDS survivors. Depression is strongly related to lifetime suicidal ideation and attempted suicide [25], and the treatment of depression has been emphasized for the prevention of suicide among elderly populations [19]. Moreover, substance use disorder is known to increase the risk of suicide [26], and prevention strategies for reducing suicide among substance users need to be prioritized at the individual level [27]. Our results suggest that ARDS survivors with concurrent psychiatric illnesses (such as substance abuse and depression) are a high-risk population for death by suicide and must be closely observed after hospital discharge.
Fernando et al. [13] reported that ICU survivors who received invasive treatment during ICU stays, such as mechanical ventilation or CRRT, were at a higher risk of death by suicide. In this study, we likewise reported that invasive treatments such as CRRT use and CPR during hospitalization were risk factors for death by suicide among ARDS survivors. The experience of invasive treatments such as CRRT and CPR during hospitalization suggests that ARDS survivors might suffer from major and severe organ failure due to ARDS [28]. A previous study reported that ARDS survivors had persistent functional disability one year after ICU discharge, and illness acquired during ICU stay and occurrence of organ failure were associated with the development of persistent functional disability [29]. Functional disability in addition to physical illness has been associated with a higher risk of suicide among older adults [30].
This study has some limitations. First, we did not consider the severity of ARDS using objective tools such as the Acute Physiology and Chronic Health Evaluation or PaO2/FiO2 ratio. As the severity of ARDS affects the risk of suicide in ARDS survivors, this might have affected the results of the study. Second, factors such as body mass index, marital status, history of smoking, and typical alcohol consumption were not included in this study because the NHIS database did not contain that information. Lastly, we used the ICD-10 codes for calculating the CCI; however, the actual underlying diseases of ARDS survivors might differ. For example, some patients went undiagnosed in the NHIS database because of mild symptoms or poor access to healthcare resources.
In conclusion, at the 1-year follow-up period, 1.9% of ARDS survivors died by suicide in South Korea. Factors such as a history of self-harm or suicide attempt, concurrent psychiatric illness (substance abuse and depression), CPR incidence, and CRRT use were associated with a higher risk of death by suicide. Our results indicate that suicide prevention and supportive care among ARDS survivors is a clinically important issue, and the knowledge of the factors associated with suicide might allow for earlier intervention to potentially reduce the death by suicide among ARDS survivors.