INTRODUCTION
The Seoul Mental Health Welfare Center (SMHWC) was established in 2005 as the first wide area facility in South Korea to protect the community of the people with mental illness. In order to improve the life quality of the people with a mental illness in the community, many projects have been carried out in a wide range of fields from mental health promotion to the management of serious mental illnesses. Recently, as the housing service adapted to the needs of the people with mental illness has become the biggest topic, the SMHWC is operating the self-reliant support housing service. Unlike existing housing facilities, the subjects are guaranteed to have independent living, and two people share the house, in which each subject has his or her own room. The case managers and self-reliant supporters provide intensive case management services.
In the past, facilities, such as hospitals and family members were mainly responsible for protecting the people with mental illness. This tendency has turned into de-institutionalization all around the world. The need for community care for the people with mental illness has risen in South Korea since the 1990s, and housing service facilities in communities have begun to settle along with the enactment of the law on community protection. Nevertheless, the number of facilities that provide housing services in the community is still limited. The way that those facilities have exclusively focused on quantitative growth appears to be facing some challenges.
Therefore, the problem of long-term admission to a hospital continues despite the fact that the services have been provided in their community [1-3]. In addition, although there are various types of facilities that provide housing services, it has been pointed out that it is provider-oriented [4-6]. In this regard, without an integrated system, the people with a mental illness is often neglected when it comes to choosing a housing service [7-9].
On the other hand, in some other countries, the housing services differ from the fragmented ones in South Korea in that it provides integrated services through a unified channel. And there is a type of housing service called ‘Supported Housing,’ which allows the community to live independently in a desired location and receive necessary services. Such a service has been provided through an integrated management centering on the request of the parties. Along the same line, there has been a tendency to reflect on the needs of people with a mental illness in South Korea [9-12]. Various types of housing services, such as community conversion facilities, cohabitation, cohabitation families, hospitals and psychiatric nursing homes, began to be provided, and related studies began to be conducted.
Thus, in this study, the SMHWC investigated the needs of the people with a mental illness and conducted the focus group interview (FGI) on the mental health professions, and based on the results of the study, it is intended to improve the qualitative aspect of the housing services by proposing the Seoul-type housing service model for the people with a mental illness. This will ultimately allow the housing services to function efficiently in helping the parties to live a healthy life with stable housing in their community.
METHODS
The study was designed by the SMHWC to identify the current status and the future direction of the housing services by examining the needs of people with mental illness for the housing services and by conducting the FGI on a group of academics and field experts related to mental health.
The questionnaire on the needs of the people with a mental illness for the housing services was filled by those who were directly involved. The subjects were those who are currently treated at mental health facilities in Seoul. Table 1 shows the type of facilities that provide housing services. The questionnaire was collected from 63 places. There were 365 subjects in total, 50 from community conversion facilities, 195 from cohabitations, 36 from cohabitations for addicts, 55 from hospitals, and 29 from psychiatric nursing homes. The questionnaire consisted of four main areas: personal information, daily living, housing services, and self-reliant living support services.
The questionnaires from ‘A Survey on the Status of Independent Living in Persons with Severe Disabilities in Seoul in 2017’ [13], ‘A Survey on the Needs of People with Mental Illness Using Facilities for the Disabled in Jeonju City and Investigation on De-facilitation for Supporting Independent Living’ [14], ‘Residential Service Needs and Related Factors among the Mentally Ill Clients’ [15] were revised and supplemented to use in our study. Although the term, “independent support service” was initially used at the time of designing this study, it was decided that the corresponding project run by the SMHWC uses the unified term, “self-reliant living support services,” so we replaced the term “independence” with “self-reliance.” As the name, ‘dorm-type cohabitation,’ was changed to the ‘independent living cohabitation’ by the ‘2018 Guide for Seoul Mental Health Business,’ ‘independent living cohabitation’ was used in this study.
Also, the mental health profession group for FGI was selected as shown below in Table 2, and three sessions were held in total for two hours per session. As for the FGI, subjects were given with questions such as “What is the role of the housing service?” along with a discussion on “the problems of current housing services and its future direction.” The meeting lasted approximately for two hours per session, and all were recorded and agreed in advance.
RESULTS
The results are as follows in order of the investigation on the needs of the housing services for people with a mental illness, the FGI analysis, and the plan for the housing service model for people with a mental illness.
First of all, as listed in Table 3, the male/female ratio was balanced for the personal information area. Subjects in their 40s to 50s accounted for 60%, and unmarried (70.14%) was predominately high. Also, the highest principal diagnosis was schizophrenia (63.84%) and the main guardians were mostly parents (37.26%).
In the area of daily living, it was found that the people with a plan (67.12%) after leaving their current facility was about twice that of people who do not have any plan (29.86%). The biggest reason for not having any plan for housing appeared to be due to not having any registered residence (46.79%) (Table 4).
As for the housing service area, ‘Not very well’ accounted for 53.15% and ‘Quite well’ accounted for 13.70% in comparison to ‘Roughly’ when asked about the their rate of awareness on the facilities that provide housing services.
Lastly, with regards to the area of self-reliant living support services, those who have needs for self-reliant living (75.34%) was significantly higher than those who do not (11.23%), and the biggest obstacle to planning for self-reliant living was found to be financial conditions (41.37%) (Table 5).
Then, with the outcome of the FGI, the current status and future direction of the housing services for people with a mental illness were observed. The problems with the housing services as discussed in the FGI are as follows.
“What do you think are the key roles and functions of the housing services? The housing services help people who lack the skills required for daily living alone so that they become accustomed to those skills. They begin with simple skills such as locking the gas valve, opening the door, and using public transportation. We intentionally make them do so since they don’t have those skills. Those skills must become second nature to them so that they feel at home with a similar environment as the facility. This is how people with a mental illness become self-reliant (Expert 6).”
“Housing services in South Korea do not help those with a mental illness to improve themselves to the next step. Instead of aiming at self-reliance, their goal is to make them adapt to the facility that they are currently using. So, is it really that the self-reliance of the mentally disabled people is the ultimate purpose of the housing services? (Expert 2).”
“Actually that’s the problem. We evaluate from the perspective of the supplier. We say that the subject cannot use some of the housing services because he or she does not have the basic skills that are required. But is that really a problem? If we offer a sufficient service, could there be a housing service he or she cannot use? We have to consider this too (Expert 2).”
“This has been an issue for a while. There are different types of facilities that provide housing services, but each type does not function properly. I think it is more urgent to reestablish the roles among the existing facilities than to diversify the types further (Expert 1, Expert 7).”
Thus, the provider-oriented service and service segmentation appear to be the most noticeable problems confronted by the housing services for people with a mental illness in South Korea. The segmentation of the housing services indicates that the original role of the housing services, which is to promote self-reliant living in the community by acquiring the skills to manage daily living, is not working properly due to the fact that the role of each facility is not clearly established. Therefore, there is a concern that the housing services might mean nothing more than an ‘accommodation’ to the people with a mental illness. Furthermore, the provider-oriented services only means providing services that suit the current conditions of the parties rather than services tailored to their needs.
The future direction of the housing services for people with a mental illness for such matter was discussed as follows.
“To provide housing services tailored to the needs of people with a mental illness in our country, we desperately need an option for supportive housing. The types of facilities available now have the basic form of cohabitation. But there are people who prefer a private life. We need to reflect such a desire (Expert 2).”
“Now that the housing services are working separately, having a housing support center to build the system will surly add some efficiency (Expert 1).”
“In advanced countries, the housing service center has a binary system. It works in a way that separates housing management from providing services for case management. A binary system like this can be easily found (Expert 2).”
“Then you need some serious thinking on the matter. Would this binary system for a housing support center work well in South Korea? I think it’s okay for the housing support center to function as a control tower. If the parties express their needs to the center, they can assess and evaluate those needs to help in choosing a housing service that meets the needs of the parties and maybe also provide them with services for case management (Expert 3).”
In sum, the future direction for the housing services is suggested as follows. First of all, it should be taken under consideration to add a new type of housing service, called ‘supportive housing’ to guarantee self-reliant living that meets the needs of the parties. This will provide services tailored to the needs rather than the somewhat limited housing service option to date. Moreover, a housing service system should be established to prevent the segmentation of the housing service. The housing support center (tentative name) would enable reestablishing roles and functions for each type of housing service and so help the parties to choose their desired services according to such information.
This could be a breakthrough to regulate the segmentation among services, the ambiguity of roles and functions, and the provider-oriented services. Although the specific system and details require further discussion, it is necessary to consider such aspects in terms of the efficiency for the providers and effectiveness for consumers.
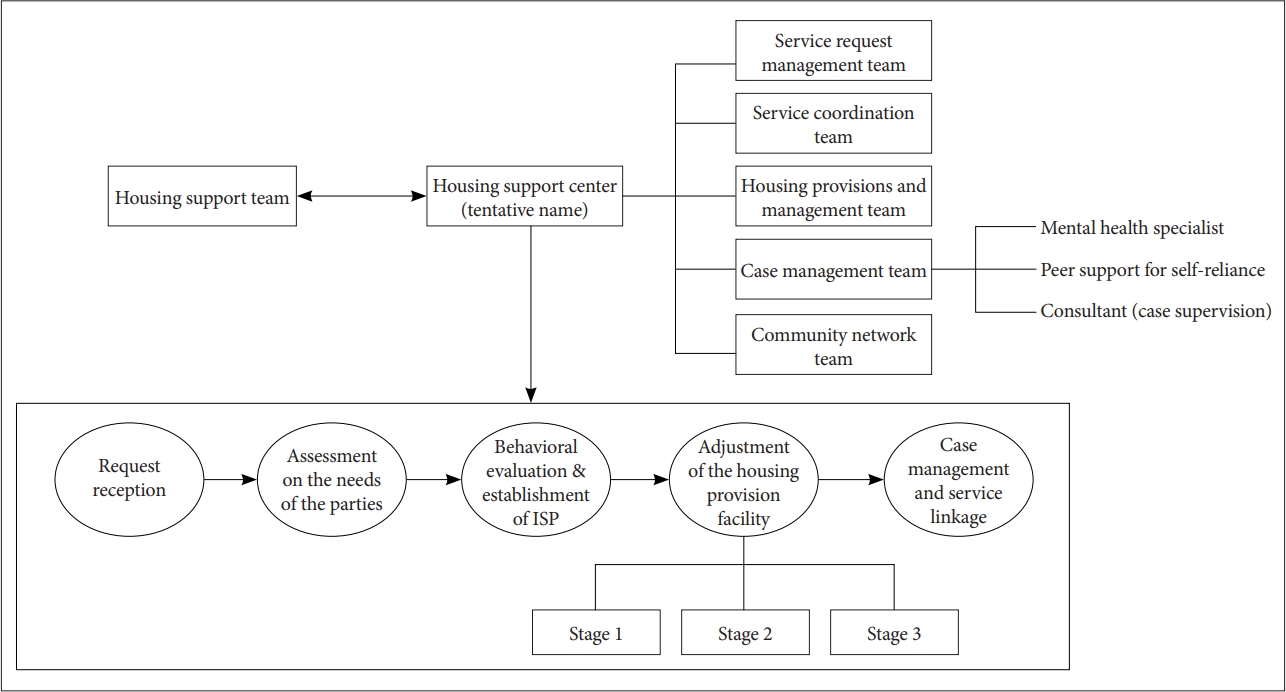
Thus, based on the results above, the SMHWC proposes the following two models for Seoul-type housing services for people with mental illness. The first model is a housing service that functions as a control tower. Model 1 is shown in Figure 1 below.
Model 1 is a control tower that establishes a housing support center, which is responsible for all housing related services such as housing provision, service provision, and case management. There, all the decision-making and promotion will be carried out together with the housing support team that is currently operated by Seoul metropolis. The housing support team is composed of Seoul metropolis, the SMHWC, and experts (field and academics) to make decisions and discussions in regards to housing services.
Thus, in the case of Model 1, all the requests and services are received and provided in a unified channel in a single institution, the housing support center. As result, all the services are managed in an integrated manner with decreased overlap and omissions. Furthermore there would be no delay in process from the beginning to the service provision. However, it might be that the system have deficit liquidity and that the independent function is weakened.
The following describes the process of the control tower in delivering housing services. When a request is made by parties or a family member, an acquaintance, or an expert, the service request management team will initially assess the parties. A multidisciplinary group of experts (physicians, mental health professions, etc.) then interviews them on their needs in housing services. One personnel from each team, as shown in the system organization chart of Figure 1, is required to participate in the interview along with the multidisciplinary group, including a physician with the parties. The behavioral evaluation should be conducted through the measures related to the housing services so that the services can be adjusted after the need assessment of the parties.
This process is regulated by the service coordination team, allowing for the establishment of an individual service plan (ISP) along with a behavioral assessment. Then, based on the needs and behaviors of the parties, a service would be recommended for them to choose. Because ISP is a structured tool which evaluates various aspects so that the mentally ill people can chose appropriate services in the community, it must be implemented before providing housing services. The facilities that provide housing services are classified into three stages as shown in Table 6. Thus, the facilities that provide housing services can be redefined with the following roles. When the stage for the service is decided, a suitable provision facility is suggested, and welfare services including case management tailored to the needs of the parties are provided.
Secondly, Model 2 is a housing service model that functions as a binary system (Figure 2). It is divided into two centers: a center that only manages housing provisions and management, and a center that provides housing support services. In this case, the decision-making of two different parties can be more independent. However, it can lower the efficiency of the service and cause a disconnection in that it is combined with not only the housing provisions but also welfare services including the case management. Comparing with Model 1, it is not easy to make an integrated decision than when making decisions and proceeding through procedures in one center.
Therefore, the housing provisions and management center should receive a request from a parties and provide information about a suitable housing facility along with all the services related to the housing provisions and management. Also, when the parties who received the service wants to be transmitted to the case management and linkage service, he or she can submit a request to the housing support center. Then, the behavioral assessment and the ISP would be confirmed in accordance with the request of the parties to provide a housing service including the case management.
Thus, for Model 2, the parties’ need for housing and services are not managed in an integrated manner but are managed by the parties’ choice to meet his or her needs.
DISCUSSION
The current study suggests that the present situation, which has biasedly resulted from the quantitative development of the housing services, has finally reached the perfect time to turn into the qualitative improvement. Therefore, the study aims to solve the problems that the housing services is currently undergoing in terms of the ambiguous roles of each housing facility, the provider-oriented service, and the limited options in choosing the type of housing service, and also to establish a housing service model that offers a living experience with a stable residence based on the needs of the people with a mental illness.
Based on the investigation on the needs of the people with mental illness and the FGI on a group of professions, the SMHWC proposes two housing service models for the Seoul-type housing services. Model 1 is a housing service that functions as a control tower. Model 2 is a housing service that functions as a binary system. What these two models ultimately seek is to reflect the needs of the parties to the housing services, to clarify the roles and functions of the housing facilities, and to expand its options for the parties to adapt to their community more easily. Therefore, both models pursue the same direction, but there is a difference in whether the directional system is unified or dualized. However, in South Korea, welfare services have been developed in a fragmented manner, and the segmentation of services has been constantly controversial. Therefore, it is necessary to apply the advantages of autonomy and liquidity so that the binary system has a unified system that functions as a control tower. Also, the content of the services and the future direction must be consistently reflected in the investigation on the needs of the parties as well as in the implication of the FGI.
On the other hand, the discussion in the current study is limited to the housing services located in the city of Seoul. The welfare services for each municipality differs from one another. Moreover, there are some limitations in that, despite the fact that many people with a mental illness residing in local communities do not use mental health related facilities, the study only included those who receive treatments from facilities. Nevertheless, this study gives significance in qualitatively providing stable living and life for the mentally disabled people based on the direct questionnaire that reflects the needs of the parties, as well as the FGI on mental health professions, which may allow such needs to be reflected in the field.