INTRODUCTION
Major depressive disorder (MDD) is a serious mental disorder, characterized by persistent low mood, lowered self-evaluation, decreased motivation, insomnia, and cognitive impairment [1,2]. At present, the general interest in MDD research focuses on the relationship between depression and cognitive deficits [3], and attentional bias is one of the core features of depression [4]. According to Beck’s cognitive model of depression, biased emotional processing of information plays a major role in the maintenance and development of depression [5]. The schemas of depressed individuals were composed of loss, separation, failure, and worthlessness. Consequently, they exhibited a systematic bias, selectively attending and processing negative stimuli in their environment [6]. It is noteworthy that recent proposals suggest that attention deployment plays a key role in mood and emotional regulation. Thus, investigations on attention-orienting biases may provide important insights into psychological vulnerability in depressive patients.
Recent studies using various tasks have shown that depression is characterized by an attentional bias towards negative information. Compared with healthy individuals, depressive patients showed a sustained attentional bias towards negative words that persisted throughout non-emotional processing trials [7]. In addition, adolescents with depression recruit visual attention regions of threat-related stimuli to a greater extent than control adolescents [8]. However, some experimental results are inconsistent. A meta-analysis of the emotional Stroop task in depression did not indicate a strong emotion-congruent bias, although emotional Stroop task has been widely used in depression research [9]. Studies using the dot-probe task have found attentional biases in depression, though only under conditions of long stimuli exposures, and not under conditions involving brief durations [10]. While behavioral tasks offer useful information regarding underlying attentional biases in depression, these tasks do not facilitate a thorough examination of this form of attentional processing. In each trial, response times provide one data time at the end of processing, but do not inform us about the time course of the processing, which reduces the sensitivity of this measure in terms of examining the components of attention [11-13].
Eye movement recordings can be considered a useful tool to assess attentional biases to visual stimuli, allowing continuous monitoring of attentional orienting and elucidating the different components of attention [14,15]. In visual tasks, eye movements are associated with attentional processes because shifts in gaze position are guided by shifts in attentional focus [16]. In particular, the application of eye-tracking technology can enable researchers to measure the attentional processing of subjects directly, such as the temporal/spatial parameters of the initial orientation and the location of an initial fixation, and can provide information about the subjects’ eye movements.
With selective serotonin reuptake inhibitors (SSRIs), a substantial proportion of patients with MDD respond to pharmacological treatment at week eight [17]. Recent studies suggested that in depressive patients, SSRIs drugs may start to modify attentional biases in emotional information processing [18]. For example, Zhou found that after eight weeks of citalopram treatment, no significant bias towards negative faces was observed in the depressive group [19]. Impairments in the neutral processing of happy facial expressions in depressed individuals were evident in the core area of emotional facial processing, and were reversed following eight weeks of antidepressant treatment [20]. In a neuroimaging study [21] that investigated the responses of depressive patients to fearful facial expressions, those who responded to SSRIs showed a greater reduction in neutral activity across a network of regions, including the anterior cingulate, insula, amygdala, and thalamus after just seven days of escitalopram treatment. Unfortunately, there is a discrepancy between published scientific literature and successful antidepressant treatment in respect to improving cognitive ability, as previous reports have highlighted that poor cognition is a predictor of worsening treatment outcomes [17]. Of note, Wells et al. [22] found depressed participants after taking antidepressant medication demonstrated greater total gaze duration and more fixations for positive stimuli compared to non-medicated depressed participants, however, participants in the study were prescribed a variety of antidepressants (not being given a single dose). Therefore, to clearly understand the impact of depression on attention bias as a whole or its use as a treatment target, depression needs to be characterized by conducting a further attentional test using eye-tracking in both acute and SSRI antidepressant-treated states.
In accordance with previous (behavioral) findings and eye-tracking evidence in MDD, we set a number of goals. First, we examined whether attentional biases are present in depressed individuals, i.e., whether untreated depressed individuals attend less to positive images or attend more to negative images than healthy controls in terms of fixation time and/or frequency. Second, we examined whether attentional biases among depressed individuals were reversed following eight weeks of antidepressant treatment, i.e., whether less attention is paid to negative emotions, while greater attention is paid to positive emotions.
METHODS
Participants
Twenty first-episode depressive patients during minor and major depressive episode were recruited from the First Affiliated Hospital of Anhui Medical University and Anhui Mental Health Center. The 20 healthy participants were recruited from local advertisements to citizens of Hefei City, Anhui Province, China. All participants were matched for age, gender, and years of education (Table 1). Two professional psychiatrists interviewed the subjects using the Chinese Revision of the Structured Clinical Interview for the DSM-IV, and consensus diagnoses were made using all available information. The following exclusion criteria: 1) subjects with other major current and past psychiatric Axis I and Axis II comorbidity such as schizophrenia, bipolar affective disorder; 2) any psychotropic drug used within 4 weeks, alcohol or substance abuse 3) history of substantial physical illness such as head trauma, neurological illness; 4) medical conditions that would contribute to psychiatric symptoms use; 5) having eye problems or difficulties in vision that were not corrected by the use of glasses or contact lenses. Exclusion criteria were the same for the healthy controls as in the patient groups. At baseline, all first-episode patients were antidepressant naive. After 2 weeks of follow-up, the patients received 100-150 mg of sertraline or 10-20 mg of escitalopram per day as their ongoing treatment. A clinical response to the SSRI treatment was defined as exceeding the baseline following eight weeks of treatment [21]. In the patient group, cognitive status was assessed using the Montreal Cognitive Assessment (MoCA) [23] and the assessment of the depressive severity and treatment response was carried out using the Hamilton Depression Rating Scale (HAMD) [24]. Participants provided their written informed consent, and the study was approved by the Anhui Medical University Ethics Committee (20180420).
Apparatus
Gaze location and duration were measured using a remote SMI-RED eye-tracking system (SensoMotoric Instruments, Teltow, Germany), an infrared video-based eye-tracking device which allowed for recording at a frequency of 250 Hz (coordinates were sampled every 4 ms). Visual fixations were defined as eye movements lasting more than 100 ms within a 1° radius of visual angle. The SMI-RED Eye tracker was capable of compensating changes in head position, allowing the participant free head movements across a wide range, so that a head resting device was not required. Two Dell computers, one of which was served as the main test machine, were used to carry out the experimental operations, and the other desktop computer was used to present the experimental materials with a resolution of 1680×960. The tracker was placed beneath the desktop computer screen. Eye movements were monitored through the reflection of infrared light on the cornea and the pupil, which is sensed by the tracker (Supplementary Figures 1 and 2 in the online-only Data Supplement). Prior to the task, we performed a 9-point calibration of the participants using BeGaze software to divide the image interest area and process the gaze information in the area of interest (AOI). BeGaze software (SensoMotoric Instruments, Germany) not only provided qualitative analysis for professional screen-based eye tracking studies, such as single video analysis using gaze replay or scan paths, but also added comprehensive quantitative analytics, with key performance indicators and AOI statistics.
Materials
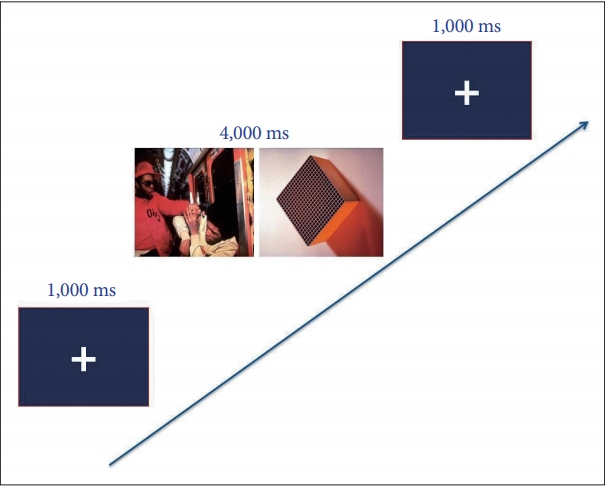
The stimuli included 100 pictures (i.e., 20 positive target pictures, 20 negative target pictures, 20 neutral target pictures and 40 neutral control pictures), which were selected from the International Affective Picture System (IAPS) [25]. Three types of emotional pictures reflected different emotional states in daily life. The happy target pictures depicted people taking pleasure in something or expressing the effect of enjoyment. Negative pictures illustrated people who were seriously threatened or hurt. Neutral pictures expressed people’s daily life or emotionless activities. Control group images showed a variety of inanimate scenes. In each trial, one emotional picture (i.e., positive or neutral or negative) and one control picture were presented together. The order of each trial involving two pictures was randomized, producing three types of emotional trials, i.e., happy-control, negative-control, and neutral-control trials.
Each experiment began with a fixed cross displayed centrally on a 22-inch monitoring computer screen (screen resolution: 1920×1080 pixels), followed by a pair of two pictures, which were presented for 4,000 ms. Participants were requested to view pairs of pictures freely while recording their eye movements. After 4,000 ms of viewing the picture pairs, the pictures disappeared and the fixed cross reappeared at the same time, which indicated the commencement of the next trail. Before the formal experiment, participants were shown the task with six practical trials involving emotional and control pictures. Thus, a total of 80 trials (60 study+20 filler) were presented. Twenty filler trials with two neutral control images were presented to obscure the nature of the task. The experimental design is presented in Figure 1.
Design and procedure
The study employed a case-controlled observational experiment. The sample of first-episode depressive patients (n=20) and healthy controls (n=20) were assessed at baseline using HAMD, MoCA, and an eye movement experiment. Patients were administered SSRIs each morning for a period of eight weeks without an adjustment of the dosage. In respect to the depressive patients group, assessments of attentional bias and treatment response were conducted using the eye-tracking method at baseline, as well as at week eight. Healthy controls included 20 participants who were assessed at baseline only.
Data analyses
In the free-viewing experiment, we computed the following eye movement indicators to reflect the participants’ attention to the pictures: 1) total fixation time (the total duration of the gaze in response to emotional pictures during the 4,000 ms free-viewing period); 2) total number of fixations (the total number of times that each participant fixed and re-fixed on a specific target picture); 3) mean glance duration (average time of each participant’s gaze was maintained within a specific boundary of a target image, i.e., the period of time between when the gaze focused on the image and when the gaze focused away from the image); 4) first-pass fixation duration (the sum of fixation duration of the image when it is first viewed) To investigate group differences in attentional bias at baseline, a 2×3 repeated-measures ANOVA was conducted, with the between-subject factor group (first-episode depression patient group at baseline, control group), and valence (positive, neutral, negative) as within-subjects factors for each eye-tracking indicator (i.e., first-pass fixation duration, total fixation number, total fixation time, and glance duration). To evaluate the therapeutic effects of SSRIs on attentional bias, first, a 2×3 repeated-measure ANOVA was conducted, with the within-subjects factors drug (baseline, eight weeks) and valence (positive, neutral, negative) in the patient group. When the interaction was significant, a paired-samples t-test was carried out to perform planned comparisons, which consisted in within-group comparisons before and after eight weeks of medication treatment. Second, we conducted a 2×3 repeated-measures ANOVA to examine the effect of SSRI treatment, with the between-subject factor group (first-episode patient group after eight weeks of treatment, control group), valence (positive, neutral, negative) as within-subjects factors for each eye-tracking indicator.
RESULTS
Demographic characteristics
Demographic characteristics for participants according to the levels of depression, cognitive function, gender, age, and education are presented in Table 1. The statistical analyses did not reveal any significant differences in gender, age, and education between the two groups.
Attentional bias
Total number of fixations
The ANOVA of the total number of fixations revealed the effect of valence [F (1, 38)=5.82, p=0.008] and the effect of group [F (1, 38)=6.64, p=0.014], which was qualified by an interaction of group×valence [F (2, 76)=15.40, p<0.001]. The simple effect tests on the effects of the groups for each valence revealed significant differences between the groups for the positive pictures (t=-4.73, p<0.001) and negative pictures (t=2.18, p=0.035) (Figure 2A).
Total fixation time
The ANOVA of the total fixation time revealed an effect of group [F (1, 38)=5.72, p=0.02]. Importantly, we found a significant group×valence interaction [F (2, 76)=27.60, p<0.001]. A simple effect analysis of the total fixation time of different emotional pictures revealed statistical difference for positive pictures between the two groups (t=-5.09, p<0.001), suggesting that depressive patients paid less attention to positive emotions compared to the control group (Figure 2B).
Mean glance duration
The analyses showed a significant valence ×group interaction, [F (2, 76) =27.97, p<0.001]. Regarding differences between groups, simple effect tests revealed that, in comparison with the control group, patients showed a higher tendency to fixate on negative pictures (t=4.06, p<0.001) and lower tendency to fixate on positive pictures (t=-4.30, p<0.001) (Figure 2C).
First-pass fixation duration
The ANOVA of the first-pass fixation duration revealed a non-significant effect for group×valence [F (2, 76)=1.88, p>0.05] (Table 2).
SSRIs effects on attentional bias
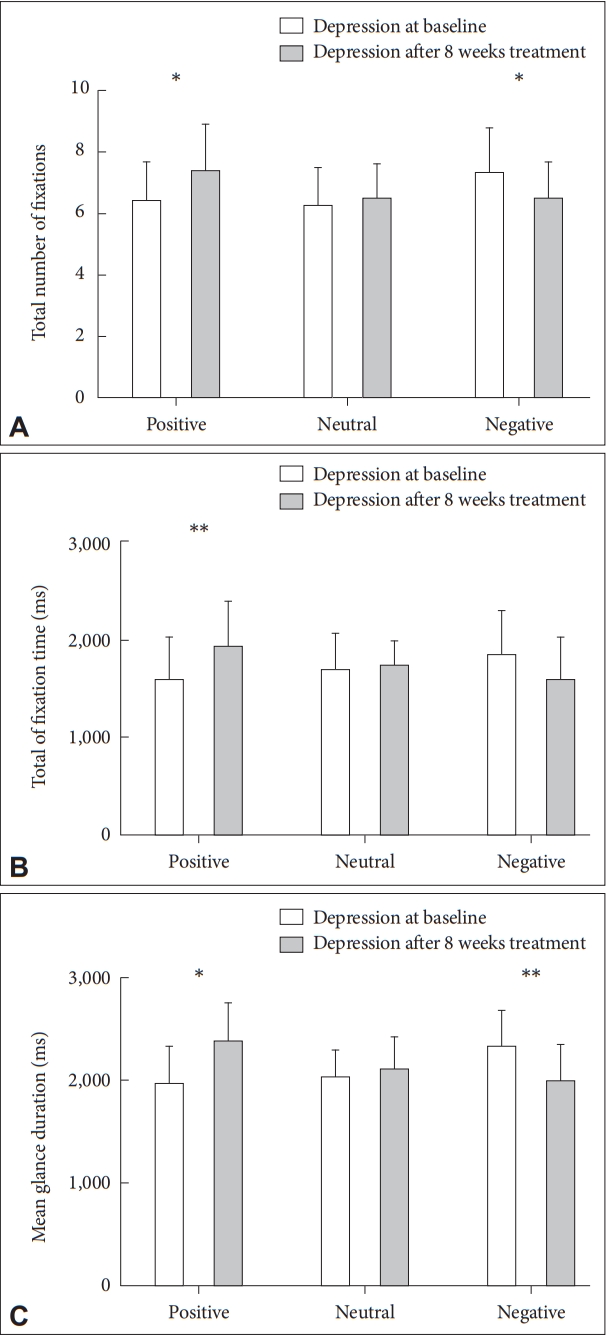
Total number of fixations
A 2×3 repeated-measures ANOVA was conducted to assess the effects of SSRIs on the total number of fixations. A significant within-subjects interaction of drug and valence was found [F (2, 38)=8.95, p=0.003]. A paired-samples t-test revealed that more number of fixations (t=-2.46, p=0.024) for positive pictures, while less number of fixations was found for negative pictures (t=1.98, p=0.048) after eight weeks of SSRI treatment in the patient group (Figure 3A). There was a non-significant interaction between group and valence [F (2, 76)=0.69, p>0.05]. These results indicated that treatment with SSRIs significantly adjusted the attentional bias of depressive patients.
Total fixation time
The ANOVA of the effects of SSRIs in respect to changing attentional bias showed that the interaction of valence×drug was significant [F (2, 38)=14.47, p<0.001]. Following SSRI therapy (eight weeks), the fixation time for positive targets was markedly increased (i.e., paired difference between preand post-treatment: t=-3.26, p=0.004) (Figure 3B). In addition, a 2×3 repeated-measures ANOVA was conducted, with the between-subject factor group, and valence as within-subjects factors for the effect following eight weeks of medication treatment. Neither the effect of group nor the interaction between valence and group approached significance [F (1, 38)=2.34, p>0.05; F (2, 76)=0.59, p>0.05]. This result indicated that attention to positive pictures in medicated depressive patients was close to “normal” when compared to controls.
Mean glance duration
The ANOVA results revealed that the interaction of valence×drug was significant [F (2, 38)=18.29, p<0.001]. To explore this difference in the patient group, a paired-samples t-test was carried out, revealing a longer fixation time for positive pictures (t=-4.33, p=0.015), while a shorter fixation time was found for negative pictures (t=2.81, p=0.01) (Figure 3C). Furthermore, the results of the analyses showed a non-significant valence×group interaction after eight weeks of SSRI treatment, [F (2, 76)=1.78, p>0.05].
First-pass fixation duration
The interaction of valence×drug was not significant between pre- and post-treatment in the depressive patients group [F (2, 38)=2.12, p>0.05] (Table 2).
Correlations of eye-tracking variables with HAMD scores
We also examined the relationship between eye-tracking parameters and clinical severity, which was measured using HAMD. Specifically, the bias scores for the negative images (i.e., the total number of fixations and glance duration) were significantly correlated with the participants’ mood symptoms (r=0.35, 0.39; p=0.039, 0.044). In addition, depressive symptoms were associated with the happy images bias in respect to the total fixation time and glance duration (r=-0.36, -0.43; p=0.03, 0.009). This is consistent with the idea that clinical severity plays a major role in the emotion-related attentional biases in depressed individuals.
DISCUSSION
The current study examined the effects of SSRIs on attentional bias in depressive patients by carrying out a free-viewing eye-tracking experiment. The key findings can be summarized as follows. First, the initial orientation of all participants (both patients and healthy controls) was determined: First-episode depressive patients oriented their gaze more frequently to negative images and less to happy images, compared to controls. Second, the attentional bias in depressive patients was regulated following eight weeks of SSRI treatment. Patients showed an increased tendency to fixate on positive pictures and a decreased tendency to fixate on negative pictures. In the SSRI-medicated depressive patients, attention to emotional pictures (positive and negative) was close to “normal” when compared to controls. Furthermore, the attentional biases of depressive patients were associated with clinical severity.
In respect to the nature of emotional biases in depressive patients, the biases toward positive and negative images were state-dependent. On the one hand, comparable to patients with bipolar disorder in the depressive phase [26], depressive patients paid less attention to the positive images than the control group, as deduced from the total fixation time, total number of fixations, and glance duration found for these images. On the other hand, in comparison to healthy controls, depressive patients paid more attention to negative images in terms of the total number of fixations and glance duration, and this result was similar to previous eye-tracking studies with individuals with major depressive disorder [27-29]. According to Beck’s cognitive vulnerability-stress theories [5], dysfunctional cognitive structures in individuals with depression may condition the attentional preferences and constitute a general vulnerability factor. This negative attentional bias toward threatening information could increase the emotional reactivity of depressive patients, and may contribute to the onset or exacerbation of an affective episode when people with depression experience stressful life events. In depressive patients, the high emotional reactivity to stressful events, influenced by a hypervigilance to threatening stimuli, affected the formation and continued progression of depression [5,30].
Previous studies found that serotonin plays an important role in the processing of affective stimuli and inhibitory control of behavior and adaptation [31], and in healthy volunteers, lowering brain serotonin level results in increased sensitivity to punishment and negative feedback without affecting reward [32,33]. These results highlight that in depressive patients, a decrease in serotonin concentration could lead to an attentional bias toward negative stimuli and away from positive stimuli [34,35]. A study found that depressive patients who were administered SSRIs received significantly less information from negative feedback than medication naïve depressive patients, which indicated that SSRI antidepressants diminish the capacity to learn from negative feedback [36]. Similar to our findings, following eight weeks of escitalopram treatment, no significant attentional bias toward negative faces was observed in depressive patients, using a dot probe task of facial expressions [19]. A body of research results suggest that these alterations in emotional processing highlight the effectiveness of SSRIs in acting on a neutral modulation circuit, which is strongly innervated by serotonin, namely, the limbic and prefrontal cortex (PFC) [37,38].
Recent imaging studies argued that depressive patients who went on to respond to SSRIs experienced a greater decrease in neutral activity, observed across a network of regions, including the anterior cingulated and amygdale [39,40], in response to facial expressions of fear and pleasure after just seven days of escitalopram treatment [21]. Short-term administration of SSRIs can regulate PFC responses to negative self-reference stimuli in individuals at a high risk of depression [41]. Therefore, early modification of negative bias may play a key role in the drug action of SSRIs and is a potential predictor of therapeutic response. In addition, the drug action of SSRIs normalizes the blood-oxygen-level-dependent (BOLD) response in the PFC and the functional connection between PFC and amygdala [36]. The PFC and limbic-cortical regions constitute the key nodes of depression models, and functional neuroimaging studies have identified these regions as the basis of negative bias on emotional processing in depressive patients [42]. The above results show that antidepressants modulate emotional processing, increasing positive emotional attention and reducing negative attentional bias.
In a previous study using a dot-probe task [43], we demonstrated that attentional biases in the processing of emotional facial expressions are evident (e.g., participants selectively attended to sad faces, which indicated a positive bias that was not observed) in remitted depressed patients. This investigation of an attentional bias in formerly depressed participants suggested that cognitive biases are stable beyond the depressive episode. In contrast, our results showed an increased tendency to fixate on positive pictures and a decreased tendency to fixate on negative pictures in treated depressed patients. This may be partially due to the difference in the depression status in the former study and the present study. In the former study, remitted depressive patients were selected to examine the attentional bias and were compared to controls. It is possible that sad expressions capture attention in remitted depressive patients who are concerned about becoming depressed again in the future because such negative stimuli relate to their own concerns. In addition, in the former study, a behavioral experiment (dot-probe task) was conducted to examine the attentional bias between remitted depressive patients and controls, whereas a free-viewing eye-tracking task was used to directly investigate the difference in attentional function in treated depressive patients and controls. Although behavioral experiments offer useful information on underlying emotional processing, there is an inherent limitation in respect to response times. Response times from behavioral experiments do not inform us about the time course of the underlying attentional processes. However, eye movements are related to attentional processes during visual tasks and provide an online measure of emotional processing.
Our study illuminates the relationship between attentional bias and clinical severity in depression. Consistent with the several prior studies [44,45], severity of depressive symptoms was positively associated with negative images bias, in contrary, negatively associated with happy images bias. Interesting, Wells et al. [46] found that attention training could lead to a reduction in depressive symptoms while subjects in the no training condition experienced relatively little change. The results of this study bolster the argument that, selective attention bias for negative images plays a key role in the maintenance of depressive symptoms.
From the point of view of the relevant statistical data, after 8 weeks of treatment, total fixation time on negative image in depression showed a declining trend. However, the difference is not statistically significant. A major limitation of the current study is the relatively small sample size of 20 first-episode depressive patients, so the research results should be considered as strictly. Another limitation relates to the fact that the attentional bias in depressive patients was regulated after SSRI treatment at the eye-tracking level. Further investigations should employ a wide range of experimental tasks and designs, as well as recording methodologies in order to facilitate a more comprehensive understanding of brain networks underlying the relationship between depression and attentional processing.
In summary, our study demonstrated that first-episode depressive patients oriented their gaze more frequently to negative images and less to happy images, compared to controls. Importantly, the present study provides key evidence that following eight weeks of antidepressant treatment, the attentional bias changes in first-episode depressive patients, who showed an increasing tendency to fixate on positive pictures and a decreasing tendency to fixate on negative pictures. These observations may be relevant for the development of improved therapeutic approaches to depression.