INTRODUCTION
Auditory verbal hallucinations (AVHs) that are the most characteristic symptom of schizophrenia [1-3], have multidimensional aspects that are mostly assessed with interviewer-rated scales, such as the Psychotic Symptom Rating Scales-Auditory Hallucination Subscale (PSYRATS-AHS) [4,5]. However, quantitative indicators of PSYRATS-AHS do not correlate well with the subjective distress [4,6,7]. Studies indicate that patients can report AVHs reliably [8-10], and self-reported outcomes can inform clinical practice [11,12]. The Hamilton Program for Schizophrenia Voices Questionnaire (HPSVQ) is a self-report scale that includes domains similar to those of PSYRATS-AHS [7,8,13]. HPSVQ is characterized by good psychometric properties and sensitive enough to changes in AVHs [8].
Though clozapine is highly effective for reducing AVHs [4], more than 25% of patients still suffer from AVHs despite adequate clozapine treatment [1,14-17]. Persistent AVHs are associated with increased violence, hospitalization, risk of suicide [18], and low likelihood of future recovery [19,20]. Despite this, there are few long-term follow-up studies on the subjective experience of AVHs in clozapine-medicated patients [15].
The aim of this retrospective study was to explore longitudinal changes in AVHs assessed with HPSVQ in patients with schizophrenia who had been treated with clozapine. We also investigated the effects of various factors on long-term change trajectories.
METHODS
Subjects
Patients with schizophrenia suffering from AVHs between 20 and 65 years of age were recruited. The eligible subjects were patients who met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition Text Revision criteria of schizophrenia, had been treated with clozapine, and assessed with HPSVQ more than twice during the observation period from March 2012 to February 2016. This study was approved by the Institutional Review Board of Dongguk University International Hospital (#2016-125).
The HPSVQ
HPSVQ was developed as a 13-item self-report questionnaire on a 5-point Likert scale to address the subjective effects of AVHs [7]. The total score of the first 9 items was taken as the severity of subjective distress. The Korean version of HPSVQ were in good agreement with PSYRATS-AHS and the Positive and Negative Syndrome Scale (PANSS)-P3 item, and also showed good test-retest reliability and internal consistency [8]. In our previous study, two factors of HPSVQ were identified and named as physical and emotional factors, respectively [8].
Statistical analysis
Demographic and clinical characteristics were evaluated at baseline. Longitudinal changes of the total and factor scores of HPSVQ were modeled using linear mixed-effect regression. The effect of the covariates on the overall mean of the response variables, and on the slopes of time-dependent changes were evaluated. The right-skewed variables such as duration of treatment (DOT) with clozapine and duration of illness were log-transformed. The significance of the calculated coefficients was tested by the Wald t-test.
The observation periods of the patients were not homogeneous and several patients were lost during the study period. Thus the Cox proportional hazard model was employed to adjust for the censored data. It could estimate the effect of covariates on the proportional hazard ratios. The target event was defined as an at-least 50% reduction in the total HPSVQ score from the baseline. The first point of measurement when the HPSVQ score was less than half the baseline was regarded as the time to the event for each subject. The appropriateness of the proportional hazard assumption was checked using the goodness-of-fit test based on Schoenfeld residuals. All statistical analyses were performed using R software (ver. 3.2.4: R Project for Statistical Computing, Vienna, Austria) [21]. A p-value<0.05 was considered significant.
RESULTS
Demographic and clinical characteristics
Among the 55 subjects originally participated in the study, 11 patients with HPSVQ total scores ≤7 (indicating absent-to-minimal AVHs) [8] at baseline were excluded. The data of remaining 44 patients were summarized in Table 1. No significant differences in the demographic and clinical information were detected between the excluded and analyzed patients.
Longitudinal changes in the HPSVQ
The mean total score of HPSVQ was significantly decreased from 16.2±5.6 at baseline to 10.4±8.6 at the last observation (t=4.441, p=0.000 by paired t-test). All items except “interference with life” and two factor scores of HPSVQ decreased significantly during the observation period.
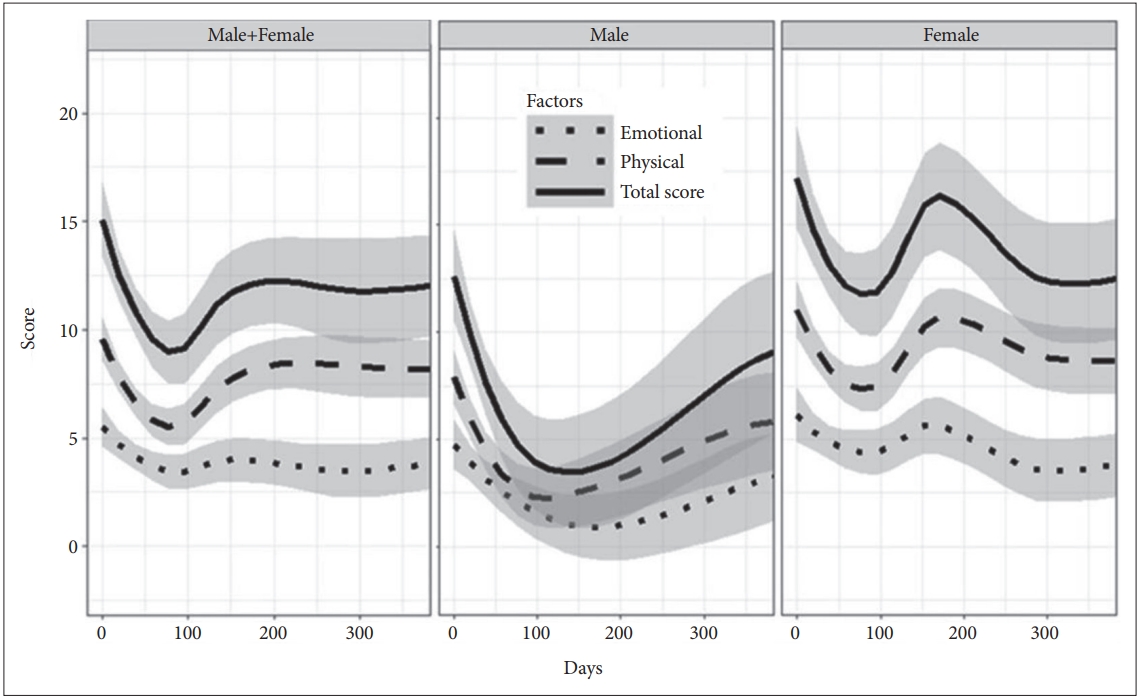
The trajectories of the total and factor scores of HPSVQ were visually inspected. All three scores changed markedly during the first year of the observation period, but the emotional factor did not show such a noticeable change. Formal statistical tests with linear mixed-effect regression also supported such findings. Total score decreased by 9.2 points per year [t(263)=-3.60, p=0.0004], the physical factor score by 5.8 points per year [t(263)=-3.64, p=0.0003], and the emotional factor score by 3.4 points per year [t(263)=-2.476, p=0.0139].
Gender exerted a significant effect on the overall mean of total score [t(40)=2.16, p=0.037] and physical factor score [t(40)=2.05, p=0.047], but not of the emotional factor score [t(40)=1.72, p=0.094]. Female patients reported more AVHs and more severe distress than males. And the log-transformed DOT with clozapine had a significant effect on the HPSVQ scores [total score: t(40)=2.86, p=0.0067, physical factor score: t(40)=2.61, p=0.013, emotional factor score: t(40)=2.39, p=0.019]. The coefficients indicate that if DOT was doubled then the total, physical and emotional factor scores would increase by 1.09, 0.59, and 0.51 points, respectively.
Gender also had a significant modifying effect on the time-dependent changes in total and physical factor scores. It was estimated that the increases (per year) in the total and physical factor scores were 6.48 and 3.70 points higher in female patients than in males, respectively.
Time-to-event analysis using Cox proportional hazard regression
Only 21 patients reached the pre-defined threshold for the event (47.8%) during the 1-year observation period, therefore the first quartile (25%) survival time was calculated (35 days) instead of the median. DOT with clozapine had a significant effect on the hazard ratio of reaching the event (z=-2.69, p=0.007). The coefficient suggests that doubling the DOT with clozapine decreased the likelihood of reaching the event by 24%. Figure 1 shows the adjusted survival curves for the Cox proportional hazard model. The survival curves of the patients with a longer DOT with clozapine were shifted significantly upwards, suggesting a lower likelihood of reaching the threshold for the event.
DISCUSSION
We demonstrated that subjective aspects of AVHs evaluated with HPSVQ gradually improved during a 3-year observation period in patients with clozapine treated schizophrenia. Female patients and patients with longer DOT were more resistant to the effect of clozapine. This result indicated the beneficial effect of clozapine on AVHs [14-16], particularly on subjective dimension.
Similarly looking item questionnaire can elicit quite different aspects of personal experience according to the method of assessment [22]. For example, the item “interference with life” of HPSVQ have not signiticantly decreased during the observation period. In our previous study, the item “disruption to life” of PSYRATS-AHS showed a gradual reduction during the 6 months of observations [10,15], wherease, the “interference with life” of HPSVQ remained unchanged during the 1 year follow-up [23]. Moreover, the present study showed that, unlike the physical factor, the emotional factor was quite resistant to change. These findings are consistent with the previous reports that emotional disruption could not be easily improved despite long-term treatment [24,25]. These results supported the distinctive value of self-report in AVHs researches.
The time-dependent changes were not even during the observation period; the total and physical factor changed markedly during the first year of observation and reached plateau thereafter, whereas the emotional factor did not change much during the early phase. The likelihood of HPSVQ total score improvement decreased by 24% with a doubling of DOT with clozapine. This is consistent with previous reports that longer-lasting AVHs increased the likelihood of becoming refractory [1,26]. Taken together, the physical dimention of AVHs seemed to respond earlier but to become more and more resistant, while the emotional dimension seemed to take more time to meaningful improvement.
Several limitations should be mentioned. First, the number of patients was small for tracking long-term course of AVHs, the numbers and intervals of the assessments were inconsistent. Second, the doses of clozapine and the other psychotropics were not controlled during the study; this may have affected the psychotic symptoms of the patients, although only patients treated with clozapine were included.
In conclusion, self-report AVHs in patients with schizophrenia using clozapine decreased markedly in the early phase of observation, fluctuated thereafter, but eventually decreased. Female gender and DOT with clozapine had negative associations with the degree of HPSVQ improvement. Further studies are needed to clarify why the decrease in the emotional factor was less marked and took more time to improve with clozapine treatment.