INTRODUCTION
Panic disorder (PD) is an anxiety disorder characterized by unexpected and recurrent panic attacks [1]. In addition to panic attacks, PD has two core symptoms, maladaptive behaviors related to panic attacks and repetitive worries about them, known as anticipatory anxiety [2]. Recurrent and unpredictable panic attacks are associated with persistent anticipatory anxiety, which exacerbates the development of PD [3]. In this context, the ability to predict and anticipate situations plays an important role in the progression of PD.
Intolerance of uncertainty (IU) is a dispositional inclination to react negatively to unknown situations and events at emotional, cognitive, and behavioral levels [4]. IU was initially used to distinguish individuals with a generalized anxiety disorder from healthy individuals [5], but research has subsequently been conducted on its association with other anxiety disorders, such as social anxiety disorder [6-8], post-traumatic stress disorder [9,10], and obsessive-compulsive disorder [11,12].
Furthermore, studies on the relationship between PD and IU have also been conducted owing to these characteristics. In a previous study, the PD patient group had higher IU Scale (IUS) scores than the healthy control group [13], and the IU inhibitory factor demonstrated a significant correlation with the severity of panic symptoms [14]. Anxiety plays a role in altering attentional processes when coping with threatening stimuli [15]. Anxious individuals tend to interpret ambiguous and neutral stimuli as threatening, which is known as an “interpretation bias.” [16] Patients with PD have a negative cognitive tendency to interpret ambiguous physiological sensations, which can be a risk factor for disease progression [17].
The neural pathways associated with IU have been studied to understand these cognitive processes. Numerous studies have been conducted to enhance understanding of the neurological basis of IU. Many functional magnetic resonance imaging (MRI) studies have demonstrated a positive correlation between anterior insula activity and IU [18-21]. Additionally, associations between anterior cingulate cortex and amygdala activity have also been observed [22,23]. It is widely accepted that PD involves the disruption of the fear circuit centered around the amygdala [24,25]. The interconnectedness between the amygdala, insula, and anterior cingulate, with the amygdala at its core, integrates sensory and bodily inputs and their interpretation of these inputs.26,27 Hypervigilance toward anticipated threats and responses is associated with amygdala overactivity [28], which is richly connected to the orbitofrontal cortex, ventral striatum, and sensory cortex [29]. The alteration of these connections makes it difficult to distinguish between safe and threatening situations, and this uncertainty is thought to be associated with anxiety [30]. In addition, there are studies that have shown associations between IU and brain structural changes. Hilbert et al. [31] reported a positive correlation between IU and gray matter volume (GMV) in the right temporal gyri in individuals with generalized anxiety disorder. Additionally, Kim et al. [32] found a positive correlation between striatal volume and IU in healthy participants.
However, little research has been conducted on structural changes in the brain associated with IU in patients with PD, and even less is known about how these structural changes affect actual functioning. Therefore, this study aimed to investigate the brain regions and structural associations of IU in patients with PD, as well as the impact of these structural alterations on clinical outcomes.
METHODS
Participants
Ninety participants with PD, aged between 18 and 66 years, were included in the current study. The participants were recruited from the Department of Psychiatry at CHA Bundang Medical Center between December 2013 and June 2020. All participants were right-handed Koreans and underwent MRI. Qualified psychiatrists diagnosed PD using the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [2].
The exclusion criteria were as follows: a primary diagnosis of schizophrenia, anxiety disorders other than PD, major depressive disorder, substance use disorder, or mental retardation. Participants who were unable to undergo brain MRI were excluded.
The study protocols followed the Good Clinical Practice guidelines and were approved by the CHA Bundang Medical Center’s Institutional Review Board (no. 2019-05-030, 2021-05-055). Written informed consent was obtained from all participants after they were given a thorough explanation of the study.
Assessments
To evaluate negative reactions to uncertainty, the Korean version of the IUS-Short Form (IUS-12) was used. The original scale, the IUS, was created by Freeston in 1994. Later, Carleton et al. [33] developed and validated a shortened 12-item, two-factor version of the scale in 2007. The scale is measured on a 4-point Likert scale and consists of 12 items that evaluate responses to uncertainty, ambiguity, and the future. Cronbach’s α for the Korean version of the IUS-12 was 0.94 [34].
To assess the severity of the participants’ baseline anxiety and depression, the Panic Disorder Severity Scale (PDSS) [35], Beck Depression Inventory-II (BDI-II) [36], Beck Anxiety Inventory (BAI) [37], and Penn State Worry Questionnaire (PSWQ) were used [38].
The PDSS consists of items that assess PD and seven panic-associated symptoms. The Korean version of the PDSS has demonstrated strong reliability, validity, and internal consistency (Cronbach’s α=0.89) [39]. The PSWQ is a tool used to measure pathological levels of anxiety and worry. The Korean version of the PSWQ has shown good internal consistency (Cronbach’s α=0.90) and factorial validity [40].
The BDI is one of the most commonly used screening tests for depression, evaluating depressive symptoms over the past two weeks. The Korean version of the BDI has shown high internal consistency (Cronbach’s α=0.94) and proper validity [41]. The BAI is a tool used to measure anxiety. The Korean version of the BAI has demonstrated favorable internal consistency (Cronbach’s α=0.90) and validity [42].
The Self-Forgiveness Scale (SFS) was used to evaluate dispositional self-forgiveness. The SFS comprises three subscales: “acceptance and improvement,” “transferring responsibility,” and “negative affect, thoughts, and behavior.” The Korean version of the SFS has demonstrated adequate validity and high internal consistency (Cronbach’s α=0.87) [43].
Additionally, to measure perceived life satisfaction, the Korean version of the Short Form 36 Health Survey (SF) was used. The SF measures health-related quality of life and is categorized into eight domains: physical functioning, social functioning, physical role, emotional role, mental health, vitality, bodily pain, and general health [31]. The Korean version of the SF has shown satisfactory content and discriminant validity, with Cronbach’s α ranging from 0.71 to 0.90 [44].
Neuroimaging data acquisition
All subjects underwent MRI using the 3T GE Signa HDxt scanner (GE Healthcare, Milwaukee, WI, USA) with an eight-channel phase-array head coil. The settings for acquiring T1-weighted fast spoiled gradient recalled echo images in the three dimensions were as follows: 6.3 ms repetition time; 2.1 ms echo time; 12° flip angle; 1 mm slice thickness; 25.6 cm field of view; 256×256 matrix; and 1×1×1 mm3 isotropic voxel size.
To analyze GMV and cortical thickness (CT), FreeSurfer v7.1.0 (http://surfer.nmr.mgh.harvard.edu) was used. Image processing was performed as follows: motion correction, intensity normalization, skull stripping, white matter segmentation, gray/white matter border tesselation, automated topology correction, and surface deformation. Previous studies have provided descriptions of the specificities of these methods in detail [45-47]. The cortex was auto-parcellated into 34 separate gyral regions per hemisphere utilizing gyral and sulcal architecture using the Desikan-Killiany atlas [48-50].
Statistical analysis
Age, sex, and the total intracranial volume (ICV) were included as covariates in the multiple regression models. We conducted the Monte-Carlo simulation to correct for multiple comparisons in cluster-wise correction.
In addition, to identify the significance of the CT in the brain correlates of the IUS and its associations with the psychological characteristics of patients with PD, an exploratory correlation analysis was performed. Pearson’s correlation analysis was performed using the IBM Statistical Package for the Social Sciences Windows software version 27 (IBM Corp., Armonk, NY, USA). A p-value of 0.05 or less was regarded as statistically significant.
RESULTS
Sociodemographics
Of the 90 participants with PD, 45 (50.0%) were male, and 45 (50.0%) were female (Table 1). The mean age of the participants was 37.92 years (standard deviation [SD]=12.57), and the mean number of years they spent in school was 14.61 (SD=2.29). A summary of the sociodemographic characteristics is presented in Table 1.
Association between IUS and gray matter structural alteration
In PD, there was a significant negative correlation between the total IUS scores and the CT in the right lingual gyrus (peak voxel of MNI: X=15.4, Y=-74.5, Z=-6.5; Monte Carlo simulation correction, cluster-wise p<0.05) (Figure 1A). There was also a significant positive correlation between the total IUS scores and GMV in the right pars triangularis (peak voxel of MNI: X=39.1, Y=33.8, Z=9.0; Monte Carlo simulation correction, cluster-wise p<0.05) (Figure 1B). After controlling for variables including age, sex, and ICV, statistical significance was maintained.
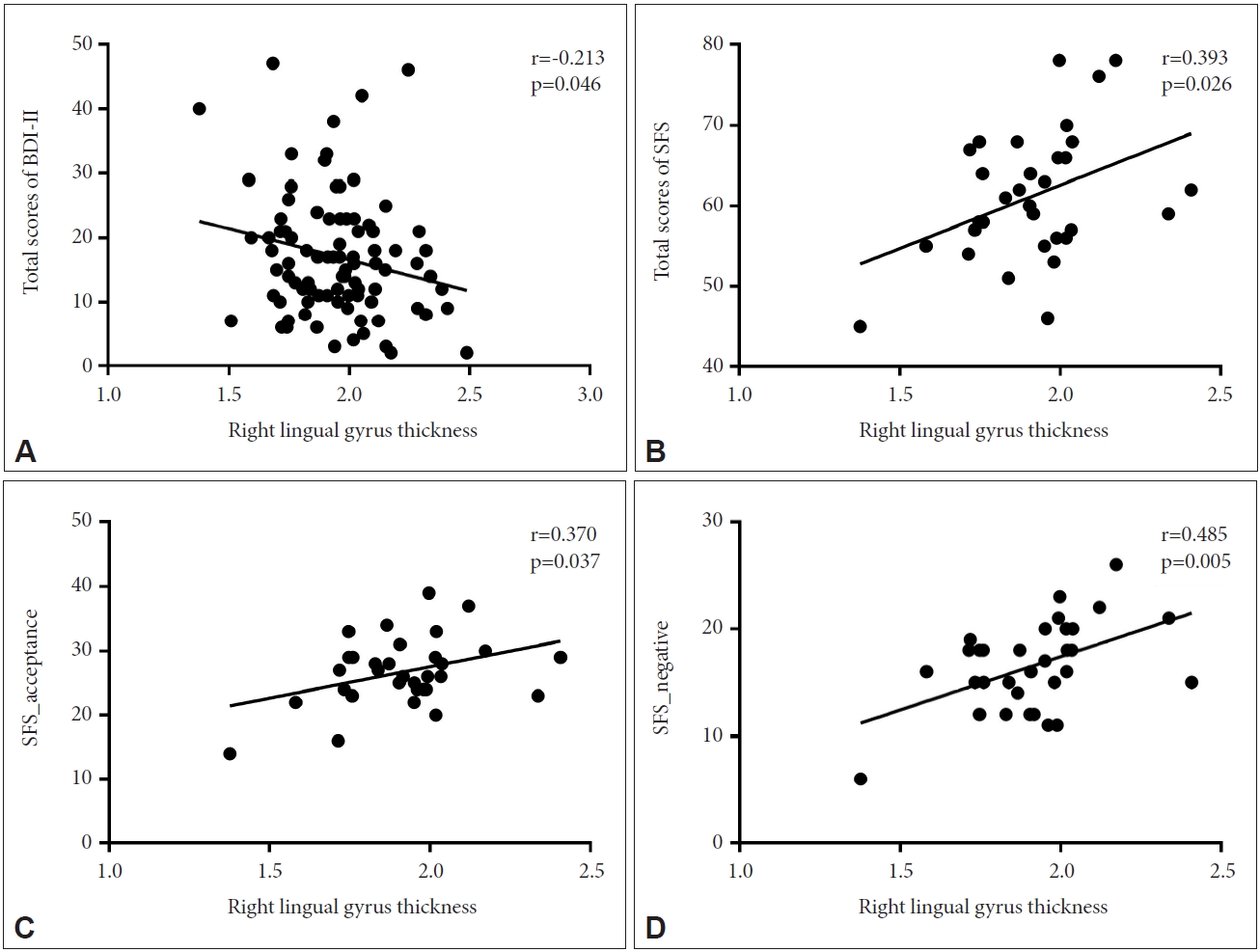
Correlation between the mean CT in the right lingual gyrus and clinical scales of PD
In participants with PD, exploratory correlation analysis showed significant negative associations between the CT in the right lingual gyrus and the total BDI-II scores. In addition, strong positive correlations were found between the CT in the right lingual gyrus and the total scores of the SFS and SFS subscales (negative emotional status and acceptance) (Figure 2).
Correlation between the GMV in the right pars triangularis and clinical scales of PD
In addition, there was a significant negative correlation between the GMV in the right pars triangularis and the mental health domain of the SF. There was a positive correlation between the GMV and the baseline total scores on the PDSS, PSWQ, and BDI-II, and the transferring responsibility subscales of the SFS (Figure 3).
DISCUSSION
This study investigated the structural brain alterations associated with IU and the associated psychological characteristics in patients with PD. Although the regions identified in previous structural-based studies did not show significant differences in the present study, it is important to note that this study employed a whole brain analysis approach specifically targeting patients with PD. Considerable amount of research has provided evidence that IU is a transdiagnostic dispositional risk factor for the development and maintenance of clinically significant anxiety [19,31,51]. Growing evidence indicates that IU is associated with a broad range of emotional disorders and other cognitive vulnerability factors [52,53], highlighting the theoretical and therapeutic importance of IU. Recent researchers argue that disorder-specific IU is more strongly related to symptoms of disorder than general IU trait [54]. This difference sets the present study apart from previous studies and provides a unique perspective on the neural correlates of PD. In patients with PD, high IU was significantly correlated with lingual gyrus thinning and increased GMV in the pars triangularis. Furthermore, the CT of the lingual gyrus was negatively correlated with subjective depression, whereas self-forgiveness and the tendency to accept mistakes and avoid negative aspects were positively correlated. The GMV in the pars triangularis was positively correlated with excessive anxiety levels, depression, and a sense of personal responsibility for mistakes but negatively correlated with mental health satisfaction.
In this study, a higher IUS score in patients with PD was associated with decreased CT in the lingual gyrus. Due to their sensitivity to environmental changes, patients with PD tend to perceive even secure situations as threatening [55], which may be a precipitating factor in PD [56,57]. According to previous studies, as part of the visual cortex, the lingual gyrus is associated with the amygdala, modulates spatial attention and fear responses [58], and is hyperactive in response to uncertain stimuli [59]. Therefore, errors in the interpretation of sensory information in the visual cortex, including the lingual gyrus, may play a significant role in the hypervigilance of neutral stimuli.
This study also found that high IU levels in patients with PD were associated with greater GMV in the pars triangularis. These findings align with previous research that has shown an association between IU and increased volume in the superior temporal pole, which is involved in affective face processing [31]. Part of the ventrolateral prefrontal cortex, the pars triangularis, is associated with affective regulation and fear conditioning in patients with PD [60,61]. The right inferior frontal gyrus is also involved in detecting behaviorally relevant stimuli that are salient or unexpected [62]. Previous research by Weilnhammer et al. [63] demonstrated that the inferior frontal gyrus contributes to the interpretation of ambiguous sensory stimuli via feedback processes with the visual cortex [63-66]. Based on these findings, structural alterations in the pars triangularis and the lingual gyrus may result in erroneous interpretations of uncertain stimuli and anxiety [66].
Thinning of the lingual gyrus, which is associated with high IUS scores, is associated with severe depressive symptoms, whereas an increase in the volume of the pars triangularis is positively correlated with PDSS, PSWQ, and BDI-II scores. This is consistent with a meta-analysis conducted by Arnone et al. [67] that demonstrated a significant decrease in the gray matter density of the lingual gyrus in patients with depression [67,68]. In addition, previous studies on patients with PD have demonstrated a positive correlation between the pars triangularis CT and the severity of panic symptoms, supporting the findings of this study [69].
Thinning of the lingual gyrus and increased size of the pars triangularis appeared to diminish life satisfaction. Numerous studies have demonstrated that IU is associated with coping styles, resilience, forgiveness, self-compassion, and lower quality of life, as higher IU levels tend to be associated with lower life satisfaction [70-73]. This is thought to be due to a genetically susceptible brain structure that increases “interpretation bias” toward neutral stimuli, making individuals hypervigilant, which exacerbates anxiety and depressive symptoms and results in a decline in quality of life [16].
This study has several limitations. First, because this study was limited to patients with PD, generalizing the results to the general population may be challenging. Nevertheless, this study provides a convincing explanation for the neural basis of IU in PD. Second, because this was a cross-sectional study, it could be difficult to establish causality between the results. Therefore, further research may be required to investigate the changes in IUS over time and the accompanying structural alterations in the brain.
In conclusion, the results of our study indicate that elevated IU in patients with PD is associated with cortical thinning in the lingual gyrus and increased volume in the pars triangularis, which may be related to high levels of individual depression and anxiety as well as decreased quality of life. This indicates that the lingual gyrus and pars triangularis may contribute to interpretation bias, resulting in hypersensitivity to neutral stimuli and increased IU in uncertain situations. These findings enhance the neurological comprehension of PD-specific anticipatory anxiety and IU.