INTRODUCTION
The acceptance and commitment therapy (ACT) model of psychopathology proposed the six ŌĆ£inflexibilityŌĆØ processes that produce human suffering and psychopathology such as experiential avoidance, cognitive fusion, inflexible attention, fusion with self-concept, remoteness from values, and unworkable action [1,2]. From an ACT perspective, patients with obsessivecompulsive disorder (OCD) show cognitive fusion in their obsessions that leads to evident experiential avoidance and unworkable behavior including ritualizing, avoidance, and other control strategies [3]. Accumulating evidence shows that ACT is an effective treatment for OCD [4-8]. One recent metaanalysis revealed that ACT was more effective than other types of treatments with a medium to large effect size [8]. However, considering the heterogeneity of OCD [9], the efficacy of ACT across any types of obsessive-compulsive (OC) symptoms remains unclear.
One may assume that ACT can be effective across symptoms within OCD since it is fundamentally transdiagnostic [10]. In fact, one of the initial studies showed that the therapeutic responses were similar regardless of the specific type of compulsions, including checking, cleaning, and hoarding [11]. Further, a few studies have found that ACT is effective against specific symptoms, such as scrupulosity (symptoms related to moral or religious issues) [12] and symmetry (perfectionism) [13]. However, although most studies in this field included all subtypes of OCD, they only reported overall improvement across various symptom types. In the same context, several studies with no ACT intervention have investigated the association between ACT processes and OC symptom dimensions, and assumed its efficacy against a certain symptom dimension when the ACT process associated with a given symptom dimension can be handled [14,15]. For example, previous studies have revealed that experiential avoidance was correlated with responsibility for harm and unacceptable thoughts, but not with contamination dimension [14,15]. However, to the best of our knowledge, no studies have investigated the association between ACT processes and individual symptom dimensions using longitudinal data before and after ACT intervention. Moreover, finding a group of symptoms that respond well or poorly to ACT and testing the actual therapeutic effect of ACT across OC symptom dimensions have important clinical significance. Thus, the current study aimed to evaluate the efficacy of ACT on the four empirically supported symptom dimensions. Further, the association between changes in ACT processes and those in individual symptom dimensions after ACT was investigated.
METHODS
Participants
Patients with OCD aged 18-55 years were recruited via advertisements in subway, online boards, and psychiatric clinics at Kyungpook National University Hospital. The Structured Clinical Interview for DSM-5, Clinical Version [16] was used to obtain clinical diagnosis. Patients with acute medical or neurological disorders that could affect cognitive function, intellectual disability, a history of brain trauma, or other major psychiatric illnesses, including major depressive disorder, and schizophrenia, were excluded from the study. After screening and providing a written informed consent, the patients received group-format ACT (GACT). Participants were allowed to receive pharmacotherapy as usual. Overall, 75 participants agreed to participate in the ACT intervention and 11 dropped out due to academic and work problems for 6, health problems for 2, and lack of motivation for 3. In the final analysis, 64 participants (including 30 females, age: 27.1┬▒7.9 years) who received six or more sessions and completed assessments before and after treatment were included. Table 1 shows the baseline demographic and clinical characteristics of the participants. This study was approved by the Institutional Review Board of Kyungpook National University Hospital (2021-04-032).
GACT program and psychological measures
An 8-week GACT program [17] was administered, which comprised 90-min weekly sessions. Each GACT group included 3-5 participants. A detailed description of the GACT protocol is provided in a previous study [5].
All measures were evaluated before and after the 8-week treatment. The Dimensional Obsessive-Compulsive Scale (DOCS), which is the primary measurement tool, was used to assess OCD severity across the four symptom dimensions (i.e., contamination, responsibility for harm, unacceptable thoughts, and symmetry) [18,19]. The self-report version of the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) was also used to assess OC symptom severity [20,21]. The Acceptance and Action Questionnaire-II (AAQ-II) [22,23], Acceptance and Action Questionnaire for Obsessions and Compulsions (AAQOC) [24], and Cognitive Fusion Questionnaire (CFQ) [25,26] were used to assess general psychological inflexibility, psychological inflexibility related to intrusive thoughts, and cognitive fusion among ACT processes of psychopathology. Moreover, the Beck Depression Inventory was used [27,28].
Statistical analyses
Demographic characteristics were presented as descriptive statistics. The Kolmogorov-Smirnov test was used to assess the normality of the distribution of all scales (Supplementary Table 1 in the online-only Data Supplement). Although some scales and subscales were not normally distributed, parametric statistics were used considering the sample size and consistency with the reporting method of previous effectiveness studies. The paired t-test was used to determine whether changes in symptom and process measures between pre- and posttreatment were significant and to calculate the effect sizes (CohenŌĆÖs d) of the four OC symptom dimensions. Zero-order and partial correlation analyses controlling baseline depression score were performed to assess the relationships between changes in symptom and process measures. A series of regression analyses were performed to examine the contributions of the three scales for ACT processes in predicting the four individual OC dimensions. Changes between pre- and posttreatment in AAQ-II, AAQ-OC, and CFT scores as independent variables and individual domain scores of the DOCS as dependent variables were included. All data analyses were performed using IBM SPSS Statistics for Windows (version 23.0; IBM Corp., Armonk, NY, USA).
RESULTS
Efficacy of GACT on overall OC symptom and individual symptom dimensions
After 8 weeks of GACT, participants showed significant improvement in overall OC symptoms, as measured by Y-BOCS (from 22.8┬▒6.2 to 18.1┬▒6.8, CohenŌĆÖs d=0.83) (Table 2). Among 64 patients, 26 (40.6%) and 15 (23.4%) showed a decrease of greater than 25% (mild improvement) and 35% (moderate improvement) in a Y-BOCS score, respectively.
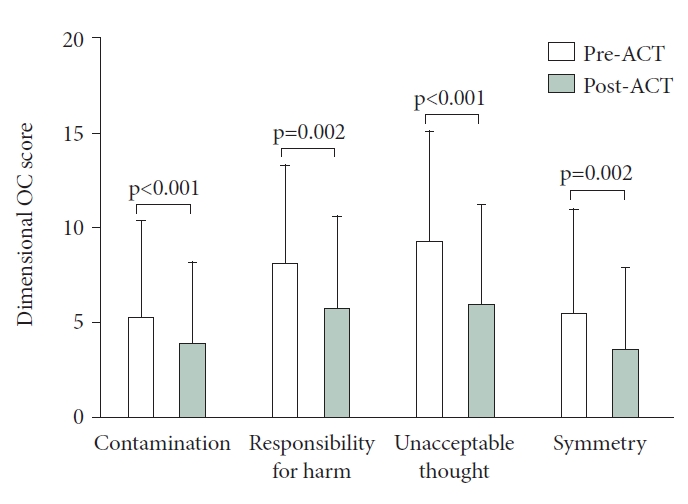
The paired t-test indicated that there were significant reductions in all four OC symptom dimensions (Figure 1). In terms of effect size, unacceptable thoughts (d=0.58) and contamination (d=0.53) domains had medium difference. Meanwhile, there was a small difference in responsibility for harm (d=0.41) and symmetry (d=0.40) dimension.
Relationship between OC symptom dimensions and ACT processes
Among the four symptom dimensions, the unacceptable thoughts dimension was significantly correlated with all ACT process measures, such as AAQ-OC (r=0.48, p<0.001), AAQII (r=0.38, p=0.008), and CFQ (r=0.38, p=0.008) (Table 3). The symmetry dimension was significantly correlated with AAQ-OC (r=0.37, p=0.010) and AAQ-II (r=0.30, p=0.042). The responsibility for harm dimension was correlated with AAQ-II alone (r=0.37, p=0.010). However, the contamination dimension was not associated with any process measures.
Regression analysis predicting individual OC symptom dimensions
Changes in the three scales of ACT processes significantly accounted for 27%, 17%, and 16% of the variance of changes in the DOCS unacceptable thoughts, responsibility for harm, and symmetry scores, respectively (Table 4). Regarding the contamination dimension, the three variables explained a very small and nonsignificant amount of variance.
DISCUSSION
This study aimed to investigate the differential effect of OCD symptom dimensions on the ACT outcome. Results showed significant reductions across all four OC symptom dimensions after ACT. The unacceptable thoughts and contamination domains had medium effect size, and the responsibility for harm and symmetry dimensions had small effect size. The unacceptable thoughts dimension showed significant correlations with all ACT process measures while the contamination dimension had no relationship. Then, three ACT variables accounted for a significant portion of variance in all dimensions except the contamination one.
In this study, ACT had the most notable effect on the unacceptable thoughts dimension. This dimension showed moderate symptom reduction, which was moderately correlated with and accounted for 27% of variance in changes in all three ACT process measures after treatment. These findings imply that ACT may effectively alleviate this symptom dimension. More importantly, this symptomatic improvement may be well explained by improvement in ACT processes. Notably, it is the only dimension related to the CFQ score. Therefore, dealing with fused thoughts (i.e., cognitive defusion) may be more helpful to this dimension than the rest since the unacceptable thoughts dimension, previously known as pure obsessional type, primarily comprises highly fused thoughts such as autogenous obsessions (i.e., forbidden thoughts), mental compulsions, and dysfunctional metacognitive beliefs (i.e., thought-action fusion).
Responsibility for harm and symmetry dimensions had similar effect size, correlation, and regression results in this study. That is, both dimensions had small effect size and were correlated with the AAQ-II score, but not with the CFQ score.
Nevertheless, improvement in the contamination dimension, although statistically significant, was the least in terms of mean score difference and was not supported by any ACT process measures. These findings corroborate with previous nonsignificant results on the correlation between this domain and AAQ-II score in cross-sectional studies [14,15]. Wetterneck et al. [15] speculated that experiential avoidance as measured by the AAQ-II may be more related to autogenous obsessions (i.e., thoughts of being responsible for harm to others) than to reactive obsessions (i.e., thoughts of contamination). Another possibility is that compulsive washing may be better related to questionnaires that measure lack of value or unworkable action, which were not used in this study. Therefore, future employment or development of ACT measures probing the effect of explicitly and highly ritualized behaviors (e.g., washing compulsion) is required [29].
Overall, these results may be contrasting to the differential effect of exposure and response prevention (ERP), the gold standard for OCD treatment, across symptom dimensions. Individuals with unacceptable thoughts have often been described as more resistant to ERP than those with other types of OCD. Thus, ERP for this group may be more challenging to implement given that compulsions are more likely to be primarily mental and reassurance-seeking behaviors that may be easily overlooked as rituals [30,31]. This difference between ACT and ERP is fundamentally attributed to the fact that ACT is a top-down approach, whereas ERP is a bottom-up approach.
This study had several limitations. First, due to the fact that the study had one sample design, the effect size was not controlled by any groups or interventions. Thus, we cannot say that this effect is clinically significant. However, our group using the same ACT program reported that the ACT intervention group was better than the waiting group [5]. Second, in addition to the self-report measure of the DOCS, most participants reported various symptoms across dimensions. Thus, it is challenging to ensure that our participants were representative of a specific dimension. Third, before we make any conclusion on the effect of ACT, post-treatment effect [5], which has been reported yet still remains controversial, should also be considered [8]. Fourth, during the treatment period, 6 patients newly started or increased the dose of antidepressants or anxiolytics, while 10 patients discontinued or decreased the dose. These changes may affect the treatment effect and further studies are needed to control the pharmacological effect with a large sample.
In conclusion, ACT may be effective against all four major symptom dimensions, and the unacceptable thoughts dimension may be better understood in terms of ACT process measures compared with the other dimensions.