INTRODUCTION
Cataracts are a major cause of visual impairment with an increasing global prevalence due to an aging society [1,2]. Decreases in visual acuity and vision loss in patients with cataracts lower the social and occupational functioning of individuals. Cataracts also cause insomnia-related symptoms, such shortened sleep duration and reduced sleep quality [3-6], which may lead to a deterioration in the patientsŌĆÖ quality of life [7-9].
Patients with cataracts often experience anxiety and depression associated with visual recovery before surgery, and these psychiatric symptoms could affect sleep [10,11]. Patients with cataracts experience diverse psychiatric symptoms according to individual factors [5,11,12]. Individual personality traits are risk factors for or protective factors against psychiatric symptoms, such as depression and anxiety.
Among the various models used to evaluate personality traits, the Big Five Model, consisting of emotional stability (ES), extraversion, agreeableness, conscientiousness, and openness to experience, is widely used [13], and various studies have been conducted to investigate the relationships among medical intervention methods and these personality domains [14]. Of these personality domains, low levels of ES may increase vulnerability to stress [15], and ES is significantly associated with preoperative anxiety and surgical outcomes [16,17]. Therefore, the ES level of patients with cataracts may be related to anxiety and insomnia.
Previous studies have mainly focused only on evaluating depression and anxiety in cataract patients, and studies examining the relationship between personality traits, such as ES, and anxiety and insomnia are lacking. The purpose of this study was to evaluate the effect of ES on preoperative anxiety and insomnia in patients who were scheduled to undergo cataract surgery.
METHODS
The subjects were scheduled to undergo an operation for cataracts. Self-questionnaires evaluating sociodemographic characteristics, the level of insomnia, depressive and anxious mood, and the ES personality trait were administered to all subjects before the cataract surgery. The total number of subjects was 54. The completed questionnaires were collected by the investigators before the surgery. This study was approved by the Institutional Review Board (approval No. 2015-01-011-003). Informed consent was provided by all subjects when they enrolled.
The subjectsŌĆÖ level of insomnia was evaluated using the Insomnia Severity Index (ISI). The ISI consists of 7 items, including satisfaction with sleep, functional impairment in daily life due to insomnia, and recognition of problematic sleep. Higher total scores represent more severe insomnia [18]. The validity of the Korean version of the ISI was confirmed (CronbachŌĆÖs ╬▒=0.86) [19].
ES was investigated using the International Personality Item Pool (IPIP). The IPIP was developed to evaluate individualsŌĆÖ personality traits, and 10 questions on the IPIP assess ES [13]. A study using the Korean version of the IPIP showed that this measure has sufficient validity (CronbachŌĆÖs ╬▒=0.86) [20].
The Hospital Anxiety and Depression scale (HADS) was used to assess anxious and depressive mood symptoms. The HADS was developed to assess subjects visiting a hospital. The measure includes two subdomains, i.e., anxiety (HADS-A) and depression (HADS-D), and each subdomain consists of 7 items; in total, the HADS consists of 14 questions. Higher total scores on each subdomain indicate more severe symptoms of anxiety or depression [21]. The internal validity of the Korean version of the HADS was confirmed, with CronbachŌĆÖs ╬▒=0.89 [22].
The subjects were divided into the following three groups according to their ES scores using a method suggested in a previous study involving a Korean population: low ES (1 SD below the mean), average ES (within┬▒1 SD), and high ES (1 SD above the mean) [20]. The Kruskal-Wallis test was performed to compare the scores on the ISI, HADS-A, and HADS-D among the three groups, and a Games-Howell post hoc analysis was performed to analyze the variables that did not show homogeneity. The Pearson analysis was performed to analyze the correlation of ES with the HADS-D score and the HADS total score. In addition, Spearman correlation analysis was performed to analyze the correlation of ES with the scores on the HADS-A and the ISI, the distributions for which did not show normality. A multiple linear regression analysis was performed to analyze the association between the ISI total score as the dependent variable and the ES score, the HADS-A score, and the HADS-D score as the independent variables, after adjusting for age, sex, and caffeine consumption as covariates. A pathway analysis was performed to analyze the indirect and mediating effects of the ES, HADS-A, and ISI scores. The model fit was evaluated by calculating the SRMR, NFI, IFI, and CFI. All statistical analyses were conducted using SPSS version 21.0 (IBM Corp., Armonk, NY, USA) and AMOS 18.0 (SPSS Inc., Chicago, IL, USA), and two-tailed p-values<0.05 were considered to indicate statistical significance.
RESULTS
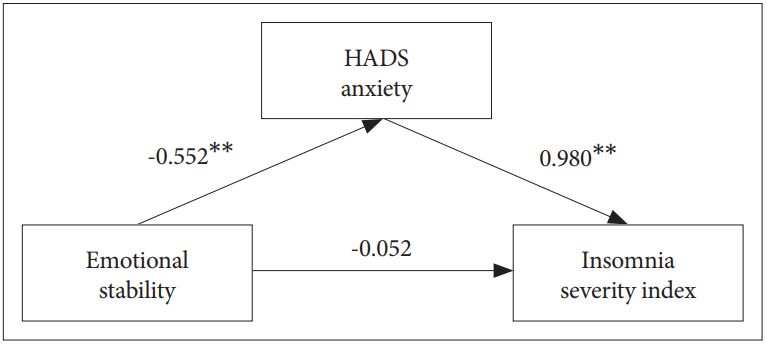
The mean age of the subjects was 63.6┬▒10.7 (mean┬▒SD) years, and males comprised 55.6% of the sample. The mean scores of the subjects on the ISI, ES, HADS-D, and HADS-A were as follows: 7.6┬▒7.6, 29.0┬▒6.0, 5.5┬▒4.9, and 7.8┬▒4.4. After dividing the subjects into three groups according to their ES score, the degree of insomnia was compared among the groups, and the low-ES group showed significantly higher insomnia severity than the high-ES group (12.7┬▒10.2 vs. 5.1┬▒5.7, p=0.048). The means of the HADS total and subscale scores significantly differed among the ES groups (Table 1). In the results of the correlation analyses, the ES score was significantly correlated with the HADS total score, the HADS-A score, the HADS-D score, and the ISI score, the r-values (p-value) for which were -0.810 (p<0.001), -0.693 (p<0.001), -0.739 (p<0.001), and -0.326 (p=0.016), respectively. According to the multiple linear regression analysis, the standardized regression coefficient (╬▓) between the ES and ISI scores was -0.099 (p=0.609), and the ╬▓ between the ES and HADS-A scores was 0.697 (p=0.001). No statistically significant association was observed between the HADS-D and ISI scores (╬▓=-0.149, p=0.421). The effect size (CohenŌĆÖs f2) for the multiple linear regression analysis was 0.828. According to the pathway analysis (Figure 1), ES had a statistically significant indirect effect (-0.541) on the ISI scores through the HADS-A scores (p=0.009, bootstrap 200; 95% confidence intervals), and the model fit was appropriate (SRMR=0.000, NFI=1.000, IFI=1.000, CFI=1.000).
DISCUSSION
In this study, we found that lower levels of ES could contribute to more severe insomnia symptoms in cataract patients before surgery. Furthermore, we revealed that anxiety had a mediating effect on the negative relationship between ES and insomnia. In a community-based study of elderly cataract patients, visual impairment was closely related to insomnia, and more than half of the patients reported sleep induction impairment and sleep maintenance difficulties [6]. Patients with cataracts easily experience anxiety and depression due to the discomfort of daily life caused by a deterioration in visual function before surgery and the negative expectations of poor postoperative outcomes [10,13]. Additionally, preoperative anxiety symptoms may trigger the activation of the sympathetic nervous system [23] and result in an abnormal arousal state, which can adversely influence the maintenance of sleep in patients [24]. Compared with emotionally disturbed individuals, people with high levels of ES are not only more tolerant of uncertain situations but are also more likely to maintain stability and practice self-control in stressful situations [13,20]. The mediating effect of anxiety symptoms on the negative relationship between ES and insomnia, which is the main outcome of this study, could be explained by the protective role played by high levels of ES in preoperative anxiety.
From a neurobiological perspective, high levels of ES are positively related to the circadian rhythm, which is responsible for favorable night sleep quality [25]. Patients with cataracts have decreased light input through the eyes due to visual impairment. This decreased light input has a negative effect on the suprachiasmatic nucleus (SCN) in the hypothalamus, which regulates the sleep cycle, thus causing insomnia [6]. However, individuals with high ES maintain better serotonergic function than those with low ES. The maintenance of these serotonergic functions could stabilize the change in the circadian rhythm due to the impairment in SCN function by the light input reduction and may be protective against insomnia in cataract patients [25,26]. This hypothesis may be a neurobiological explanation of the negative association between ES and insomnia in the present study.
This study has several limitations. First, assessing objective insomnia-related symptoms was challenging due to the use of self-report questionnaires. Therefore, evaluating the patientsŌĆÖ sleep state more precisely using laboratory tools, such as polysomnography or actigraphy, is necessary. Second, because the total number of participants in this study was relatively small, the generalizability of the results to the entire population is limited. However, since the effect size (0.828) of the outcomes was large, the significance of the results appears to be sufficient.
Despite these limitations, this study is the first to reveal that ES, which is a personality trait, may be associated with preoperative insomnia in cataract patients. Previous studies investigating psychiatric symptoms in cataract patients have been limited to anxiety and depression and did not evaluate personality traits [5,11,12]. Anxiety symptoms in patients with cataracts decrease the psychological and physical quality of life [8] and adversely affect the course and prognosis of the disease [27]. Screening for factors associated with anxiety, such as ES, in cataract patients could be important. In this study, we revealed a negative relationship between ES and preoperative anxiety. Thus, if the ES level of the patient is assessed before surgery and psychological stability is facilitated using appropriate interventions for patients with low ES, then surgical outcomes and quality of life are expected to improve.