Leptin, Nesfatin-1, Orexin-A, and Total Ghrelin Levels in Drug-Naive Panic Disorder
Article information

Abstract
Objective
This study aimed to examine the changes in serum nesfatin-1, leptin, orexin-A, and total ghrelin levels of patients diagnosed with drug-naive panic disorder (PD) before and after six weeks of the treatment and to compare the findings with the healthy subjects.
Methods
The neuropeptides were measured in venous blood samples taken from 32 patients and 32 healthy subjects. The blood samples of the patients who used paroxetine 20 mg/day plus alprazolam 0.5 mg/day were retaken again after six weeks. Measurements were performed with the Enzyme-Linked Immunosorbent Assay (ELISA) method.
Results
Serum nesfatin-1, leptin, orexin-A and total ghrelin levels of the patient group were found to be significantly lower than the control group (p<0.001, p<0.001, p<0.001, and p<0.001, respectively). When the serum nesfatin-1, leptin, orexin-A and total ghrelin levels of the patient group were compared before and after treatment, significant differences were found in terms of orexin-A and total ghrelin levels (p=0.046, p<0.001, respectively). However, no significant differences were found in terms of nesfatin-1and leptin levels (p=0.205, p=0.988, respectively).
Conclusion
This study reports that PD, like other anxiety disorders, may affect serum nesfatin-1, leptin, orexin-A, and total ghrelin levels, and there may be a relationship between PD treatment and the levels of these neuropeptides. The variability of this relationship among the neuropeptides examined indicates that various factors other than treatment play a role in this process.
INTRODUCTION
Sociodemographic characteristics, childhood experiences, attachment styles, physical diseases, genetics, and many other factors have been investigated in the etiology of panic disorder (PD), a common psychiatric disorder characterized by recurrent and unexpected panic attacks. However, the etiology of PD, in which psychiatric symptoms and physical symptoms are seen together, has not yet been clarified. In recent years, the number of studies on genetics, panic models, provocation, respiration and hyperventilation, neuroimaging, and psychotrophic drugs has been increasing to elucidate the etiology of PD [1-3]. Another area of interest to researchers is the possible roles of metabolic hormones in PD. A limited number of studies investigate the relationship of between neuropeptide hormones with PD [4,5].
Neuropeptides are proteins that enable neurons to communicate with each other in the brain and nervous system, and thus perform many physiological regulation and behavior in metabolism [6]. The neuropeptides such as leptin, ghrelin, and nesfatin-1 are associated with the pathophysiology of PD [4,7,8]. Inconsistent study findings in the relevant literature show that this relationship has not been revealed yet. Most studies were conducted in PD patients with a history of treatment. Very few studies have examined the effect of PD treatment on neuropeptide hormones. No study has been found in the literature examining the change in serum nesfatin-1, leptin, orexin-A, and total ghrelin levels in drug-naive PD patients with the administration of paroxetine plus alprazolam.
This study aimed to compare the serum nesfatin-1, leptin, orexin-A, and total ghrelin levels of drug-naive PD patients before and after paroxetine plus alprazolam treatment with healthy subjects.
METHODS
Participants
The participants of this study consisted of consecutive outpatients diagnosed with PD who applied to Firat University Faculty of Medicine psychiatry outpatient clinic between January 1, 2022–June 30, 2022. One hundred and eighty-seven patients with a diagnosis of PD were evaluated for inclusion in this study. Among the PD patients who applied to the outpatient clinic, 32 patients who had not used any psychotropic drugs before, did not accompany organicity, did not have alcohol and substance comorbidity, were not found to have neurocognitive impairment, and whose sociocultural level did not prevent adaptation to the study were included in the study. Ninety-two patients who used psychotropic drugs had a psychiatric history or had an additional psychiatric disorder, 24 had an additional medical disease and/or used additional medical drugs, and 39 patients who prevented adaptation to the sociocultural study and other reasons were excluded from the study. Two psychiatry specialists with at least five years of experince diagnosed PD according to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) [9] and managed the treatment process. All of the scales were administered by the first author who was trained in psychometric scales. The healthy control group was selected from patients who did not have any psychiatric or organic disease, did not use drugs, did not have alcohol and substance comorbidities, and did not have neurocognitive impairment. Age and sex distributions of the patient group were taken into consideration when choosing the healthy control group. Disease and drug histories of the healthy control and patient groups were checked with their consent from the national patient registry system, e-nabız. This study was approved by Firat University Faculty of Medicine Non-Interventional Research Ethics Committee (Number: 2021/05-39). In addition, the study was funded by the Scientific Research Project Coordination Unit of Firat University (Project Number: TF.21.44).
Instruments
Sociodemographic and clinic data form
The sociodemographic data form was developed by the researchers in order to determine the sociodemographic characteristics of the subjects participating in the study. In this form, information about the patient’s name-surname, age, sex, application date, height, weight, contact number, education level, marital status, occupation, employment status, place of residence, smoking status, psychiatric or organic disease history in themselves and their families and medication history was questioned. In addition, in the patient group, questions related to panic attacks, which medical branches they applied to before psychiatric admission, and whether they had an emergency application were determined.
DSM-5 Panic Disorder Scale (PDS)
The PDS is a 10-item self-assessment scale developed by the American Psychiatric Association and provides a 5-point Likert-type rating (0=never; 1=sometimes; 2=half of the time; 3=most of the time, 4=all of the time). When completing the scale, participants consider how much PD has affected their private lives in the last seven days. The scores obtained from the scale items determine the severity of PD. The score that can be obtained from the scale is between 0–40, and high scores indicate that PD is severe. The Turkish validity and reliability study was performed by Balıkçı et al. [10] It assesses the severity of PD in individuals aged eighteen and older. The raw scores of the ten items must be added together to obtain a total raw score. In addition, the clinician is asked to calculate the average total score. The average total score is calculated by dividing the total raw score by the number of items in the scale. In DSM-5 field studies, it is stated that the average total score is reliable, easy to use, and useful for clinicians. The average total score transforms the overall score into a 5-point scale and enables the individual to evaluate the severity of PD as absent (0), mild (1), moderate (2), severe (3) and extreme (4). The average total score was used in this study.
Procedure
The general characteristics of the study and the process were explained in detail to the patients and healthy controls included in the study, and informed consent was obtained. The patients were started on paroxetine 20 mg/day plus alprazolam 0.5 mg/day therapy. In addition to medical treatment, all patients were informed about PD with a guide. The psychiatric interview was carried out in the following order and content in general terms: What is PD and panic attack? Why does PD occur? What are the symptoms of PD? How is the physiology of PD and its relationship with the sympathetic system? How does the first panic attack begin? What is the mechanism of fear of death, heart attack, paralysis and going crazy? What is anticipatory anxiety? How is the progress in PD? Is PD treatment possible? What are the effects and side effects of drug therapy? What is cognitive behavioral therapy and how is it applied in PD? What is muscle relaxation and breathing exercise? How should it be applied in panic attacks?
Psychiatric interview, application of the study and initiation of treatment were determined as 45±5 minutes for each patient. At the end of 6 weeks, the patients were called for reassessment/second interview. Control dates were reminded to them before the control via their contact phone numbers, and all the patients who were treated in this way were allowed to come for the control. Sociodemographic and clinical data forms were filled in for patients and healthy controls. Psychometric scale was administered to the patient group at the beginning and end of the six weeks of the treatment, and once to the healthy control group.
All cases included in the study were referred to medical biochemistry laboratory. Five milliliters of venous blood samples were taken by a registered nurse from the healthy control and patient groups within the scope of the study and placed in tubes with aprotonin. After the blood samples were centrifuged at 3,000–4,000 rpm for 5–10 minutes, their serum and plasma were separated; taken into capped tubes and numbered; it was stored at -80°C until analysis. All blood samples were taken between 08:00–09:00 am when the subjects were fasting in the morning. Blood samples were taken again by a registered nurse for biochemical measurements from patients who were emphasized to use drug treatments regularly and were called for reassessment/second interview after 6 weeks. Blood sample was drawn from healthy control subjects only at the beginning of the study.
Biochemical analysis
Nesfatin-1, leptin, total ghrelin, orexin-A levels were measured with commercial Enzyme-Linked ImmunoSorbent Assay (ELISA) kits using ELx50 (BioTek ELx50 Microplate Washer; Agilent Technologies INC., Santa Clara, CA, USA) and EPOCH 2 (Agilent BioTek Epoch 2; Agilent Technologies INC., Santa Clara, CA, USA) microplate reader based on ELISA method.
The features of ELISA kits are as follows:
Nesfatin-1: Human NES1 Elisa Kit (Shanghai Sunred Biological Technology Co., Ltd, Baoshan, China), Cat No: 201-12-4341, Assay Range: 0.2 mmol/L-35 mmol/L, Senstivity: 0.113 mmol/L, Intra-assay: CV<10%, Inter-assay: CV<12%;
Leptin: Human LEP Elisa Kit (Shanghai Sunred Biological Technology Co., Ltd, Baoshan, China), Cat No: 201-12-1560, Assay Range: 0.2 ng/mL–60 ng/mL, Senstivity: 0.153 ng/mL;
Orexin-A: Human Orexin A Elisa Kit (Shanghai Sunred Biological Technology Co., Ltd, Baoshan, China), Cat No: 201-12-1297, Assay Range: 7 ng/L-2,000 ng/L, Senstivity: 5.125 ng/L;
Total Ghrelin: Human Ghrelin Elisa Kit (Shanghai Sunred Biological Technology Co., Ltd, Baoshan, China), Cat No: 201-12-5583, Assay Range: 30 pg/mL–9,000 pg/mL, Senstivity: 28,225 pg/mL.
Statistical analysis
Analyzes were evaluated in the IBM SPSS 22.0 (Statistical Package for Social Sciences; IBM Corp., Armonk, NY, USA) package program. The study shows descriptive data as n, % values in categorical data and standard deviation in continuous data. The chi-square test was used to compare categorical variables between groups. The conformity of continuous variables to normal distribution was evaluated by Kolmogorov–Smirnov test. Diagnosis of PD and the effect of PD treatment were accepted as independent variables, and sociodemographic, clinical, and biochemical parameters were accepted as dependent variables. Student’s t-test was used for normally distributed variables, and the Mann–Whitney U test was used for non-normally distributed variables to compare pairwise groups. The dependent sample t-test was used for normally distributed variables, and the Wilcoxon Signed Ranks test was used for non-normally distributed variables to compare dependent variables. Cohen’s d and Glass’s delta were calculated for the effect size. Cohen’s d values were used when the standard deviations were similar, and Glass’s delta values were used when the standard deviations were not. The Pearson correlation test was used for those with normal distribution, and the Spearman correlation test was used for those who did not show normal distribution in examining the relationship between continuous variables. The statistical significance level in the analysis was accepted as p<0.05.
RESULTS
Sociodemographic characteristics of the subjects
The patient and control groups consisted of 32 subjects (13 female, 19 male). There was no statistically significant difference between the groups in terms of age (p=0.835), education level (p=0.064), marital status (p=0.458), income status (p=0.232), smoking status (p=0.133), and body mass index (BMI) (p=0.580) (Table 1).

Sociodemographic and clinical characteristics of the patient and control groups
The patients had experienced their first panic attack 23.65±16.11 days ago. In the patient group, 19 (59.4%) subjects had a history of admitting to the emergency department due to a panic attack; 15 (46.9%) subjects to cardiology; 18 (56.3%) subjects to internal medicine; 2 (6.3%) subjects to neurology and 1 (3.1%) subject to chest diseases. Nineteen (59.4%) of the patients were referred to psychiatry by non-psychiatric physicians. While 7 (21.9%) patients applied directly to psychiatry of their own free will, 6 (18.8%) patients were referred to psychiatry by their relatives or friends.
Serum nesfatin-1, leptin, orexin-A and total ghrelin values of the patient group before treatment were compared with the control group (Table 2). Accordingly, a statistically significant difference was found between the patient group and the control group in terms of serum nesfatin-1, leptin, orexin-A and total ghrelin levels before treatment (p<0.001).

Comparison of serum nesfatin-1, leptin, orexin-A and total ghrelin levels of the patient group before treatment and control group
Serum nesfatin-1, leptin, orexin-A and total ghrelin values of the patient group after treatment were compared with the control group (Table 3). Accordingly, a statistically significant difference was found between the patient group and the control group in terms of serum nesfatin-1, leptin, orexin-A and total ghrelin levels after treatment (p<0.001).

Comparison of serum nesfatin-1, leptin, orexin-A and total ghrelin levels of the patient group after treatment and control group
Serum nesfatin-1, leptin, orexin-A and total ghrelin values of the patient group before and after treatment were compared (Table 4). Accordingly, there was no statistically significant difference in serum nesfatin-1 (p=0.205) and leptin (p=0.988) levels before and after treatment, while there was statistically significant difference in orexin-A (p=0.046) and total ghrelin (p<0.001) levels. The PDS score of the patient group before treatment was 28.87±7.99, while the post-treatment score was 13.15±8.62 (p<0.001).
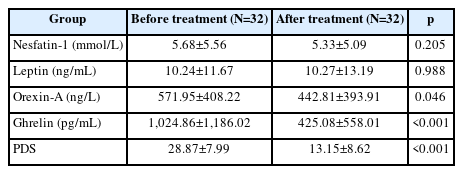
Comparison of serum Nesfatin-1, Leptin, Orexin-A and total ghrelin levels of the patient group before and after treatment
DISCUSSION
The relationship between psychiatric disorders and neurotransmitter systems has been known for many years. Recent studies have shown that neuropeptides may also be more associated with psychiatric disorders than previously thought. The various physiological and pathological mechanisms in which they play a role have been the most important reason for thinking in this way [11]. In this study, drug-naive PD and control groups with similar sociodemographic characteristics were compared in terms of serum nesfatin-1, leptin, orexin-A and total ghrelin levels. The fact that the sociodemographic variables of the patient and control groups were similar facilitated the interpretation of the findings. Serum nesfatin-1, leptin, orexin-A and total ghrelin levels of the patient group were significantly different from the healthy control group both before and after the treatment. When the serum nesfatin-1, leptin, orexin-A and total ghrelin levels of the patient group were compared before and after the treatment, significant differences were found in terms of orexin-A and total ghrelin levels, but no significant difference was found in terms of leptin and nesfatin-1 levels.
In addition to its effects on hunger and satiety, the relationship of nesfatin-1 with stress has been investigated in various studies. By activating the hypothalamic-pituitary-adrenal axis, nesfatin-1 activates serotonin in the nucleus raphe and norepinephrine in the locus cereleus. The nucleus raphe and locus cereleus are key centers of the serotonergic and noradrenergic brain signaling system. Their inability to function adequately is closely related to psychiatric disorders [8]. Könczöl et al. [12] reported that the level of stress-related hormones increased with intravenous nesfatin-1 administration. Bez et al. [8] compared nesfatin-1 levels between PD patients and healthy control groups, and the mean plasma nesfatin-1 level of PD patients was found to be higher than the control group. In addition, in this study, a positive correlation was found between plasma nesfatin-1 levels and panic disorder severity scores of patients with PD. In the study of Bez et al. [13] in which they compared nesfatin-1 levels between obsessive-compulsive disorder patients and healthy control groups, the mean plasma nesfatin-1 level of obsessive-compulsive disorder patients was found to be higher than the control group.
On the other hand, there are also studies reporting that the level of nesfatin-1 decreases in stress-related situations. In the study performed by Gunay et al. [14] on male patients with a diagnosis of generalized anxiety disorder, decreased nesfatin-1 levels were found in the patient group compared to the healthy control group. In the study of Hofmann et al. [15], no significant change was found in the nesfatin-1 levels of obese female patients treated for anxiety. According to the findings of our study, nesfatin-1 levels were found to be significantly lower in both female and male patients compared to healthy controls, both before and after treatment. In addition, similar to the study of Hofmann et al. [15], in our study, it was observed that treatment did not significantly affect nesfatin-1 levels in this study.
The possible reasons why nesfatin-1 levels were found to be lower in the patient group compared to the healthy control group have also been the subject of discussion in studies that reached similar findings in the past. It has been stated that one of the possible reasons for this may be the fasting-satiety status of the patients and the duration of fasting. Kohno et al. [16] reported that nesfatin-1 neurons in both hypothalamic paraventricular and supraoptic nuclei were not activated after two days of fasting, but became active after refeeding. Studies have shown that plasma nesfatin-1 levels in rats are significantly reduced after twenty-four hours of fasting and return to baseline after refeeding [17]. In our study, the blood of the subjects was taken during fasting and in the early morning hours at every stage of the study. However, the fasting-satiety status and duration of the patients in the patient or control group were not determined precisely, their verbal statements were taken as basis. It is possible that changes in appetite accompany the diagnosis of PD and that this situation may affect nesfatin-1. In addition, the effect of stress on nesfatin-1 is not known exactly. The reason for the anxiety or panic attacks of our patients may be due to a situation unrelated to nesfatin or metabolism. In this case, how a stress occurring in the body affects the level of nesfatin-1 is a subject that needs to be investigated.
The number of studies investigating the effects of leptin on mood and affect is increasing. Animal studies of anxiety have reported possible anxiolytic effects of leptin in anxiety disorders. Asakawa et al. [18] found a decrease in anxiety levels in addition to obesity in mice receiving leptin treatment. Human studies have also shown the relationship between anxiety and leptin levels. Yoshida-Komiya et al. [19] reported that leptin levels were lower and anxiety scores were higher in women of reproductive age with mild anxiety compared to healthy controls. On the other hand, in some studies, no significant difference was found between anxiety patients and healthy controls, or anxiety was found to be high in case of stress. Masdrakis et al. [4] suggested that serum leptin levels are associated with the severity of psychopathology including anxiety, phobic anxiety and panic attacks in PD patients. However, in the same study, no significant difference was found between the leptin levels of PD patients and healthy controls [15]. Ozmen et al. [20] found that leptin levels in girls with anxiety were similar to healthy controls. Atmaca et al. [21] found no difference in leptin levels between pure obsessive-compulsive disorder patients and the control group. Otsuka et al. [22] showed that male subjects with a high perception of psychological stress had high leptin levels. In our study, the leptin levels of the pre-treatment patient group were found to be lower than the healthy controls, which is consistent with the vast majority of information in the literature. This significant difference between the patient and control groups continued after six weeks of treatment. However, according to this study, the treatment did not have a significant effect on the leptin levels of the patient group. Although the findings of this study are consistent with the majority of the literature, there are also studies reporting the opposite. These differences in the literature are thought to be due to the methodologies or limitations of the studies.
Recent evidence suggests that orexins are involved in the elicitation of both behavioral and neuroendocrine responses to conditions that activate the hypothalamic-pituitary-adrenal axis, and that dysregulation of the orexin system may lead to pathological stress-related conditions [23-25]. Studies investigating the relationship of orexins with anxiety and stress in humans are limited. Just as with leptin and nesfatin-1, it is seen that there are various differences between the findings of the studies in the literature related to orexin-A. Johnson et al. [26] investigated the levels of orexin-A in the cerebrospinal fluid of patients presenting with acute suicidal behaviors. These patients were divided into three groups: patients with panic anxiety without major depressive disorder, patients with panic anxiety and major depressive disorder together, and patients without panic anxiety or major depressive disorder. Johnson et al. [26] found that only patients with panic anxiety had the highest levels of orexin-A. Akça et al. [27] reported that orexin-A level was positively and significantly correlated with anxiety in a study in which they compared adolescents who do not use drugs and have any anxiety spectrum disorder and healthy controls. In addition, it was reported that orexin-A levels were higher in the patient group. Strawn et al. [28] found lower cerebrospinal fluid and plasma orexin-A concentrations in patients with post-traumatic stress disorder compared to healthy controls. It also reported a negative correlation between cerebrospinal fluid orexin-A concentrations and the severity of post-traumatic stress disorder. Ozsoy et al. [29] compared the orexin and cortisol levels of female patients with depression and/or anxiety symptoms and healthy controls and did not report a significant difference between the groups. The findings of studies investigating the anxiety-reducing effects of orexin antagonists are also contradictory. These conflicting reports on the use of orexin antagonists as anxiolytic agents suggest that the issue needs to be clarified in future studies. In our study, the orexin-A levels of the pre-treatment patient group were found to be lower than the healthy controls. This significant difference between the patient and control groups continued after six weeks of treatment. In addition, according to our study, it was observed that the treatment significantly reduced the orexin-A levels of the patient group. It was thought that the agents used in the treatment may have a role in this alteration. As a matter of fact, alprazolam, an anxiolytic agent, was used in this study. As can be seen from the literature, it is thought that the contradictory findings of orexin-related studies are due to the methodologies or limitations of the studies.
With the emergence of the effects of ghrelin in the central nervous system, the number of studies aimed at elucidating its role in psychiatric disorders has gradually increased. In our study, it was determined that total ghrelin levels were significantly lower in the patient group both before and after the treatment compared to the healthy controls. After six weeks of treatment, it was observed that the total ghrelin levels decreased remarkably. When the literature is examined, it is seen that there are different findings regarding the relationship between anxiety and ghrelin levels.
Both animal and human studies suggest that ghrelin is involved in the regulation of the stress response. Available data show an increase in serum ghrelin after exposure to psychological stress in both rodents [30] and humans [31], although there are studies that did not detect any increase [32]. In parallel, the serum ghrelin levels of women reporting many interpersonal stressors were found to be higher than those reporting few interpersonal stressors [33]. The precise role of ghrelin in anxiety is fiercely debated. There is no consensus on whether ghrelin alleviates anxiety [34]. The most important research supporting the anxiolytic effects of ghrelin is the study of Lutter et al. [35] Lutter et al. [35] concluded that ghrelin reduces anxiety-like behaviors that occur during times of high stress. Anxiolytic effects were also observed in another study after ghrelin infusion into the amygdala. Interestingly, feeding abolished these anxiolytic effects between the ghrelin infusion and the anxiety test [36]. There are also animal and human studies suggesting that ghrelin is associated with increased anxiety-like behavior and increased fear memory after chronic stress [37]. However, a trend towards deterioration in fear memory was observed after acute stress in these studies, suggesting an anxiolytic effect [34]. Thus, ghrelin may exert anxiolytic effects in acute stress, while promoting anxiogenic behavior in non-stressful and chronically stressful conditions. The assumption that ghrelin exerts a dual effect, both anxiogenic and anxiolytic depending on the circumstances, may reconcile some, if not all, of the conflicting findings [34,38]. Studies suggesting that ghrelin has an anxiolytic effect include peripheral ghrelin administration [35], while studies suggesting an anxiogenic effect include central ghrelin administration [39]. This may be one of the reasons for the different findings in animal studies. There is also some evidence that ghrelin exerts different effects depending on the site of administration in the central nervous system [40]. The majority of animal studies have examined the effects of external ghrelin administration on animals. However, in our study, there is no external application of ghrelin. Still, this information from animal studies can make it easier to understand the situation in humans.
Human studies investigating the potential role of ghrelin in anxiety disorders are relatively limited. In one study, higher ghrelin serum levels were reported in patients with PD who did not respond to treatment compared to responders and healthy controls [5]. Emül et al. [41] compared the ghrelin plasma levels of obsessive-compulsive disorder patients, patients with obsessive-compulsive disorder and major depressive disorder together, and healthy controls, and found no difference between the groups. Ozmen et al. [20] found that ghrelin levels were higher in children with anxiety disorder compared to healthy controls. Gul et al. [7] found that patients with PD had significantly higher ghrelin levels before treatment with paroxetine 20 mg/day compared to healthy controls. It has been reported that ghrelin levels decreased significantly after paroxetine treatment. Wittekind et al. [42] applied an anxiety disorder scale to the subjects in their study conducted in the general population and found a non-significant positive correlation between ghrelin levels and anxiety scale scores. A significant positive correlation was found in cases whose anxiety level was evaluated as mild or less. On the other hand, it has been reported that there is a negative correlation in subjects with anxiety symptoms above the cut-off value of the anxiety scale score. According to the study of Wittekind et al. [42], the positive relationship between ghrelin and mild anxiety is the first indicator of the role of ghrelin in the regulation of physiological anxiety in humans. This relationship and the opposite relationship in pathological anxiety are similar to the findings in animals showing different ghrelin effects in acute and chronic stress conditions. When the findings of animal and human studies related to ghrelin are evaluated together with the findings of this study, it is seen that the discussions on this subject will continue for a while. It should not be overlooked that patients with PD were recruited in our study and that the symptoms of these patients started recently and acutely (approximately 20 days). As seen in the study of Wittekind et al. [42], it is possible that the effect of acute and chronic stress on ghrelin levels is different. Although our healthy control group does not have a clinical psychiatric disorder, the level of their physiological anxiety is unknown. The significant decrease in ghrelin levels in the patient group after paroxetine treatment is a finding similar to the study of Gul et al [7].
This study has several limitations. The control group of this study consisted of healthcare workers. It is known that the health system in Turkey is challenging for healthcare workers [43]. The coronavirus disease-2019 pandemic has further increased these difficulties unique to Turkey and has caused a widespread increase in stress and anxiety even though it has not reached the level of psychiatric disorder in healthcare workers [44]. In this sense, it should not be forgotten that our healthy control group may have possible anxiety states. In future studies, it may be considered as an option to recruit people from outside the health sector as a healthy control group. Although the inclusion and exclusion criteria of patients and controls have been carefully considered, it should not be overlooked that there may be possible errors due to inaccuracy of verbal statements, incorrect recall and individual forgetting factor. The fact that a structured clinical interview was not applied to the patient and control groups makes it difficult to exclude psychiatric comorbidities. It was thought that the possibility that the subject’s statements about hunger and fullness status or duration were incorrect may have affected the results. Sleep patterns and physical activity levels were not questioned in either the patient or control group. The treatment duration in this study was relatively short. There is a need to increase the sample size. It is possible that the ELISA kits used affected the results differently. Measuring acyl and desacyl ghrelin levels separately in addition to total ghrelin will provide a more detailed interpretation of ghrelin findings. Since there are not enough studies examining the neuropeptide levels mentioned in drug-naive PD, interpreting it based on non-PD anxiety spectrum disorders is another limitation.
In conclusion, this study reports that serum nesfatin-1, leptin, orexin-A and total ghrelin levels are lower in drug-naive PD patients compared to the healthy control group. Six weeks of treatment decreased orexin-A and total ghrelin levels, but did not affect leptin and nesfatin-1 levels. Neuropeptide levels have the potential to be affected by many different factors such as fasting-satiety status, drugs, kits, acute-chronic stress and pathological-physiological anxiety. It is recommended to pay attention to these conditions that may cause limitations in future studies.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Dilek Örüm, Sevda Korkmaz. Data curation: Dilek Örüm, Mehmet Hamdi Örüm. Formal analysis: Dilek Örüm, Mehmet Hamdi Örüm, Sevda Korkmaz, Nevin İlhan. Funding acquisition: Sevda Korkmaz, Dilek Örüm. Investigation: all authors. Methodology: Dilek Örüm, Mehmet Hamdi Örüm, Sevda Korkmaz, Nevin İlhan. Project administration: Sevda Korkmaz, Dilek Örüm. Resources: Dilek Örüm, Mehmet Hamdi Örüm, Sevda Korkmaz, Nevin İlhan. Software: Dilek Örüm, Mehmet Hamdi Örüm. Supervision: Murad Atmaca, Sevda Korkmaz, Nevin İlhan. Validation: Murad Atmaca, Sevda Korkmaz, Nevin İlhan. Visualization: Dilek Örüm, Mehmet Hamdi Örüm. Writing—original draft: Dilek Örüm, Mehmet Hamdi Örüm. Writing—review & editing: Dilek Örüm, Mehmet Hamdi Örüm, Murad Atmaca.
Funding Statement
Firat University Scientific Research Projects (FÜBAP) Coordination Unit (Project Number: TF.21.44).