Diabetic Ketoacidosis Associated With Second Generation Antipsychotics: A Case Study and Review of Literature
Article information

Abstract
Objective
Second-generation antipsychotics (SGAs) have revolutionized the treatment of psychiatric disorders, but are associated with significant metabolic risks, including diabetes and hyperglycemic crises. This review explores the complex interplay between antipsychotics, diabetes, and hyperglycemic crises, highlighting the mechanisms underlying SGA-induced diabetes.
Methods
We present the case of a patient with schizophrenia who was taking antipsychotic medication and was admitted to the emergency room due to the sudden onset of diabetic ketoacidosis (DKA) without any history of diabetes. We extensively searched databases, including Elsevier, PubMed, IEEE, SpringerLink, and Google Scholar, for papers on the effects of antipsychotic drugs on DKA from 2002 to 2021. We focused on DKA, hyperglycemia, and atypical antipsychotics, and retrieved 117 papers. After full-text review, 32 papers were included in this comprehensive review.
Results
DKA was significantly more frequent in patients taking SGAs. Antipsychotics can induce insulin resistance either directly or through the onset of obesity. Antipsychotics can reduce insulin secretion from pancreatic β-cells, which is associated with absolute insulin deficiency.
Conclusion
As the use of antipsychotics continues to increase, understanding their risks and mechanisms is crucial for clinicians to enable informed treatment decisions and prevent potentially life-threatening complications.
INTRODUCTION
Antipsychotic drugs are commonly used to treat various psychiatric disorders, including schizophrenia, bipolar disorder, major depression, and the behavioral and psychological symptoms of dementia [1]. First-generation antipsychotics have been prescribed since the 1950s, and exert their therapeutic effects by blocking dopamine D2 receptors. The associated adverse effects include extrapyramidal symptoms, akathisia, and tardive dyskinesia [2]. To reduce these neurological adverse effects, second-generation antipsychotics (SGAs) were developed, and have been approved by the FDA since the 1990s [3]. SGAs target multiple neuroreceptors such as the serotoninergic 5-HT2A/5-HT2C, histaminergic H1, and muscarinic M3 receptors, apart from the D2 receptors. These drugs are now widely used as first-line antipsychotics due to the lower risk of side effects and are more successful in terms of long-term treatment and tolerability compared to first-generation antipsychotics [4]. However, SGAs cause metabolic disorders including obesity, hyperlipidemia, and diabetes [5,6]. Several studies have shown that the incidence of diabetes is higher in patients treated with SGAs [7,8]. According to a meta-analysis that evaluated 25 studies, schizophrenia patients treated with SGAs exhibited a 2.5 times higher risk of developing type 2 diabetes (T2D), compared to the control group [9]. SGA-induced diabetes can occur via various mechanisms involving SGA-induced insulin resistance and β-cell damage [10]. Patients with SGA-induced diabetes were 74% more susceptible to developing acute complications and showed higher mortality than the general population [11].
Diabetes is characterized by hyperglycemia (fasting plasma glucose level >126 mg/dL [7 mmol/L]) due to insufficient insulin production or insulin resistance [12]. Autoimmune damage to pancreatic cells results in type 1 diabetes (T1D) due to complete insulin deficiency. In contrast, T2D is caused by insulin resistance in cells that do not respond to insulin stimulation or cell dysfunction [12]. The association between diabetes and psychosis is complex and multifactorial. Risk factors for T2D, such as a sedentary lifestyle or poor diet, are more common in the population with psychotic disorders than in the general population. A sedentary lifestyle involves very little physical activity and primarily involves sitting or lying down for extended periods. Obesity is approximately 1.5 to 2.0 times more prevalent in patients with schizophrenia. Antipsychotic drugs contribute to diabetes by either inducing weight gain or promoting insulin resistance [13].
Hyperglycemic crisis is a metabolic emergency associated with uncontrolled diabetes, including the hyperosmotic hyperglycemic state (HHS) and diabetic ketoacidosis (DKA). Relative or absolute insulin deficiency and excessive regulation of hormones (glucagon, cortisol, catecholamine, and growth hormones) cause hyperglycemia and ketone body accumulation. Unlike in DKA, in HHS, higher insulin levels inhibit ketone production and limit metabolic acidosis. DKA is more common in young people with T1D, whereas HHS is more frequently reported in adult and elderly patients with T2D. However, many patients exhibit both HHS and DKA, and both DKA and HHS can occur in patients with T1D and T2D [14,15]. In a previous multicenter, retrospective cohort study, 59.4% of hyperglycemic emergency cases in patients aged 18–65 were attributed to DKA, compared to 9.6% of HHS hospitalizations. In contrast, these events were reported with a similar frequency of DKA and HHS hospitalizations in patients of age >66 years old. Therefore, clinicians should be careful about the possibility of DKA when prescribing antipsychotics to young and old patients, who are typically considered a risk group [15].
DKA is an acute complication of diabetes characterized by uncontrolled hyperglycemia, metabolic acidosis, and increased ketone bodies. Since it can be life-threatening, treatment should be started immediately and can reduce sequelae [16]. SGAs such as olanzapine, clozapine, risperidone, and quetiapine can cause DKA, and the average treatment period to onset may be about six months [17]. Although some mechanisms of DKA have been associated with SGAs, these associations remain uncertain. Several cases of antipsychotics-induced DKA have been reported, among which cases with the first sign of DKA characteristically presented in psychiatric patients without underlying diabetes [18]. Interestingly, the incidence of DKA in schizophrenia is 10-fold higher than that in the general population. One study reported that DKA occurred in 5 out of 11 individuals using antipsychotic medications [19]. The overall mortality rate in patients exposed to antipsychotics was 26.5% [20]. Despite the high risk of mortality, there has been little attention to DKA in the context of SGA use [21].
As psychiatric patients often use antipsychotic drugs chronically for extended periods, these side effects should be considered seriously [22,23]. It is noteworthy that the number of patients who have been prescribed antipsychotics has increased over the past decade [24]. Therefore, it is necessary to consider the occurrence of DKA with the use of SGAs. We present the case of a patient with schizophrenia who was taking antipsychotic medications but had no history of diabetes. This case report and review provides an overview of DKA and focuses on the molecular mechanisms through which antipsychotics can cause DKA.
CASE PRESENTATION
A 35-year-old male presented with dyspnea and a drug overdose that started 10 days before admission to the emergency room. He was diagnosed with schizophrenia 14 years ago and had been receiving long-acting injectable palmitate 234 mg once a month for 9 months, in addition to the oral administration of lithium 900 mg, quetiapine 400 mg, and lorazepam 0.5 mg daily. His auditory hallucinations, persecutory delusions, and depressive feelings had worsened 15 days back. There was no history of administration of any other medication or herbal supplement. His blood glucose and HbA1c levels 6 months back were 123 mg/mL and 5.9%, respectively. He was 174 cm tall and weighed 120 kg with a body mass index of 39.6 kg/m2. There was no prior diagnosis of diabetes, hypertension, or hyperlipidemia (Figure 1).
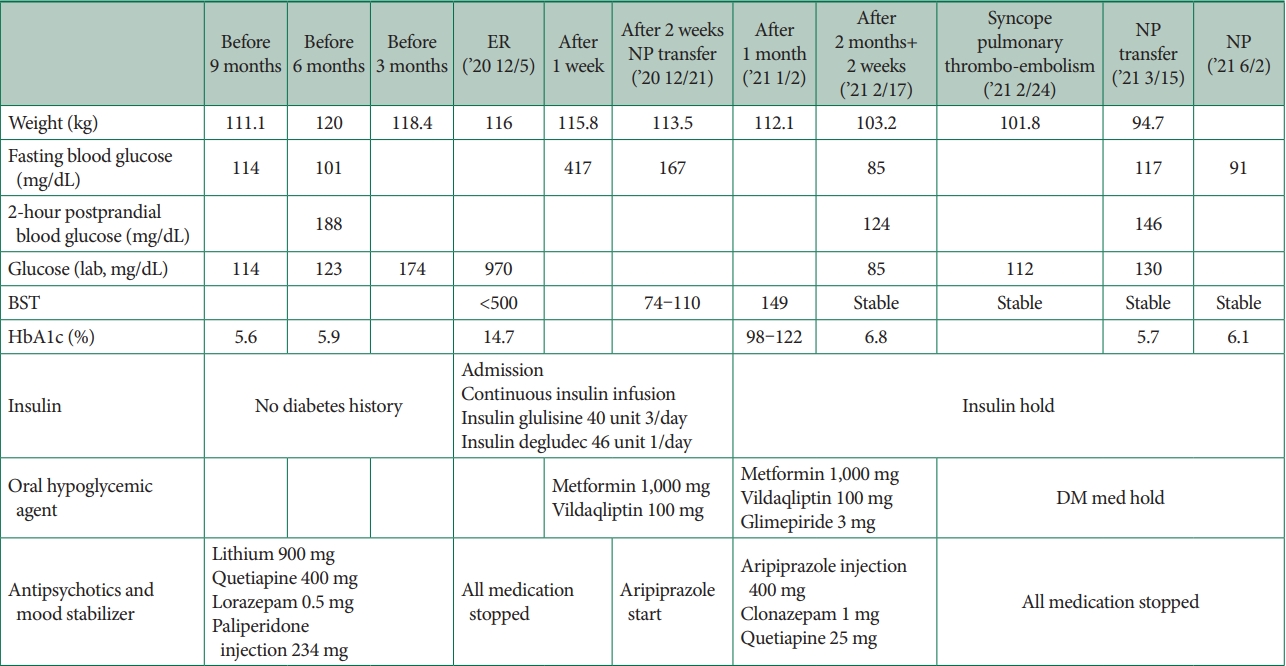
Flow chart illustrating the clinical progression of the case patient. ER, emergency room; NP, neuropsychiatry ward; BST, blood sugar test; DM, diabetes mellitus.
Physical examination revealed signs of acute illness and alert consciousness. At the time of admission, his blood pressure was 99/55 mm Hg, heart rate was 98 beats/min, respiratory rate was 32 breaths/min, and body temperature was 36.7°C. His weight was 116 kg, with a weight loss of 4 kg compared to that 6 months back.
Laboratory findings showed no abnormalities in the complete blood count. However, serum biochemical analysis revealed elevated blood glucose, blood urea nitrogen, and creatinine levels of 970 mg/dL, 34.2 mg/dL, and 2.78 mg/dL, respectively. The sodium level had decreased to 120 mEq/L, while the potassium level and serum osmolality had increased to 5.6 mEq/L and 342 mOsm/kg, respectively. The HbA1c level was 14.4%, while the ketone level had increased to 4.1 mmol/L. Arterial blood gas analysis showed metabolic acidosis with a 6.848 pH and 20.1 mm HgpCO2, 64.6 mm HgpO2, 3–3.5 mmol/L HCO, and 28 mmol/L lactate (reference range: 4.5–14.4) levels. The C-peptide level was 0.79 ng/mL, indicating diminished insulin secretion, and tests for both anti-insulin and anti-GAD antibodies were negative. The lithium level was 0.34 mmol/L.
After the diagnosis of DKA, all previously administered medications were discontinued, and the patient was admitted to the endocrinology department for aggressive fluid therapy, intravenous insulin administration, and electrolyte correction. After 1 week of hospitalization, his fasting blood glucose level was 417 mg/dL, and he began taking oral hypoglycemic agents in addition to insulin. The C-peptide level recovered to 2.04 ng/mL, indicating normal insulin secretion. After 2 weeks, the fasting blood glucose level was 167 mg/dL. After being transferred to the psychiatric department, he was administered aripiprazole. Insulin treatment was stopped one month after admission, and only oral hypoglycemic agents were continued. Two months after admission, the patient experienced shortness of breath and presyncope with cyanosis. On examination, his heart rate was regular but elevated at 128 beats/min, his blood pressure was 101/72 mm Hg, and his respiratory rate was 32 breaths/min; the oxygen saturation level of the room air was 85%. The D-dimer test results were positive, and further evaluation with computed tomography pulmonary angiography confirmed the presence of a pulmonary thromboembolism. Thrombi were detected in the main, superior, and inferior pulmonary arteries and the segmental branches. The patient received anticoagulant treatment with intravenous heparin and an oral anticoagulant, which resolved tachycardia and hypoxia within 10 days of treatment. After 3 months, the patient was able to discontinue the oral hypoglycemic agent, and their fasting blood sugar, postprandial blood sugar 2 hours after a meal, and HbA1c levels were 117 mg/dL, 146 mg/dL, and 5.7%, respectively. After 6 months, the patient’s fasting blood sugar level improved to 91 mg/dL, whereas the HbA1c level was 6.1% without the need for oral hypoglycemic agents. This case report was approved by the Clinical Trials Review Committee of the Veteran’s Health Service Medical Center (IRB No. 2023-06-012).
LITERATURE REVIEW METHODS
We analyzed the effects of antipsychotic drugs on DKA. Our eligibility criteria were as follows: english-language papers published from 2002 to 2021 in electronic databases, including Elsevier, PubMed, IEEE, SpringerLink, and Google Scholar. We included papers with keywords such as hyperglycemia, DKA, hyperosmolar hyperglycemic syndrome, SGA, clozapine, olanzapine, risperidone, quetiapine, ziprasidone, and aripiprazole. Exclusion criteria were limited to case reports.
A total of 117 papers examining the relationship between atypical antipsychotics and diabetes mellitus (DM) or DKA, as well as research papers identifying the underlying mechanisms, were included; of these, 38 duplicate papers and 47 single case reports were excluded. Each potentially relevant paper underwent a comprehensive review of its full text to ensure that it met the established eligibility criteria. Finally, we included 32 studies that were most relevant and closely aligned with our eligibility criteria in our analysis (Tables 1 and 2). This literature review was approved by the Clinical Trials Review Committee of the Veteran’s Health Service Medical Center (IRB No. 2022-03-015).

Summary of the literature review results (human)

Summary of the literature review results (animal models and cell lines)
RESULTS
The patient was admitted to the emergency room after presenting with worsening psychosis, dyspnea, and polydipsia after taking excessive antipsychotics. He had no medical history of T1D or T2D. However, he was diagnosed with DKA after admission. The primary underlying causes of DKA and HHS include either a partial or complete lack of insulin, or an abundance of counter-regulatory hormones (Figure 2).

Pathophysiology of hyperglycemic emergencies and antipsychotics. Second-generation antipsychotics can induce insulin resistance either directly or through obesity. Increased food intake can lead to obesity and insulin resistance. Moreover, antipsychotics can reduce insulin secretion, which is associated with absolute insulin deficiency, from β-cells. FFAs, free fatty acid.
Mechanisms for SGA-induced DKA: focusing on molecular pathways
The pathophysiology of DKA requires insulin deficiency and an increase in counter-regulatory hormones (glucagon, catecholamines, and cortisol). In contrast, under hyperosmotic hyperglycemic state (HHS) conditions, insulin levels are relatively high, inhibiting ketone production and metabolic acidosis [15]. Insulin deficiency occurs under the complete loss of β-cell function over extended periods. However, this is not always the case because some patients present within a few years of diagnosis where complete β-cell dysfunction is impossible [25]. Studies have suggested that the mechanism could involve relative insulin deficiency and increased lipolysis caused by counter-regulatory hormones [26]. Insulin deficiency and counter-regulatory hormone increase leads to hyperglycemia and ketoacidosis. Hyperglycemia occurs due to increased gluconeogenesis, accelerated glycogenolysis, and impaired glucose use in peripheral tissues. This is amplified by hormone imbalances and temporary insulin resistance. Ketoacidosis occurs when free fatty acids are liberated from adipose tissues into the blood, and uncontrolled fatty acid oxidation is induced in the liver.
Insulin deficiency: impairment of insulin signaling pathways
Alterations in the insulin signaling pathway associated with SGAs may occur in hepatocytes and skeletal muscles. SGAs affect the insulin signaling pathway in two ways: inhibition of insulin receptor substrate 1/2 (IRS-1/2) phosphorylation, and inhibition of Akt and glycogen synthase kinase-3 (GSK3) phosphorylation. A previous study found that olanzapine attenuated IRS-1 phosphorylation in insulin-stimulated human wild-type fibroblasts [27].
Male Sprague-Dawley rats treated with olanzapine (10 mg/d) for 8 weeks showed significantly reduced IRS-2 levels, reduced GSK3α-Ser21 phosphorylation, and increased GSK3β-Ser9 phosphorylation, which directly inhibit the hepatic insulin signaling pathway [28,29]. In contrast, another study reported that olanzapine (5 mg/kg/d) treatment for 8 weeks in the same mouse model increased IRS-1 Ser307 and IRS-2 Ser731 phosphorylation. This result demonstrated that the increase in baseline insulin triggers proteasomal degradation, finally resulting in the blockade of insulin signaling pathways [28]. SGAs also promote the decrease in Akt/GSK phosphorylation, a critical node of insulin signaling in the liver [30]. Oral olanzapine (3 mg/kg/d) or clozapine (20 mg/kg/d) treatment in female Sprague-Dawley rats for 9 weeks reduced hepatic Akt and GSK3β phosphorylation at the Ser9 and Ser473 levels, respectively [31].
Similar to hepatocytes, SGAs interfere with the insulin signaling pathway in skeletal muscle cellular models. The study showed that the Rat L6 skeletal muscle cells treated with olanzapine (10 and 100 µM) for 72 hours blocked IRS-1 phosphorylation and decreased Akt and GSK-3 phosphorylation [32]. In line with this finding, clozapine (1.5 µM) treatment using PC-12 cells and L6 skeletal muscle cells as a model of the brain and peripheral tissue, respectively, reduced the effect of insulin on insulin receptors by 40% and on insulin-induced IRS-1 tyrosine phosphorylation by 60% in 24 hours. Akt phosphorylation at Ser473 had decreased by approximately 40% [33].
Decrease in insulin secretion of pancreatic β-cells
Insulin secretion is tightly controlled by pancreatic β-cells. Pancreatic β-cells express various dopaminergic, serotonin, and cholinergic muscarinic receptors involved in insulin secretion.
There are five types of dopamine receptors, and the D2 and D3 receptors have been identified as those associated with insulin secretion. Dopamine is secreted along with insulin in a hyperglycemic state, released into the extracellular space, binds to D2 receptors, and partially suppresses insulin secretion by decreasing cell membrane depolarization and increasing cytosolic calcium influx [34]. Prolonged D2 blockade may lead to the depletion of insulin and an eventual defect in pancreatic compensation [35]. In addition, another study showed that dopaminergic negative feedback in mouse pancreatic islets was abolished by a specific antagonist of the dopamine receptor D3. D3 receptor activation results in changes in intracellular calcium dynamics, leading to reduced insulin secretion [36].
Serotonergic receptors are also expressed in response to glucose stimulation, and extracellular 5-HT may act as a stimulator or inhibitor of insulin secretion depending on the expression of different 5-HT receptor subtypes [37]. A study reported that selective serotonin reuptake inhibitors can reduce insulin secretion in isolated islets and β-cell lines, like direct 5HT2c agonists [35]. This study suggested that SGAs that exhibit partial agonist activity against 5HT2a/c receptors may adversely affect insulin secretion [38]. SGAs inhibit M3R action on glucose-dependent parasympathetic regulation of insulin secretion. Grajales et al. [10] reported that olanzapine and clozapine suppress M3R, which decreases cholinergic-stimulated insulin secretion by directly blocking these receptors in β-cells [10]. M3R is also located in the brain and can be affected by SGAs. Disruption of M3R density in the brain has also been observed in female Sprague-Dawley rats treated with olanzapine (0.25–2.0 mg/kg) which resulted in an up-regulation of M3R in the hypothalamic arcuate ventromedial nuclei and dorsal vagal complex of the brainstem. Elevated hypothalamic M3R levels negatively correlate with peripheral insulin levels [39].
Increase in counter-regulatory hormones
Several studies have reported that SGAs increase glucagon levels in pancreatic alpha cells. In male Sprague-Dawley rats injected with octreotide (250 mg/kg) for 5 min, clozapine increased glucagon levels despite an increase in both blood glucose and plasma insulin levels [40]. Similarly, male Wistar rats received intravenous injections of clozapine (2.5, 5, and 10 mg/kg). After clozapine administration, glucagon levels increased dosedependently at 2.5–10 mg/kg [41]. These results suggested that clozapine directly stimulates glucagon secretion.
Chronic treatment of male Sprague-Dawley rats with clozapine (10 mg/kg) or quetiapine (10 mg/kg) for 42 days increased insulin and glucagon levels [42]. Castellani et al. [43] previously reported that glucagon levels were higher in rats following clozapine (structurally similar to olanzapine) administration, and that this increase significantly contributed to elevated blood glucose levels [43]. Another possible mechanism through which SGAs could disturb insulin homeostasis is by suppressing the release of incretins, which amplify glucose-mediated insulin release from the gut [44].
DISCUSSION
Case reports of DKA induced by SGAs are infrequent [15,45,46]. DKA cases reported in other countries are 6, 18, 29, 7, and 9 for aripiprazole, clozapine, olanzapine, quetiapine, and risperidone, respectively [47]. In South Korea, DKA cases for clozapine, olanzapine, risperidone, and paliperidone were 1, 2, 3, and 2, respectively [48]. The average age of DKA onset among individuals taking antipsychotics was 37.5 years, with the majority falling within the 20–39 years age group, wherein 30–39 years accounted for 70% and 20–29 years for 20% [47]. In the present case, the patient was 35 years old, falling within this age range. Although the patient had not been previously diagnosed with DM, he had several risk factors that could lead to metabolic disease. He had been diagnosed with schizophrenia, was severely obese, and was taking two different SGAs; an overdose was suspected 10 days before admission. However, the exact cause of DKA, and not of HHS, was unclear. It is possible that severe psychological stress led to an excessive secretion of the stress hormone cortisol, and the concurrent use of lithium may have exacerbated dehydration, possibly contributing to DKA.
Patients treated with SGAs may exhibit dysfunctions in glucose metabolism [48,49]. Metabolic abnormalities include dry mouth, loss of appetite, and weight change. Hyperglycemia in DKA presented with polydipsia and polyuria that had occurred several days back. Metabolic acidosis is associated with acute symptoms of nausea, vomiting, and abdominal pain, as well as weight loss and general weakness. Aggravation of metabolic acidosis can progress to confusion or coma [42]. However, as these symptoms are similar to the side effects of SGAs, it is difficult to differentiate them clinically. Therefore, periodic observation and examination are important for patients taking SGAs [50]. In addition, DKA is caused by physical or mental stress, such as infection or surgery, in patients with insulin deficiency [43]. SGA-induced DKA, mediated by the abovementioned mechanisms, may occur even in the absence of previous conditions influencing its occurrence [51,52].
Sudden premature death has been reported in patients treated with SGAs [53]. A previous study reported that 391 patients with schizophrenia had 5 cases of DKA and 14 cases of pulmonary thromboembolism. One-third of the causes of death in DKA are thromboembolic, with septic embolisms. This is because hypercoagulation occurs owing to changes in the vascular endothelium and coagulation factors, and dehydration increases blood viscosity, leading to thrombosis. Similarly, the patient in the current case experienced fatal pulmonary thromboembolism as well. It is essential to be aware of these potential risks and closely monitor patients for adverse effects during treatment with antipsychotics.
Prevention
The guidelines of the American Diabetes Association and American Psychiatric Association published in 2004 and the Korean Medication Algorithm for Schizophrenia 2019 recommend checking the patient’s medical history, family history, height, weight, body mass index, waist circumference, blood pressure, fasting blood sugar, and lipid abnormalities before taking SGAs [15,54]. Weight should be monitored at regular outpatient visits at 4, 8, and 12 weeks after treatment with SGAs and thereafter. Blood pressure, fasting blood sugar, and lipid abnormalities were assessed at 12 weeks after the administration of SGAs. Subsequently, blood pressure and fasting blood sugar levels should be monitored annually, and lipid abnormalities should be monitored every five years. In addition to the above guidelines, recent reports recommend checking weight, fasting blood sugar, and lipid abnormalities quarterly for 1 year after 12 weeks of SGA treatment. It is hard to provide sufficient evidence to validate risk factors associated with the development of SGA-induced DKA. Individuals with risk factors for DM, such as obesity, immobility, and atypical antipsychotic intake, are at a higher risk of hyperglycemic crisis. However, the mechanism underlying the occurrence of DKA due to an absolute deficiency of insulin in these individuals has not been established. Nevertheless, we hope that this case report and review will lay the foundation for elucidating the mechanism of SGA-induced DKA in the future.
CONCLUSION
SGAs are associated with DKA, a hyperglycemic emergency. SGA-related DKA may be mediated by the mechanisms described earlier. It can be caused by insulin deficiency due to the impairment of insulin signaling pathways, inhibition of insulin secretion, and increase in counter-regulatory hormones. This mechanism causes DKA even in patients without underlying diabetes or obesity. Sudden premature death has been reported in patients exposed to antipsychotics. DKA is a fatal condition; therefore, prevention and prompt treatment are required. Therefore, clinicians should follow the guidelines for prevention and carefully examine patient symptoms during treatment with SGAs for extended periods. Clinicians should be aware that individuals with risk factors for DM, such as severe obesity, immobility, and irregular atypical antipsychotic intake, are at a higher risk of hyperglycemic crisis.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Hayun Choi. Data curation: Heewon Bae, Sungsuk Je. Formal analysis: Heewon Bae, Hayun Choi. Funding acquisition: Hayun Choi. Investigation: Heewon Bae, Ji Hyun Lee, Sungsuk Je. Methodology: Heewon Bae, Sungsuk Je, Hayun Choi. Project Administration: Sungsuk Je, Hayun Choi. Resources: Hayun Choi, Seung-Hoon Lee. Software: Sungsuk Je, Hayun Choi. Supervision: Ji Hyun Lee, Hayun Choi. Validation: Ji Hyun Lee, Sungsuk Je. Visualization: Heewon Bae. Writing—original draft: Heewon Bae. Writing—review and editing: Ji Hyun Lee, Hayun Choi.
Funding Statement
This study was supported by the VHS Medical Center Research Grant, Republic of Korea (grant number: VHSMC 22033).
Acknowledgements
We would like to express our deepest gratitude to the study coordinator, Aram Park (Veteran Health Service Medical Center) and the professor Joon Ho Moon (Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine), who made valuable contributions to this work.