The Effect of Psychological Inflexibility on Social-Distancing Phobia Mediated by Preoccupation With Sleep and Intolerance of Uncertainty in the Elderly Population During the COVID-19 Pandemic
Article information

Abstract
Objective
The aim of this study was to explore whether psychological inflexibility in the elderly population is related to social-distancing phobia, and examine whether their viral anxiety, preoccupation with sleep, or intolerance of uncertainty may mediate the relationship.
Methods
Among the elderly population aged ≥65 in Korea, we conducted an anonymous online survey during January and February 2023. We collected the responses of 300 participants, collected demographic information, and symptoms using rating scales such as the Social-Distancing Phobia scale, Stress and Anxiety to Viral Epidemics-6 items (SAVE-6), Intolerance of Uncertainty Scale-12 (IUS-12), Acceptance and Action Questionnaire-II (AAQ-II), and Glasgow Sleep Effort Scale (GSES).
Results
Social-distancing phobia was expected by the SAVE-6 (β=0.34, p<0.001), IUS-12 (β=0.18, p=0.003), and GSES (β=0.18, p=0.001) in the linear regression analysis. In the mediation analysis, psychological inflexibility did not directly influence social-distancing phobia. However, viral anxiety, intolerance of uncertainty, or preoccupation with sleep completely mediated the influence of psychological inflexibility on social-distancing phobia among elderly population.
Conclusion
The management of psychological inflexibility, intolerance of uncertainty, or preoccupation with sleep needs to be considered when designing interventions to address social-distancing phobia in elderly populations in future pandemics.
INTRODUCTION
During the past three years of the coronavirus disease-2019 (COVID-19) pandemic, physical distancing (or social distancing) was one of the most effective and useful strategies to prevent viral transmission [1]. The practice entails staying at least two meters away from others in crowded public places, avoiding large crowds, and minimizing non-essential travel [2]. This policy was helpful in slowing down the spread of the virus, reducing the infection or mortality rates from the virus, and reducing the burden placed on healthcare systems [3]. However, the term physical distancing was changed from social distancing [4], because the latter insinuates being ignored, unwelcome, left alone, and even being excluded from society. On the other hand, people may fear social closeness because of the physical distancing policy. When confronted with people who do not wear masks or who demonstrate symptoms like coughing or sneezing, one may experience a greater level of fear. This may lead to viral anxiety or social-distancing phobia [5,6].
People at high risk of COVID-19 infection [7] in particular might fear physical closeness in public. As an example, cancer patients may experience anxiety due to viral epidemic (viral anxiety) or be afraid of physical closeness while undergoing treatment at the medical center, as they believe their impaired immune function makes them susceptible to infection [8]. The elderly population is likely to be affected the most by viral infection. It has been reported that 80% of the deaths caused by COVID-19 occurred in individuals over the age of 65 [9]. Some countries have adopted stricter lockdown measures to protect older individuals [10] who are a high-risk group [11]. As a result of being socially isolated, the elderly suffer from loneliness and depression [12]. The socially isolated state itself might induce viral anxiety or depression among the elderly, though viral anxiety or depression may rather lead to self-isolation to prevent the viral infection as a form of social-distancing phobia [6] or adherence to physical distancing [3].
Insomnia is also a highly reported psychiatric symptom [13] among the elderly [14]. Although insomnia is prevalent among the general population [15] even when the coronavirus is not present, sleep disturbances were prevalent during the COVID-19 pandemic. We previously reported that insomnia can mediate the influence of viral anxiety on preoccupation with the coronavirus [16], and sleep-related dysfunctional beliefs make cancer patients to avoid crowded public places [8]. The feasibility of using the “anxiety-dysfunctional beliefs about sleep-distancing” model needs to be investigated in the elderly population.
To prevent or reduce this psychological distress, coping strategies such as resilience, self-efficacy, or cognitive emotional regulation were proposed [17,18]. Psychological flexibility was reported as one of the psychological states which can reduce one’s depression, anxiety, or insomnia during the COVID-19 pandemic [19]. Psychological inflexibility is the rigid dominance of psychological responses over values and contingencies as the determining factor in guiding action [20] that is characterized by persistent avoidance of adverse internal or external events [21]. In the elderly population, it was reported that psychological flexibility might reduce their death anxiety. During this COVID-19 pandemic, psychological flexibility was also suggested as a potential means of reducing the negative consequences of social isolation [22].
Another psychological status, intolerance of uncertainty, might have a role in the association between viral anxiety and social-distancing phobia. In the general population in Korea, we reported that intolerance of uncertainty mediated the influence of viral anxiety on social-distancing phobia [6]. Furthermore, intolerance of uncertainty among healthcare workers may increase adherence to the physical distancing policy [3]. In the elderly population, the feasibility of the “anxiety-uncertainty-distancing” model needs to be investigated. Since psychological inflexibility was reported to be related to intolerance of uncertainty [22], we can consider that this relationship may play a role in social-distancing phobia in the elderly population.
In this study, we aimed to explore the feasibility of two models of “anxiety-uncertainty-distancing” and “anxiety-dysfunctional beliefs about sleep-distancing” in the elderly population. Furthermore, we explored whether psychological inflexibility in the elderly population is related with social-distancing phobia, and examined whether their viral anxiety, preoccupation with sleep, or intolerance of uncertainty may mediate the relationship. We hypothesized that 1) psychological inflexibility will be positively associated with social-distancing phobia, 2) viral anxiety will be positively associated with social-distancing phobia, 3) preoccupation with sleep will be positively associated with social-distancing phobia, 4) intolerance of uncertainty will be positively associated with social-distancing phobia, and 5) psychological states including viral anxiety, preoccupation with sleep, or intolerance of uncertainty will mediate the influence of psychological inflexibility on social-distancing phobia in the elderly population.
METHODS
Participants and procedure
Among the elderly population aged ≥ 65 in Korea, we conducted an online survey via a professional survey company, EMBRAIN (www.embrain.com) during January and February 2023. We collected the responses of 300 participants, and the sample size was calculated by allocating 30 samples across 10 cells (biological sex X five regions of Korea) [23]. The company sent enrollment emails to 1,822 of 6,460 elderly individual panelists on the survey platform; 451 participants accessed and 343 completed the survey. The first 300 samples excluding incomplete or too rapid responses were delivered to the researchers. We collected demographic information, psychiatric history, medical disease history, and information on current psychological distress. Questions regarding COVID-19 (experiences of being infected, quarantined, and vaccinated) were included in the survey form. The e-survey form was developed according to the Checklist for Reporting Results of Internet e-Surveys guidelines [24]. The study protocol was approved by the Institutional Review Board (IRB) of Asan Medical Center (2022-1707). Though obtaining the written informed consent was waived, we collected responses of participants who agreed to participate in this survey at the time of access to the survey form.
Measures
Social-Distancing Phobia scale
The Social-Distancing Phobia scale is a self-report rating scale which can measure one’s level of phobia to social closeness during the pandemic [5]. It consists of 17 items which can be rated on a 5-point Likert-type scale. The total score ranges from 17 to 85, and a higher total score means greater level of phobia to social closeness. In this study, the Korean version of the scale was applied [6], and Cronbach’s alpha among this sample was 0.943.
Stress and Anxiety to Viral Epidemics-6 items
Stress and Anxiety to Viral Epidemics-6 items (SAVE-6) scale is a self-report rating scale designed to assess one’s level of viral anxiety in the context of the COVID-19 pandemic [25]. This scale was developed from the original SAVE-9 scale, which measured healthcare workers’ response to the viral epidemic [26]. There are six items in the SAVE-6 that can be rated on a Likert scale from 0 (never) to 4 (always). Those with a higher total score, ranging from 0 to 24, exhibit a higher level of viral anxiety. In the original version, the SAVE-6 scale was developed in Korean. In this sample, Cronbach’s alpha was 0.889.
Intolerance of Uncertainty Scale-12
The Intolerance of Uncertainty Scale-12 (IUS-12) is a shortened version of the IUS [27], which is used to measure one’s tolerance for uncertainty. The questionnaire contains 12 items that can be rated according to the level of agreement (1–7). An increased total score indicates a greater tolerance for uncertainty. We applied the Korean version of the IUS-12 scale [28] in this study, and Cronbach’s alpha was 0.911 in this sample.
Acceptance and Action Questionnaire-II
The Acceptance and Action Questionnaire (AAQ) [21] is a measure of experiential avoidance and psychological inflexibility, originally developed within the Acceptance and Commitment Therapy. It was revised as AAQ-II [20]. This questionnaire contains seven Likert-type items with seven response options, where 1 means “never true” and 7 means “always true”. A higher total score reflects a higher level of psychological inflexibility. In this study, we applied the Korean version of the AAQ-II [29], and Cronbach’s alpha among this sample was 0.869.
Glasgow Sleep Effort Scale
The Glasgow Sleep Effort Scale (GSES) is a rating scale designed to measure the persistent preoccupation with sleep [30]. Seven items of the GSES can be rated on a three-point Likert scale, and a higher total score reflects a greater preoccupation with sleep. The Korean version of GSES [31] was applied in this study, and Cronbach’s alpha among this sample was 0.837.
Statistical analysis
Demographic characteristics are presented as means and standard deviations. An acceptable significance level was defined as two tailed, p<0.05. The Pearson’s correlation coefficients were calculated to examine the association between social-distancing phobia and the SAVE-6, GSES, IUS-12, and AAQ-II scores. In order to identify the factors that predispose the elderly population to social-distancing phobia, linear regression analysis with enter methods was conducted. A mediation analysis was conducted to examine the feasibility of two proposed models in the elderly population and the mediating effect of viral anxiety, preoccupation with sleep, or intolerance of uncertainty on the association between psychological inflexibility and social-distancing phobia by implementing the bootstrap method with 2,000 resamples. The statistical analysis was conducted using SPSS version 21.0 (IBM Corp., Armonk, NY, USA), AMOS version 27 (IBM SPSS., Chicago, IL, USA) and JASP version 0.14.1.0 (JASP Team, Amsterdam, Netherlands).
RESULTS
All 300 elderly individuals participated in this study. Their mean age was 68.2±3.5 years old, and 62.0% were male (Table 1). About 84.3% were living with their spouse or descents, and 13.7% lived alone. About half (54.3%) had been infected, and 90.7% were vaccinated. 11.7% had a psychiatric past history, and 9.7% currently had psychological distress.
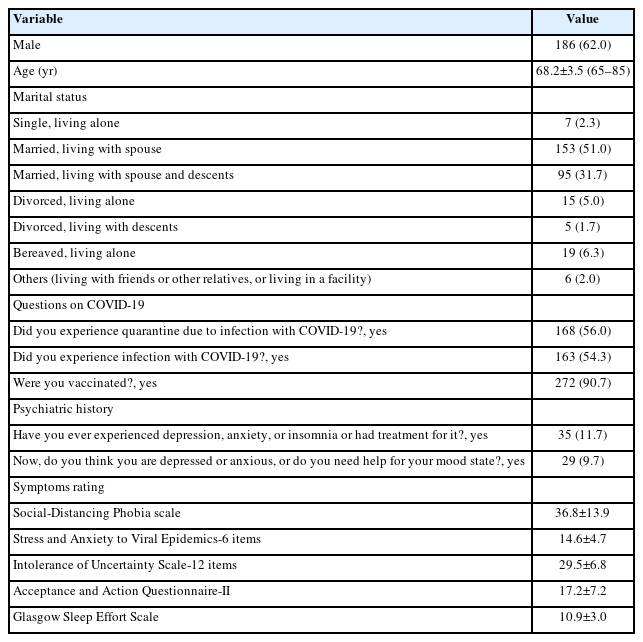
Clinical characteristics of the study participants aged ≥65 years old (N=300)
In Table 2, Pearson’s correlation coefficients were presented. Social-distancing phobia was significantly correlated with the SAVE-6 (r=0.47), IUS-12 (r=0.39), AAQ-II (r=0.32), and GSES (r=0.40) (all p<0.01). The SAVE-6 was correlated with IUS-12 (r=0.31), AAQ-II (r=0.28), and GSES (r=0.35) (all p<0.01). The IUS-12 score was significantly correlated with the AAQ-II (r=0.55) and GSES (r=0.44) (all p<0.01), and the AAQ-II was correlated with the GSES (r=0.32, p<0.01).

Correlation coefficients of each variable among participants aged ≥65 years old (N=300)
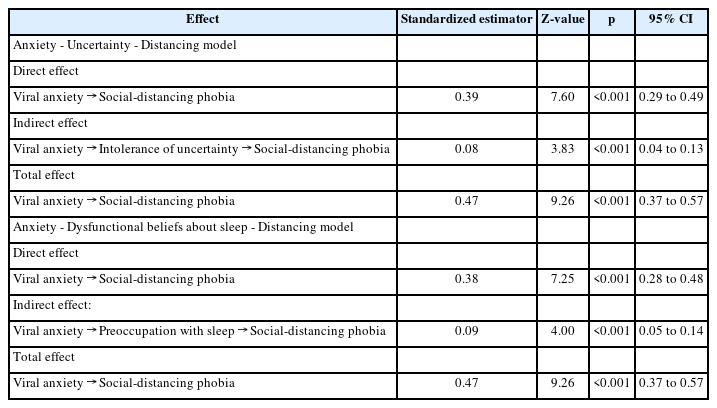
Social-distancing phobia was expected by the SAVE-6 (β= 0.34, p<0.001), IUS-12 (β=0.18, p=0.003), and GSES (β=0.18, p=0.001) (Table 3) in the linear regression analysis. The feasibility of the two models was examined using a mediation model (Table 4). The anxiety-uncertainty-distancing model was feasible, and the anxiety-dysfunctional-beliefs-about-sleep-distancing model was also feasible among the elderly population. In the final mediation analysis (Table 5 and Figure 1), the AAQ-II was not one of expecting variables for social-distancing phobia. In the medication analysis, psychological inflexibility did not directly influence social-distancing phobia. However, viral anxiety, intolerance of uncertainty, or preoccupation with sleep completely mediated the influence of psychological inflexibility on social-distancing phobia among the elderly.
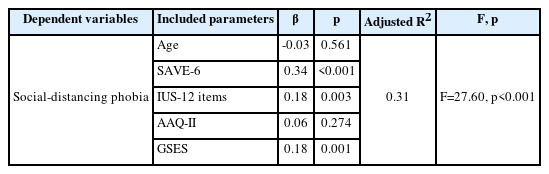
Linear regression analysis to explore variables which predispose to preoccupation with coronavirus among participants aged ≥65 years old (N=300)
The feasibility of proposed distancing models among participants aged ≥65 years old (N=300)

The results of direct, indirect, and total effects on mediation analysis among participants aged ≥65 years old (N=300)

Mediation model showing the pathway from the effect of psychological inflexibility (independent variables) on social-distancing phobia (outcome) through viral anxiety, intolerance of uncertainty, or preoccupation with sleep (mediator) among participants aged ≥65 years old. **p<0.01.
DISCUSSION
In this study, we observed that an elderly person’s socialdistancing phobia was significantly correlated with psychological inflexibility, intolerance of uncertainty, viral anxiety, and insomnia severity in the correlation analysis. However, in the linear regression analysis, psychological inflexibility could not be included as one of the predisposing variables for social-distancing phobia. Mediation analysis also showed that psychological inflexibility could not directly influence the socialdistancing phobia, but viral anxiety, intolerance of uncertainty, and preoccupation with sleep mediated the relationship among elderly population.
Worry was explained using a model with intolerance of uncertainty [32]. We observed that viral anxiety and intolerance of uncertainty were correlated with social-distancing phobia in the elderly population in accordance with the previous study [6] done in the general population. This anxiety-uncertainty-distancing model is useful to explain how an individual becomes phobic to physical closeness (social-distancing phobia). If one has viral anxiety and intolerance of uncertainty, they feel anxious about being infected, and as a result, they can become phobic to physical closeness in public. This model can be feasible when explaining the adherence to physical distancing. Even though adherence to physical distancing does not arise from social-distancing phobia only, people may adhere to physical distancing when they experience viral anxiety and intolerance to uncertainty [3].
Our study showed that psychological inflexibility could play a role in the anxiety-uncertainty-distancing model. Though psychological inflexibility in the elderly population did not directly influence social-distancing phobia, viral anxiety and intolerance of uncertainty completely mediated this relationship. These results show that psychological inflexibility might have been associated with social-distancing phobia during the COVID-19 pandemic. During this pandemic, it was reported that psychological flexibility was important to mental health [33] or well-being [34] during lockdown [35]. In addition, psychological inflexibility, together with intolerance of uncertainty, mediated social isolation and psychological distress [22]. In addition, state anxiety was predicted by intolerance of uncertainty and psychological inflexibility [36].
Furthermore, viral anxiety in the elderly population was related to psychological inflexibility. It is well known that anxiety symptoms are associated with psychological inflexibility [37]. During this pandemic, viral anxiety was one of the most important issues that needed to be addressed. It was reported that physical distancing influenced viral anxiety [38]. We reported that viral anxiety mediated the influence of intolerance of uncertainty on adherence to physical distancing among healthcare workers [3] or mediated the influence of perceived benefits of the health-belief model on adherence to physical distancing [39]. On the other hand, intolerance of uncertainty mediated the influence of viral anxiety on social-distancing phobia [6]. In this regard, viral anxiety and physical distancing are double-edged swords. Viral anxiety influences people’s fear of physical closeness. However, this seems beneficial, since it may allow people to adhere to physical distance in serious situations [40]. In the current study, we observed that viral anxiety in the elderly population mediated the influence of psychological inflexibility on their social-distancing phobia.
Insomnia was also an important psychiatric symptom during this pandemic. Dysfunctional beliefs about sleep or preoccupation with sleep, which insomnia patients usually have, influenced anxiety, depression, and insomnia during this pandemic [41]. This was particularly true of cancer patients who had dysfunctional beliefs about sleep because they are a high-risk group that could be easily infected. Furthermore, sleep disturbance may impair immune function and consequently be detrimental to their health [8]. This can be a model of anxiety-dysfunctional beliefs about sleep-distancing. It explains how an individual who suffers from insomnia and is preoccupied with sleep becomes phobic to physical closeness. The results of the current study showed that this model is feasible in the elderly population, and preoccupation with sleep can mediate the influence of psychological inflexibility on social-distancing phobia.
This study had several limitations. First, the survey was done three years after the first wave of the pandemic. Hence, participants’ response to a question needed to be interpreted cautiously, as they had adapted to the COVID-19 pandemic. Second, this study was conducted using an online survey rather than a face-to-face interview, and the elderly individuals might have had difficulty responding to the survey. Finally, a sample size of 300 participants is insufficient to represent the general Korean population.
In conclusion, we observed that the “anxiety-uncertaintydistancing” and “anxiety-dysfunctional beliefs about sleepdistancing” models are feasible in the elderly population. In addition, psychological inflexibility can be a variable which plays a role in these two models. Healthcare professionals should consider addressing these psychological factors when designing interventions to address social-distancing phobia in elderly populations in future pandemics.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
Seockhoon Chung, a contributing editor of the Psychiatry Investigation, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Author Contributions
Conceptualization: all authors. Data curation: Seockhoon Chung, Kayoung Song. Formal analysis: all authors. Methodology: all authors. Writing— original draft: all authors. Writing—review & editing: all authors.
Funding Statement
None