INTRODUCTION
With world population ageing, the prevalence of dementia will triple worldwide by 2050 [1]. Due to rapid increase in the prevalence of dementia, the social and financial burden on the caregivers and the community is growing out of proportion [2,3]. Vascular dementia (VaD) is the second leading cause of dementia worldwide [4,5]. Clinically, impaired judgment and impaired ability to make decisions, to plan or to organize are all early symptoms more likely to be associated with a diagnosis of VaD in the initial stages [6], while Alzheimer’s dementia (AD) manifests as memory loss, i.e., a gradual decline in the ability to remember new information [7]. Moreover, patients with mild VaD are likely to have more pronounced deficits in frontal functioning [8] and instrumental activities of daily living (ADL) than patients with mild AD [9].
Although the early detection and differential diagnosis of dementia is essential to make appropriate treatment strategies at the earliest stages, accurately identifying the underlying etiology of dementia remains challenging due to overlaps in symptomatology, pathophysiology, and comorbidity [10]. Further understanding the typical features of VaD and AD in terms of current cognitive function and ADL may enable clinicians to plan tailored treatment strategies, contributing to a positive outcome of each disease [11-13].
Clinical Dementia Rating (CDR) scale was originally developed to stage the severity of AD [14,15] but is now used globally in the initial evaluation of individuals with dementia regardless of types of dementia [16,17]. The pattern of CDR domains (CDR-Ds) could affect the physician’s diagnostic impression and the treatment strategies adopted, ultimately affecting the burden on the caregiver. Rosness et al. [18] found that the CDR may be used to differentiate frontotemporal dementia from AD. However, there is limited studies characterizing the clinical features of VaD and AD with using CDR scale.
The aim of this study was to investigate the characteristic pattern of CDR-Ds and its association with neuropsychological findings and ADL in patients with VaD and aged-matched patients with AD among the first visitors to a dementia clinic.
METHODS
All subjects were recruited from a dementia clinic, Jeju National University Hospital (JNUH), between July 2009 and June 2020. The subjects were the first consecutive visitors for the evaluation of dementia and had not suffered from major psychiatric illnesses including major depressive disorder, bipolar disorder, and schizophrenia before cognitive decline. The subjects had not taken or were not taking antidementia medications and antidepressants. All subjects were fully informed about the study protocol and written statements of informed consent were signed by either the subjects or their legal guardians. The Institutional Review Board of Jeju National University Hospital, Korea, approved this study protocol (JNUH 2021-03-014).
The subjects were assessed using the protocol of the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease assessment battery (CERAD-K) [19], which is composed of the standardized clinical interview, physical and neurological examinations, and laboratory tests including either the brain computerized tomography scan or magnetic resonance imaging. The modified Hachinski ischemic score [20] is included in CERAD-K. Depressive symptoms were evaluated using Korean version of the short form Geriatric Depression Scale [21]. For comprehensive neuropsychological assessments, the CERAD-K Neuropsychological Assessment Battery (CERAD-K-N), Stroop Color and Word Test [22], Frontal Assessment Battery (FAB) [23], and executive Clock Drawing Task (CLOX) [24] was administered by 3 neuropsychologists. The CERAD-K-N consists of categorical Verbal Fluency Test, 5-item Boston Naming Test (BNT), the Korean version of the Mini-Mental State Examination (MMSE), Word List Memory Test (WLMT), Constructional praxis Test, Word List Recall test (WLRT), Word List Recognition Test (WLRcT), Constructional Recall Test (CRT), and Trail Making Test A and B (TMB). TMB results were excluded from this study because the failure rate of performance on the TMB was extremely high at 87%. The basic and instrumental ADL of patients with dementia were evaluated by using Disability Assessment for Dementia (DAD) [25]. Lower scores indicate more dysfunction in DAD (maximum score: initiation 13, planning and organization 10, effective performance 17, total 40).
Subsequently, all available information was reviewed by a panel of 3 experienced dementia research neuropsychiatrists for the determination of the CDR index and diagnosis. Information relative to CDR-Ds was collected from both the collateral source and from the subjects. In assigning a global CDR and CDR sum of boxes (CDR-SOB), the six domains that are used to construct the overall CDR table are each scored individually. A global CDR rating of 0 signifies no dementia, a rating of 0.5 signifies very mild dementia, and ratings of 1, 2, and 3 signify mild, moderate, and severe dementia, respectively [26,27]. The six CDR-Ds are: memory (CDR D1), orientation (CDR D2), judgment (CDR D3), community affairs (CDR D4), hobbies (CDR D5), and personal care (CDR D6) [28]. Additionally, the CDR cognition (CDR-COG) was operationally defined as the sum of scores on CDR D1, D2, and D3. The CDR-ADL was obtained through the sum of scores on CDR D4, D5, and D6. Other factors, such as age, depression, or physical disability, that may affect the patients’ cognitive function, must be excluded at the time of CDR evaluation. Only the patients with global CDR of 0.5 and 1, suggesting very mild to mild severity of dementia, were included in this study.
VaD was diagnosed according to the National Institute of Neurological Disorders and Stroke/Association Internationale pour la Recherche et l’Enseignement en Neurosciences criteria (NINDS-AIREN) [29], and AD was diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association criteria (NINCDS-ADRDA) [30]. The patients with probable VaD or probable AD were enrolled in the study.
For the analyses of demographic characteristics, continuous variables were analyzed using the Student’s t-test and categorical variables were by using chi-squared test. As CDR scores were ordinal variables and were not normally distributed, we applied mainly nonparametric statistics in the analysis of CDR score. A Mann-Whitney U test was used to determine the significance of differences in scores of global CDR, CDR-SOB, CDR-COG, CDR-ADL, and CDR-Ds between patients with VaD and patients with AD. Friedman test was used to compares scores of CDR-Ds within the groups. Wilcoxon signed-rank test was used in post-hoc tests to examine significant differences between the scores of CDR-Ds within AD and VaD groups. Analysis of variance (ANOVA) after adjustment for sex and years of education was used to examine differences in scores of neuropsychological tests between the VaD and AD groups. For all the analyses, a two-tailed p-value of less than 0.05 was considered statistically significant. All the statistical analyses were performed using the Stata version 16.1 (Stata-Corp LLC, College Station, TX, USA).
RESULTS
One hundred and five pairs of VaD (75.59±5.38 years) and age-matched AD patients (75.93±5.33 years) were enrolled in this study (Table 1). The percentages of female with VaD and with AD were 49.5% and 71.4% (p=0.001, chi-square test). Levels of education (6.42±5.67 years in patients with VaD; 3.48±4.09 years in patients with AD) were different between the two groups (p<0.001, Student’s t-test). The proportion of very mild (CDR=0.5) dementias was higher in the patients with AD than in those with VaD (p<0.001, chi-square test). The difference of MMSE mean scores between two groups did not reach the statical significance (p=0.077, Student’s t-test) and additionally adjusted mean scores were very similar between two groups (p=0.843, ANOVA) after after adjustment for sex, age, and years of education, which were different demographic factors between two groups. As predicted, the mean modified Hachinski ischemic score was higher in the patients with VaD than in patients with AD (p<0.001, Student’s t-test). In the DAD scale, the scores for initiation, effective performance, and the total score are significantly lower in patients with VaD compared to those with AD (Table 1). A significant difference was detected in the CDR-SOB between patients with AD and patients with VaD (p<0.001, Student’s t-test; p<0.001, Mann-Whitney U test). The CDR-SOB mean scores in the 1st, 2nd, and 3rd quartiles of the MMSE scores distribution were higher in patients with VaD than in patients with AD (p=0.001, p<0.001, p<0.001, Mann-Whitney U test) but that of 4th quartile did not reach the statistical significance (p=0.137, Mann-Whitney U test) (Figure 1). The mean total score of DAD was lower in VaD patients than in AD patients (p<0.001, Student’s t-test; p< 0.001, ANOVA adjusted for sex and years of education), indicating greater functional impairment in VaD patients.
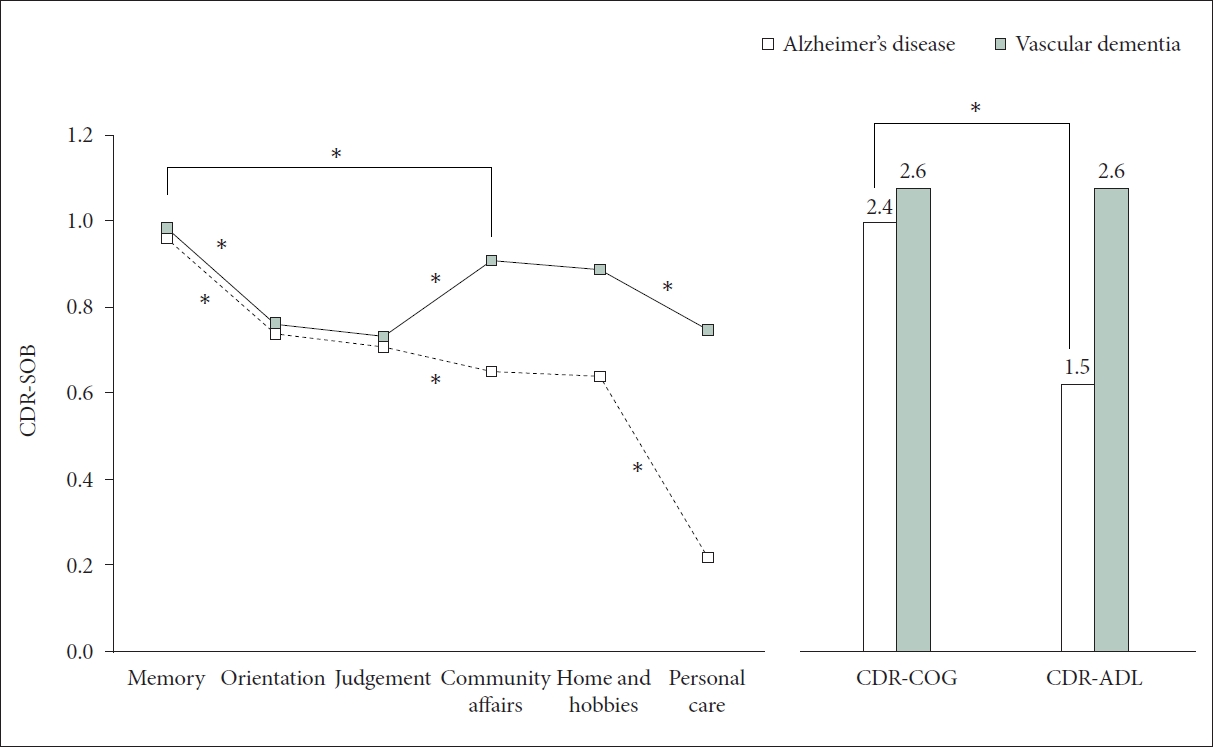
The mean scores on global CDR, CDR-SOB, CDR-D4, D5, D6, and CDR-ADL were higher in patients with VaD than in patients with AD (p<0.001, Mann-Whitney U test), while those of CDR-D1, D2, and D3, CDR-COG were not different (p=0.722, p=0.391, p=0.170, p=-0.313, Mann-Whitney U test) between the two groups (Table 2 and Figure 2). Within patients with VaD, the means of CDR-Ds decreased in the order of CDR-D1, D4, D5, D6, D2, and D3 (p<0.001, Friedman test; CDR-D1>D4, D5>D6, D2, D3, Wilcoxon signed-rank test for post-hoc). Within the AD patient, the means of CDR-Ds consecutively decreased from CDR-D1 to D6 (p<0.001, Friedman test; CDR-D1>D2, D3>D4, D5>D6, Wilcoxon signed-rank test for post-hoc). The differences of means between CDR-COG and CDR-ADL were significant within AD patients (p<0.001, Wilcoxon signed-rank test), not within VaD patients (p=0.736, Wilcoxon signed-rank test) (Figure 2).
Patients with VaD showed better performances on BNT (p=0.028), WLMT (p<0.001), WLRT (p<0.001), WLRcT (p=0.018), and CRT (p=0.007), but showed poor performances on FAB (p=0.009), CLOX1 (p=0.018), Stoop Word test (p<0.001), Stoop Color test (p<0.001), and Stoop Color-Word test (p=0.037) than age-matched patients with AD after adjustment for sex and years education (Table 3).
DISCUSSION
This study investigated the characteristic pattern of CDR-Ds in patients with VaD in comparison with age-matched patients with AD. With the progression of dementia, the cognitive dysfunction and functional disabilities develop comprehensively in both VaD and AD, and clinical features of VaD and AD become similar in advanced stages of dementia [31,32]. Therefore, we included only patients with very mild to mild dementia in this study.
In general, as VaD has an earlier onset and its prevalence is less associated with increasing age in comparison with AD, the mean age of patients with VaD is lower than that of AD [33,34]. Therefore, we matched subjects with respect to age, which is a potential risk factor affecting cognitive function and disability, to increase the comparability between VaD and AD. In this study, patients with VaD were more educated and included fewer female participants, compared with patients with AD in accordance with previous studies [35,36]. As women have a higher risk of AD than men, but no increased vulnerability to VaD [35]. A higher prevalence of AD is associated with low levels of education, while VaD is not associated with the level of education [36].
The CDR scale is widely used in the initial evaluation of dementia, regardless of types of dementia [16,17]. The CDR rates only impairment caused by cognitive loss rather than by physical disability and other noncognitive factors. Validity and reliability of the CDR are excellent (93% diagnostic accuracy) [37,38]. The determination of the CDR requires an extended time to conduct interviews. For this reason, the CDR is not suitable as a brief screening tool but the process of collecting information relative to CDR-Ds and rating CDR-Ds with using a semi-structured interview is practically equal to the clinical history taking for diagnosis of dementia. The CDR-Ds are less influenced by the “floor” and “ceiling” effect associated with other psychometric test0s [39].
Although all subjects were recruited among the first visitors for the evaluation of dementia and the adjusted mean scores of MMSE were similar between VaD and age-matched AD patients, the scores on the global CDR and CDR-SOB were higher (p<0.001, Mann-Whitney U test) and the proportion of global CDR 1 to global CDR 0.5 was higher in VaD patients than in AD. The differences in the scores on global CDR and CDR-SOB are mainly attributable to higher scores on CDR-D4, D5, D6, and CDR-ADL, indicating more impairment of ADL in patients with VaD. The greater impairment in ADL among patients with VaD was confirmed through lower sub-scores in initiation and effective performance, as well as a lower total score on the DAD scale, indicating more significant functional impairment in ADL. However, there was no significant difference in planning and organization between the two groups. The scores of CDR-D1, D2, D3, and CDR-COG, the CDR-Ds reflecting cognitive function, were not different between two groups. VaD patients are in more severe stages of dementia than those with AD mainly due to more impaired ADL.
Why does patients with VaD show more impaired ADL than patients with AD, despite similar adjusted MMSE score and better performances on episodic memory, visual memory, and confrontational naming test? The question can be answered in two ways. First, patients with VaD present greater impairment in executive function than patients with AD. Poor performances on FAB, CLOX1, and Stroop tests in patient with VaD, which was applied to assess executive function in this study, were consistently confirmed. The difference in CDR patterns may be interpreted as being indicative of the different pathology between VaD and AD. VaD pathology frequently entails predominant deficits in attention, information processing, and executive function [40,41]. Recent studies [42-44] have consistently demonstrated that patients with VaD are more impaired than those with AD on tests of executive functions. Several studies [45,46], applying standard neuropsychological tests of executive function, have shown robust links between executive dysfunction and impairments in daily functioning such as cooking, dressing, shopping, and housework [47], which correlate with the community affairs, home and hobbies, and personal care domains of CDR. Executive function and daily living activity are more preserved in mild AD than in mild VaD [8,9]. Second, the raters of CDR may be influenced by the impairments due to other medical conditions such as physical handicap or depression. Sometimes, it is difficult to distinguish the declines in ADL attributable to cognitive decline from those attributable to combined medical conditions. There is a possibility that combined physical disabilities in patients with VaD may partly cause ADL-related domains to be over-rated in patients with VaD.
There were typical patterns of CDR-Ds within patients with very mild to mild VaD or AD. Patients with VaD have similar severities between ADL-related CDR-Ds and cognition-related CDR-Ds while in those with AD, cognition-related CDR-Ds were severer than ADL-related CDR-Ds. In the assessment of new visitors to a dementia clinic, recognizing these characteristic CDR patterns is clinically beneficial for distinguishing between VaD and AD. Additionally, it is advantageous to create a personalized care plan that considers both cognition-related CDR-Ds and ADL-related CDR-Ds. For patients with VaD, it becomes crucial to prioritize care plans that specifically target and address issues related to reduced initiation and less effective performance in executive functions.
There are some strengths in this study. First, this study is the first study to investigate the characteristic pattern of CDR in very mild to mild VaD compared with age-matched AD with relatively large sample. Second, we matched subjects with respect to age, to increase the comparability between VaD and AD. There are also several limitations to the present study. First, there was the demographic differences in education level and proportion of female between the patients with VaD and agematched AD. However, all these factors were adjusted for in the statistical analysis in the present study. Second, all the subjects were recruited in only one dementia clinic. There may be a selection bias that in clinical setting, subjects with more severe dementia tend to be enrolled than in community sample. Further studies using community sample will make clear the difference of CDR patterns between AD and VaD.
In conclusion, the severity and pattern of CDR-Ds are different between patients with very mild to mild VaD and agematched AD. Despite similar general cognitive function and better memory function, patients with VaD tend to be staged as severer dementia on CDR scale than age-matched patients with AD because of more impaired ADL associated with executive dysfunction in VaD patients.