INTRODUCTION
Schizophrenia is a chronic and serious mental disorder, affecting nearly one percent of people globally (more than 24 million people) [1]. Although the prevalence of schizophrenia seems roughly similar across jurisdictions, the age-standardized statistics indicate that Asian countries with lower prevalence and regions, such as the Middle East and East Asia, experience more negative impacts based on disability-adjusted life years [2,3]. A study assessing the prevalence of schizophrenia in China from 1990 to 2010 found a growing number of affected people during this period, growing from 3.09 million to 7.16 million, reflecting a 132% increase [4]. According to the National Health Insurance dataset, the cumulative prevalence rate was 6.42 per 1,000 persons in Taiwan in 2001 [5].
Schizophrenia as a long-term disability is characterized by impairments in thoughts, emotions, behaviors, and cognitive functions. Many affected individuals experience occupational and/or marital concerns [6]. Therefore, social problems, including social relationship and networking impairments, are common [7]. The World Health Organization has listed five important consequence of schizophrenia (i.e., mortality, social stigma, social cost, impact on caregivers, and social isolation), with social concerns being prominent [1].
Approximately one-third to two-thirds of individuals with mental disorders, like their unaffected peers, use social media to make friends, share information, and receive social contacts [8,9]. Affected individuals may also use social media to experience support and find treatments for their conditions of mental well-being and psychological symptoms [10]. Studies from 2008 to 2020 indicate an increasing rate (by about 50%) of internet use in people with psychiatric concerns. Social media may be perceived as a non-threatening space with less associated stress and anxiety for people with mental illness to interact socially [11-13]. Therefore, people with schizophrenia may engage in social media to be socially active, and such media may also be used to connect clinicians and patients to monitor clinical status and provide therapeutic consolations [8,10]. However, use of social media may also expose people with schizophrenia to potential risks such as worsening of symptoms, unwanted or impulsive disclosures, lost privacy and confidentiality, and possibly internet addiction and stigmatization [14].
Problematic use of social media (PUSM) use refers to the potential negative impacts of using internet platforms (i.e., social media like Facebook) for connecting with other people, with the level of engagement linked to addiction-like symptoms, mood fluctuations, preoccupation, psychological or functional impairments, and tolerance [15]. A review of potential risks and benefits of use of social media by people with schizophrenia suggested widespread use; however, less is known regarding the clinical risks or benefits of such growing usage [14]. Data suggest potential negative impacts of PUSM as one form of problematic use of the internet in people with schizophrenia [8]. Problematic use of internet has been correlated with psychotic-like experiences, suggesting possible similar experiences in people with schizophrenia [10,14]. Particular situations like lockdowns during the coronavirus disease-2019 (COVID-19) pandemic may have intensified use of the internet and social media both among the general population and people with schizophrenia, with possible particular negative influences on the clinical conditions of the latter group [16]. However, internet addiction and PUSM should be considered as different kinds of addiction-like behaviors because despite associations between these two phenomena (both use online connections), they may have unique attributes and uses that may differentiate them. Indeed, internet addiction may mostly occur when people become preoccupied excessively with and experience diminished control over internet use for different aims including education, communication, entertainment, and other purposes, whereas in PUSM, excessive use of electronic devices (and perhaps particularly cell-phones) may occur basically with the goal of social communications [17].
The impact of PUSM on quality of life (QoL) has been investigated in different populations. For example, more time spent on social media may limit adolescents from spending sufficient time engaging in physical activity and social relationships in non-virtual settings, and this may lead to decreased well-being and QoL [18]. In a recent cross-sectional study, the association between PUSM and QoL and mental health disorders among adolescents in Hong Kong revealed that those who used social media for less than three hours daily had better QoL and fewer mental health problems including anxiety and depression than those with PUSM [19]. Negative impacts of PUSM on QoL in other populations have also been documented [20]. Given that QoL in people with schizophrenia is often worse than that in healthy individuals and those with other health conditions, further assessments between the PUSM and QoL are required.
Sleep quality is also important to the well-being of people with schizophrenia [21]. Sleep disturbances are among the most prevalent problems experienced by people with schizophrenia, with approximately 30% to 80% of individuals experiencing sleep disturbances [22]. Poor sleep quality may not only reduce cognitive functioning, but also trigger psychotic symptoms that in turn may decrease QoL [23]. Among Chinese people with schizophrenia, about one-third reported sleep disturbances and insomnia, and sleep problems were associated with low QoL [24]. Studies of QoL and sleep problems in individuals with mental disorders including schizophrenia have found negative relationships between these domains [24-26]. PUSM may influence sleep quality in the general population and also in people with mental disorders [27,28]. However, less is known regarding how sleep quality may operate to influence QoL in people with schizophrenia.
Self-stigmatization is common among people with schizophrenia, and its associations with PUSM and QoL in people with psychological problems have been investigated [29,30]. Self-stigma is related to shame regarding individual differences, and people with mental illnesses may accept and internalize negative stereotypes [31]. Internalized self-stigma may act as a negative mental habit and negatively impact life satisfaction and QoL in response to feelings of discrimination [29]. People with schizophrenia often experience self-stigma during the course of treatment, and their social interactions may lead to low self-esteem, depression and feelings of hopelessness that may have detrimental impacts on QoL [32,33]. Self-stigma may moderate relationships between social functioning, self-efficacy and hope in people with schizophrenia [34,35]. However, a mediating role for self-stigma between PUSM and QoL has not been investigated in this population.
Data suggest that PUSM, QoL, sleep quality, and self-stigma in people with schizophrenia may be interrelated. A better understanding of mechanisms underlying relationships between PUSM and QoL would be helpful to reduce the negative impact of PUSM and improve the QoL among people with schizophrenia. Identifying possible roles for modifiable risk factors (e.g., sleep disturbances and self-stigma) may help with intervention development. Therefore, a conceptual model for this study is shown in Figure 1. We hypothesize there may be indirect associations between PUSM and QoL that may be explained through self-stigma and sleep quality. Identifying whether such relationships exist may help find pathways through which interventions may be developed to decrease negative effects of PUSM on QoL in people with schizophrenia. The current study hypothesized that sleep quality and self-stigma may operate as mechanisms linking PUSM and poor QoL in this population. Thus, the aims of this study involved: 1) assessing measures of PUSM, QoL, sleep quality, and self-stigma; 2) identifying temporal relationships between these variables; and 3) investigating potentially mediating effects of sleep quality and self-stigma on associations between PUSM and QoL over a 1-year follow-up.
METHODS
Participants and recruitment process
The present study was approved by the Institutional Review Board of the Jianan Psychiatric Center (IRB ref: 18-039 & 19-034), and the sample has been described in detail previously [36]. In brief, the present study’s participants were treated in day and outpatient treatment programs at the Jianan Psychiatric Center (JPC) in Tainan, Taiwan. The JPC is the largest national psychiatric center in Southern Taiwan and provides multiple psychiatric services [37]. The present sample was recruited under the supervision of trained research assistants between April 30, 2019 and August 6, 2021. Inclusion criteria were 1) having a diagnosis of schizophrenia based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria (American Psychiatric Association, 2013); 2) possessing a smartphone during the study period; and 3) being an adult (i.e., aged 20 years or above according to the Civil Law definition in Taiwan). All participants provided written informed consent prior to the study and completed the survey five times (12-month period at 3-month intervals [0, 3, 6, 9, and 12 months]). The present study applied convenience sampling for recruitment and aimed to recruit at least 100 participants at the final follow-up according to the ratio of 10 participants per variable. Because the model planned in the present study included 10 variables, more than 100 participants were recruited for study. At baseline, 193 participants were recruited, with 103 participants at the final follow-up. Missing values were checked for randomness, and data were missing completely at random based on Little’s Missing Completely At Random test [36,38].
Measures
Demographics
The present sample’s demographics included 1) age (reported in years); 2) sex (male or female); 3) marital status (single, married, or other); 4) years of education; and 5) physical disease (yes or no).
QoL
Participants’ QoL was assessed using the World Health Organization Quality of Life Questionnaire Brief Version (WHOQOL-BREF), a self-reported instrument with 28 items in its Taiwanese version [39-41]. Among the 28 items, 26 were distributed into four QoL domains: physical (seven items), psychological (six items), social (four items), and environmental (nine items). The remaining two items assess general QoL and over health. Two WHOQOL-BREF items were not distributed into any QoL domain because they are general items asking overall QoL (item 1) and general health (item 2) [42,43]. Therefore, the two general items were not used in analyses. All items were rated on a 5-point Likert scale. After reverse coding three negatively worded items and converting the item scores into domain scores (ranging between 4 and 20 for each domain), summed scores were generated, with higher scores reflecting better QoL [44]. The WHOQOL-BREF has been validated in Chinese, with Cronbach’s α values ranging from 0.73 to 0.83 [45,46].
Sleep quality
Participants’ sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a self-reported instrument with 19 items [47]. Answers were converted into seven component scores (each component score ranging between 0 and 3). Summed component scores (ranging between 0 and 21) were generated, with higher scores reflecting poorer sleep quality [36,48,49]. The PSQI has been validated in Chinese, with a Cronbach’s α of 0.83 [50].
Self-stigma
Participants’ self-stigma was assessed using the Self-Stigma Scale-Short (SSS-S), a self-report instrument with nine items [51]. The SSS-S was developed within a cognitive-behavioral theorical framework. All items were rated on a 4-point Likert scale, with each item score ranging between 1 and 4. The nine SSS-S item scores were calculated using a mean score (i.e., summing the nine SSS-S item scores and then dividing by nine), with higher SSS-S scores reflecting higher levels of self-stigma [52-55]. The SSS-S has been validated in Chinese, with Cronbach’s α values ranging from 0.80 to 0.91 [56,57].
PUSM
Participants’ PUSM was assessed using the Bergen Social Media Addiction Scale (BSMAS), a self-report instrument with six items [58]. The BSMAS was developed within the framework of Griffiths’ [59] components model of addiction. All items were rated on a 5-point Likert scale (each item score ranging between 1 and 5). The six BSMAS item scores were summed, with higher BSMAS scores reflecting higher levels of PUSM [60-65]. The BSMAS has been validated in Chinese, with Cronbach’s α values ranging from 0.73 to 0.82 [66-68].
Data analysis
Participants’ characteristics and measure scores at baseline were analyzed using descriptive statistics, including means (standard deviations [SDs]) and frequencies (percentages). Next, six general estimating equation (GEE) models were constructed to understand temporal associations between variables. All GEE models utilized a random effect of time (i.e., the repeated measures of the mediators or outcome variables) and shared potential confounding variables of sex (reference group of male), age, marital status (reference group of single), years of education, and physical disease (reference group of yes). For the GEE models using sleep quality and self-stigma as dependent variables, PUSM was treated as the independent variable to assess associations with consideration of repeated measures. For the GEE models using QoL measures as dependent variables (i.e., physical, psychological, social, and environmental QoL), sleep quality and self-stigma were included as independent variables.
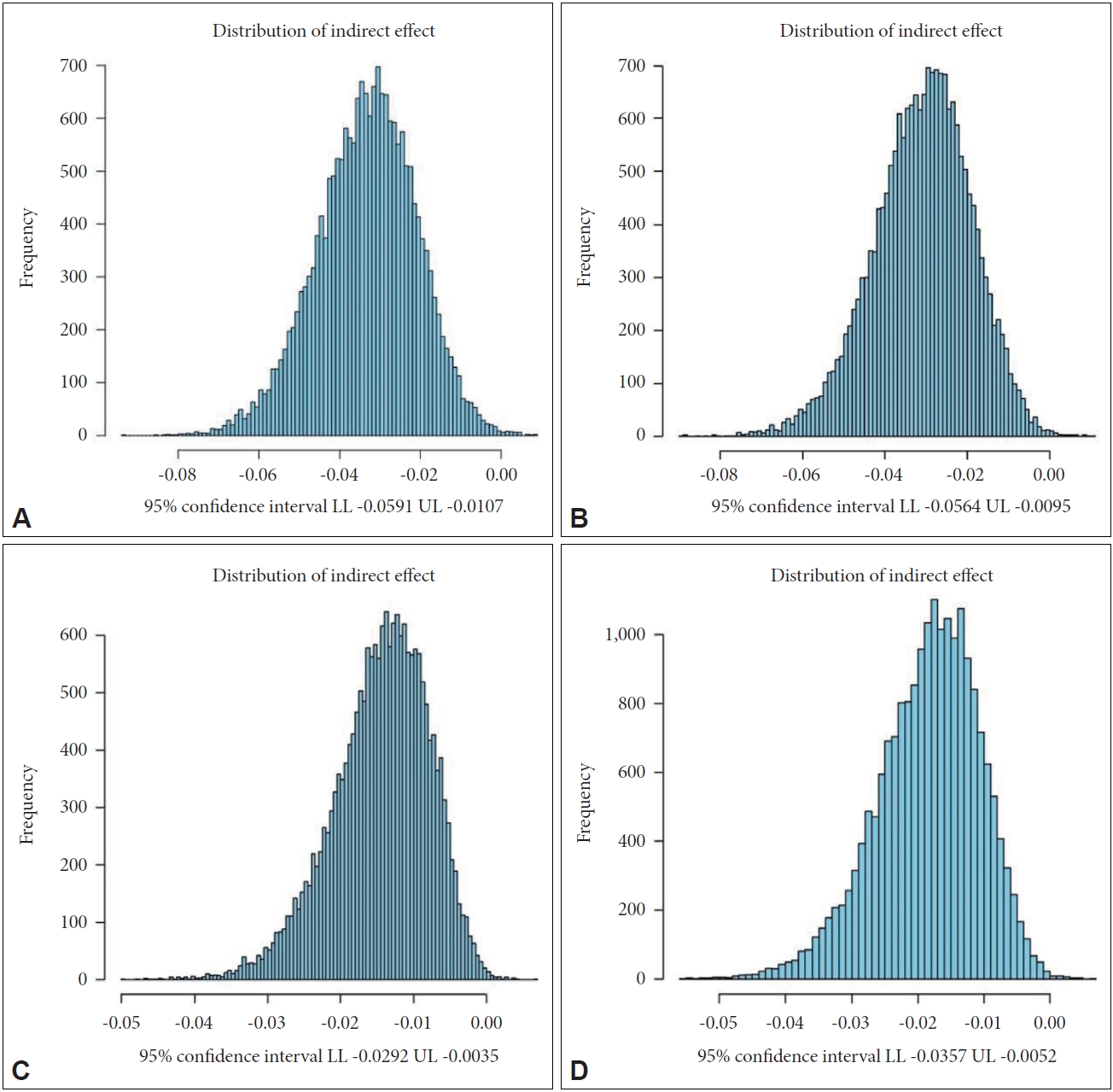
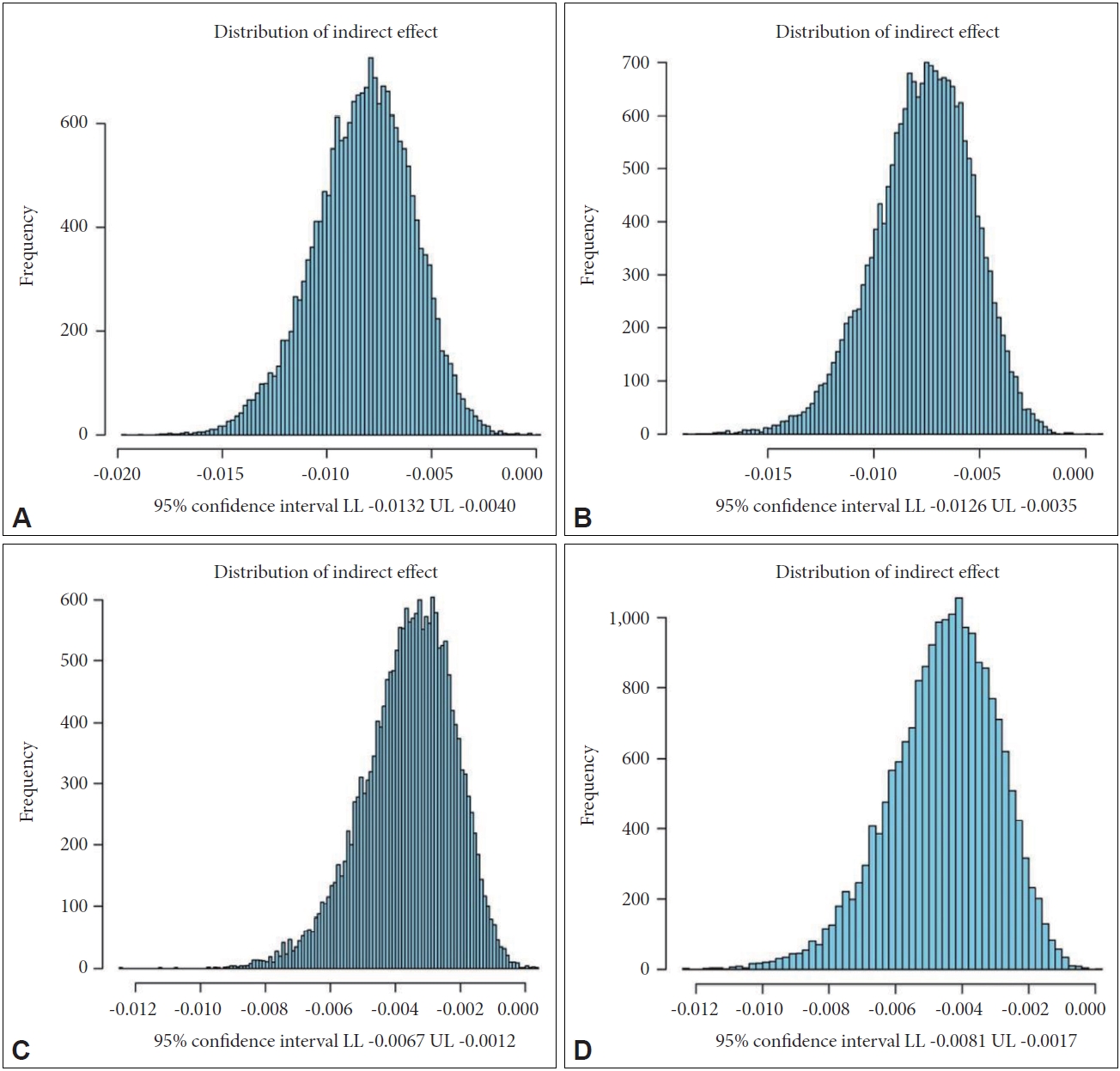
To examine potential mediating effects of sleep quality and self-stigma in the associations between PUSM and QoL, a Monte Carlo method was used [69,70]. Specifically, coefficients and standard errors (SE) derived from every two GEE models were used in R software to generate Monte Carlo simulations with 20,000 repetitions (http://quantpsy.org/medmc/medmc.htm). In the 20,000 repetitions, 95% confidence intervals (CIs) were calculated for the association. For example, the statistical procedures were 1) retrieving the coefficient and SE of sleep quality in the GEE model with physical QoL as an outcome variable; 2) retrieving the coefficient and SE of PUSM in the GEE model with sleep quality as an outcome variable; and 3) calculating the 20,000 repetitions to test whether sleep quality mediated the association between PUSM and physical QoL. A mediation is supported when the 95% CI does not include 0 [69]. Apart from mediating effects, all statistical analyses were performed using IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The present sample (n=193; mean age=41.34±9.01 years) consisted of more females (n=105; 54.4%) than males. Over half of the sample was single (n=122; 63.2%), and less than one-third of participants had a physical disease (n=62; 32.1%). On average, participants reported 12.14 (SD=2.58) years of education. Participants’ QoL, sleep quality, self-stigma, and PUSM are reported in Table 1.
The GEE models (Table 2) showed that PUSM was not a significant factor directly explaining any of the QoL domains: coefficient (SE/p-value)=0.02 (0.03/0.61) for physical QoL; -0.01 (0.03/0.72) for psychological QoL; -0.001 (0.03/0.98) for social QoL; and 0.01 (0.03/0.81) for environmental QoL. However, both sleep quality (coefficients=-0.12 to -0.27; p<0.001) and self-stigma (coefficients=-0.92 to -1.42; p<0.001) were significant factors related to QoL. Additionally, PUSM was found to be a significant factor relating to both sleep quality (coefficient=0.12; SE=0.04; p=0.003) and self-stigma (coefficient= 0.03; SE=0.008; p<0.001).
The Monte Carlo method additionally showed that sleep quality and self-stigma were significant mediators in the association between PUSM and QoL. For the mediator of sleep quality, the 95% CIs for indirect effects ranged from -0.0591 to -0.0107 for physical QoL; -0.0564 to -0.0095 for psychological QoL; -0.0292 to -0.0035 for social QoL; and -0.0357 to -0.0052 for environmental QoL (Figure 2). For the mediator of self-stigma, the 95% CIs for indirect effects ranged from -0.0132 to -0.0040 for physical QoL; -0.0126 to -0.0035 for psychological QoL; -0.0067 to -0.0012 for social QoL; and -0.0081 to -0.0017 for environmental QoL (Figure 3).
DISCUSSION
The current study investigated associations between PUSM, QoL, self-stigma, and sleep quality among people with schizophrenia, with a specific goal of examining how sleep quality and self-stigma may mediate relationships between PUSM and QoL over time. We sought to identify new pathways between PUSM and QoL to consider how potential interventions may address negative impacts of the former on the latter. Our findings indicated that although there were not significant direct effects of PUSM on QoL, sleep quality and self-stigma accounted for indirect effects between these domains, suggesting possible mechanisms by which PUSM may operate to reduce QoL in people with schizophrenia.
Although this was not an epidemiological study, the sample characteristics were similar to those from other cross-sectional studies. For example, in a study on a multicenter sample of people with schizophrenia, Xiang et al. [71] reported more than half of their sample was unmarried with a mean education of 12.2±2.3 years, with a mean age of 32.6±10.8 years. They also found that factors such as stable marriages and lower educational attainment may be common in people with schizophrenia, and this may negatively impact QoL. Similarly, the average scores of measures assessing QoL, sleep quality, and self-stigma reported here were comparable with those from other studies of people with schizophrenia [7,25,32,34,35], and these findings suggest a need for designing health-promoting interventions addressing these domains.
Unlike previous studies that have reported significant associations between PUSM and QoL in general populations, particularly among youth [19,72], we did not observe significant direct associations between these two domains in our sample. Several possibilities exist. First, using social media may have positive impacts, particularly for improving social communication in people with schizophrenia who may have limited in-person, face-to-face social interactions; this may have been particularly relevant during the COVID-19 pandemic when some data were collected [10,14]. Therefore, direct associations between these two variables may not have been observed despite expectations. Second, we used statistical methods based on temporal associations between the variables longitudinally that may provide a more concise estimation than those conducted in cross-sectional studies. Thus, we examined associations between these variables through sleep quality and selfstigma in mediation models. Third, using GEE models may lead to different results than those that may be observed in bivariate correlations. Indeed, we employed this method to provide a more comprehensive approach to understanding how specific variables may influence QoL instead of conducting correlations between paired variables. Finally, demographic characteristics of our sample differ from several previous studies [19,72]. While those focused on the adolescents and young adult populations, our sample included people with an average age of 40 years, and age should be considered as possibly modifying effects of PUSM on QoL.
As we found, there were significant associations between PUSM (as the independent variable) and self-stigma and sleep quality (as mediators). Such relationships have been identified in prior studies of other populations. However, a main point here involves which mechanisms may underlie these associations. A likely explanation for the association between PUSM and self-stigma may be related to situations in which people receive more information or feedback regarding their conditions (specifically here schizophrenia), this process may lead to comparisons between their current situations and the situations of healthy people that may promote self-stigmatization due to recognizing limitations related to the disorders. Indeed, when people communicate through social media excessively, this may increase their sensitivity concerning their condition and consequently generate self-stigma. In a similar manner, people who engage in social media beyond normal usage (i.e., those with PUSM), may experience disruptions in their circadian rhythms, leading to sleep disturbances. For example, individuals may devote time intended for sleep to excessive use of social media. Consistent with this notion, associations between PUSM and low sleep quality have been shown in several studies [18,27,28].
The associations between sleep quality and QoL among people with schizophrenia have been assessed in several studies [25,26]. Among 207 people with schizophrenia, Wang et al. [25] found a mean score of 6.14±2.94 for the PSQI, with 58% experiencing sleep disturbances. The mean score for this variable in our study was higher than in that study, and this may be attributed to differences in the inclusion criteria for the two studies. Wang et al. [25] enrolled only clinically stable people, whereas we included all people with a schizophrenia diagnosis. They also found a significant difference in QoL between men and women, with men having better QoL than women. However, in our sample we did not find such a difference. This may be related to different scales used to measure QoL (Schizophrenia Quality of Life Scale vs. WHOQOL-BREF), different analytical approaches (logistic regression vs. GEE), and/or different sample characteristics and sizes (n=207 vs. 193 at baseline that reduced to 103 at the last follow-up). Among 623 Chinese people with schizophrenia recruited from different primary care centers, Hou et al. [26] found serious sleep disturbances among the sample that may have negatively impacted their QoL, consistent with our findings.
Mosanya et al. [32] studied relationships between self-stigma and QoL among 156 outpatients with schizophrenia. They also found significant associations between self-stigma and poor QoL. Another study conducted in China found that people with schizophrenia were commonly at risk of self-stigmatization and this may not only affect subjective QoL, but also negatively impact physical QoL, as we found here [34].
To the best of our knowledge, this is the first study conducted to assess how sleep quality and self-stigma may serve as mechanisms relating PUSM to poorer QoL over time in people with schizophrenia. The temporal association models reflect novelty and provide directional insights. However, there are some limitations that should be noted. First, as we recruited our sample from only one medical center in Taiwan, generalizability of the findings is limited. Indeed, the literature suggests that the incidence of schizophrenia is higher in males than in females [73]; however, the present study included a relatively higher proportion of females (54.4% females vs. 45.6% males). Second, our study was conducted during the COVID-19 pandemic, and the related lockdowns may have intensified particular problems such as sleep disturbances and PUSM or may have mitigated some of the negative effects of PUSM. Additional studies under more “normal” conditions are warranted. Third, we experienced considerable attrition in our sample over time, and this may have affected our findings. However, we used robust statistical techniques to mitigate negative effects of attrition in as much as possible. Fourth, we controlled some variables including sex, marital status, and education level in our analyses. However, other variables that may influence associations between independent and dependent variables, such as severity of mental symptoms, were not collected and should be considered in future studies. Fifth, the present sample size was relatively small for conducting latent models (e.g., structural equation modeling). Therefore, the present study used GEE models to simplify the statistical analysis and to satisfy the principal of parsimony. Nevertheless, future studies may recruit larger samples to investigate latent models. Finally, the measurement of sleep in the present study (i.e., the PSQI) was subjective. With the use of objective measures of participants’ sleep (e.g., physiological measures assessing sleep quality such as sleep onset and sleep efficiency) may provide additional information via less biased measures to examine the phenomenon investigated in the present study.
In conclusion, the study’s findings suggest mediating roles for both sleep quality and self-stigma in the associations between PUSM and QoL in people with schizophrenia. Therefore, developing interventions to target sleep and self-stigma may reduce not only direct negative impacts on QoL in people with schizophrenia, but also indirect effects of PUSM. Further studies into other possible psychological concerns such as self-concept and self-esteem that may potentially also negatively affect QoL are needed. Such investigations may help further improve our understanding of mental health concerns in people with schizophrenia.