INTRODUCTION
Alzheimer’s disease (AD) is the most common cause of dementia. Nevertheless, the underlying mechanisms and pathophysiology of AD are not fully understood, and there is currently no effective treatment for AD [1]. Regarding the disappointing outcome of the disease-modifying trials of AD [2-4], researchers have pointed out that mixed pathology of amyloid pathology, vascular pathology, tau pathology, and/or alpha-synuclein pathology may be a possible cause [5,6].
Recent studies have shown that cortical amyloid burden, a hallmark of AD, frequently occurs alongside chronic cerebrovascular disease (CVD), such as white matter hyperintensities (WMH), lacunar infarction, and/or microbleeds in patients with cognitive decline [7,8]. Recent studies suggest that progressive cognitive decline can be driven by amyloid burden or vascular burden alone but can also be driven by the presence of both pathologies and their synergistic effects on neurodegeneration [9-12]. In this context, the cortical amyloid burden and vascular burden caused by chronic CVD have become important research goals over the last decade. Given the above, the Biobank Innovations for Chronic Cerebrovascular Disease with ALZheimer’s Disease Study (BICWALZS) was planned and initiated in 2016 by the Korea Disease Control and Prevention Agency for the Korea Biobank Project. The BICWALZS is a multi-center collaborative research project with five clinical centers, a regional biobank, and the National Biobank of Korea.
The original goal of BICWALZS was to facilitate, regulate, and ensure optimal research use of human biospecimens and data in the field of AD, chronic CVD, and mixed pathology for mild cognitive impairment (MCI) and dementia. Considering the multifactorial nature of neurodegenerative disorders and their heterogeneous clinical presentation, it is essential to assess not only clinical characteristics but also various biomarkers such as neuroimaging results, genomics data using single nucleotide polymorphism microarray chips, and actigraphy measurements [13]. In addition, considering its potential for the generation of induced pluripotent stem cells, possible ex vivo research, and precision medicine, we also sampled patient-derived dermal fibroblast in a subset of participants [14,15].
This paper reports the study design, methodology, and baseline clinical and biomarker characteristics of BICWALZS.
METHODS
Participants
BICWALZS was planned and initiated in October 2016 by the Korea Disease Control and Prevention Agency for the Korea Biobank Project which is a national innovative biobanking program to foster biomedical and healthcare R&D infrastructure. A total of five institutions participated: Ajou University Hospital, Samsung Medical Center, Inha University Hospital, Pusan National University Hospital, and Chonnam National University Hospital. The multi-site infrastructure is linked to a centralized coordinator center and database. A coordinating committee is in place to harmonize and standardize specimen handling, technical best practices, data entry, management, and ethical and legal issues. A total of 1013 participants were enrolled in the BICWALS from October 2016 to December 2020. All participants underwent clinical assessments, blood tests, and standardized neuropsychological tests (n=1,013). From the subset of the participants, we performed brain magnetic resonance imaging (MRI, n=817), brain amyloid positron emission tomography (PET, n=713), single nucleotide polymorphism microarray chip (n=949), actigraphy measurement (n=200), and patient-derived dermal fibroblast sampling (n=175). We planned to follow all participants annually with brief assessments and participants who had cortical amyloid burden, subcortical vascular pathology, apolipoprotein E4 allele, or significant cognitive decline biannually with an expanded assessment including neuropsychological tests, actigraphy measurements, and brain MRI. We first classified the participants according to their clinical diagnosis. The subjective cognitive decline (SCD) criteria included self and/or informant reports of cognitive decline but no impairment in objective cognitive tests and daily functioning. Participants with MCI were evaluated using the expanded Mayo Clinic criteria [16]. Participants with Alzheimer’s dementia met the core clinical criteria suggested by the National Institute on Aging and the Alzheimer’s Association working group in 2011 [17]. Participants with vascular dementia were evaluated using major vascular neurocognitive disorder criteria, as suggested in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders [18]. Additionally, for the neuroimaging-based approach and our study purpose, we classified a subset of participants into CN, ADCI, or VCI based on the mini-mental state examination (MMSE) and two critical neuroimaging biomarkers, cortical amyloid burden and subcortical vascular burden. For this process, age, sex, and education matched -1, or lower z-scores were considered cognitive decline. As a result, participants with amnestic MCI or AD were considered to have ADCI. Participants with possible other vascular pathologies, such as severe white matter intensities, were excluded from the ADCI group. Participants with subcortical vascular MCI or subcortical vascular dementia were considered to have an VCI. Participants with cortical amyloid pathology on amyloid PET or those with infarctions or WMH due to radiation injury, multiple sclerosis, vasculitis, or leukodystrophy were excluded from CN and VCI group.
BICWALZS is registered in the Korean National Clinical Trial Registry CRIS (identifier: KCT0003391). Prior to beginning the study, the Institutional Review Board approved the study plan (AJIRB-BMR-SUR-16-362). Written informed consent was obtained from all participants and caregivers. The study was conducted in accordance with the International Harmonization Conference guidelines on Good Clinical Practice.
Neuropsychological test
Cognitive function was evaluated using a standardized neuropsychological test, Seoul neuropsychological screening battery (SNSB) [19]. The SNSB includes tests of language, visuospatial, memory, and frontal/executive functions. General cognition was evaluated using the MMSE. Dementia severity was measured using a global deterioration scale (GDS). Attention ability was evaluated using the digit span test (DST). Language function was based on the Korean version of the Boston naming test (K-BNT). Visuospatial function was based on the Rey complex figure test (RCFT) copy score. Verbal memory function was evaluated using the Seoul verbal learning test (SVLT) immediate recall, delayed recall, and recognition score. Visuospatial memory function was evaluated using the RCFT immediate recall, delayed recall, and recognition score. The frontal/executive function was calculated using the controlled oral word association test (COWAT) and Stroop test. Additionally, depressive symptoms and instrumental activities of daily living were evaluated using the Korean version of the short form geriatric depression scale and Seoul instrumental activity of daily living (S-IADL).
Amyloid PET acquisition and measurement of amyloid deposition
Participants underwent 18F-flutemetamol PET scans using a Discovery Ste/690 PET/CT scanner (GE, Milwaukee, WI, USA) with an identical protocol. 18F-flutemetamol was injected into the antecubital vein as a bolus with a mean dose of 185 MBq. After 90 min, a 20 min PET scan (4×5 min dynamic frames) was performed. 18F-flutemetamol PET scans were co-registered to individual MRI scans, which were normalized to a T1-weighted MRI template. Using transformation parameters, MRI co-registered 18F-flutemetamol PET images were normalized to the MRI template. To quantify 18F-flutemetamol retention, the standard uptake value ratio (SUVR) was obtained using the pons as a reference region. Global cortical 18F-flutemetamol retention was calculated from the volume-weighted average SUVR of bilateral ten cortical volumes of interest from the frontal, posterior cingulate, lateral temporal, parietal, and occipital lobes using the annotated anatomical labeling atlas [20]. Based on a previous report on the elderly Korean population and our observed data distribution, participants were considered to be positive for amyloid if their global cortical SUVR was greater than 0.634 [21]. Alternatively, we also evaluated amyloid positivity by a visual rating of experienced nuclear medicine specialists who were blinded to the clinical information of the participants.
MRI acquisition and measurement of neurodegeneration
MRI scan data were obtained using a 3.0T MR scanner. Structural MRI, including 3-dimension T1, T2, fluid-attenuated inversion recovery (FLAIR) imaging, was performed. All MR images were reviewed by neuroradiologists. Inevitably, MRI machines and detailed MRI parameters were slightly different between the clinical centers. These differences were thoroughly considered in the analytic process and are fully described in Supplementary Table 1 (in the online-only Data Supplement). In addition, from the subset of participants recruited from Ajou University Hospital, diffusion tensor imaging, susceptibility-weighted imaging, resting-state functional MRI (rs-fMRI), and arterial spin labeling imaging were also obtained. For measurement of neurodegeneration, visual rating of medial temporal lobe (MTL) atrophy in each hemisphere was evaluated by Schelten’s criteria using T1 brain MR images, and then these two values were averaged [22]. Alternatively, we also assessed neurodegeneration using voxel-based morphometry with diffeomorphic anatomical registration through an exponentiated lie algebra procedure on T1-weighted images. Preprocessing of the T1 brain MR data was performed using the Statistical Parametric Mapping software (SPM12; Wellcome Department of Cognitive Neurology, London, UK) implemented in MATLAB (Mathworks Inc., Natick, MA, USA). Before assessing gray matter density, we normalized each participant’s image into the Montreal Neurological Institute space with the normalized images modulated to ensure that relative gray and white matter volumes were preserved following spatial normalization.
Measurement of chronic CVD burden
To measure chronic CVD burden, WMH were evaluated using the modified criteria of Fazekas et al. [23] using FLAIR brain MR images. WMH was separately examined in the periventricular white matter and deep white matter lesions. The severity of deep white matter lesions was classified as mild (deep white matter <10 mm), moderate (deep white matter from 10 mm to <25 mm), and severe (deep white matter >25 mm) based on the greatest diameter of the lesions. The severity of periventricular white matter lesions was divided into mild (cap and band <5 mm), moderate (cap and band from 5 mm to <10 mm), and severe (cap and band >10 mm), based on the size of the cap and band, which were perpendicular to the ventricle, respectively. The degree of overall WMH was assigned to one of three groups by using periventricular and deep white matter hyperintensity (PVWMH and DWMH) severity, such as mild (D1P1 and D1P2), moderate (neither mild nor severe; D1P3, D2P1, D2P2, D2P3, D3P1, and D3P2), and severe (D3P3) [24].
Blood sampling and laboratory assessments
For baseline routine laboratory tests and blood sampling for potential peripheral biomarker research, blood samples were taken after an overnight fast in the morning by venipuncture and collected in serum separating tubes and dipotassium ethylenediaminetetraacetic acid. Baseline routine blood laboratory tests included complete blood cell count, blood urea nitrates, creatinine, albumin, liver function tests, fasting serum glucose, glycated hemoglobin (HbA1c), serum lipids, total protein, folic acid, high-sensitivity C-reactive protein, fibrinogen, venereal disease research laboratory test, treponema pallidum hemagglutination, electrolyte analysis, vitamin B12 test, homocysteine, thyroid function test, and apolipoprotein E (APOE). Blood samples were stabilized and centrifuged at 3,000 rpm for 10 min at room temperature to obtain plasma and serum supernatants. To obtain samples with high purity, the plasma and serum supernatants were further centrifuged under the same conditions, collected, and immediately stored in a -80°C deep freezer. Extracted genomic DNA specimens were also stored at -80°C for future analyses.
Single nucleotide polymorphism (SNP) genotyping arrays
SNP genotyping was carried out using the Korea Biobank Array (Affymetrix Axiom KORV1.1-96 Array, Thermo Fisher Scientific, Santa Clara, CA, USA) at DNA Link Inc. (Seoul, Republic of Korea) [25]. For SNP quality control, SNPolisher was used to exclude low-quality markers by considering a poly high resolution, mono high resolution, and no minor homozygosity. In addition, SNPs with low call rates (<95%) or with a low p-value in the Hardy Weinberg Equilibrium test (<10-6) were excluded. For the sample quality controls, the following criteria were considered to provide better data: call rates (≥97%), hetero rate (within ±2), multidimensional scaling (MDS) analysis (within coordinate±absolute value 0.02), singletons (≤15), identity-by-state test, and gender mismatch. As a result, 769,894 SNPs with 949 participants were extracted for SNP genotyping.
Measure of locomotor activity
A subset of participants who were recruited from Ajou University Hospital were invited to wear a research-purposed accelerometer (Fitmeter; Fit. Life Inc., Suwon, Korea) on their non-dominant wrist for at least seven days while performing their usual activities at home [26,27]. Activity counts in 1 min epochs from the first four consecutive days of data, starting at midnight, were analyzed to assess the rest-activity patterns. Some participants had irregular missing time on their data, indicating device removal or removal during their four-day assessment period. We used the imputation method “missing” to control for this, which was designed and validated for the accelerometer data imputation process using 2003-2004 National Health and Nutrition Examination Survey accelerometer data [28]. Subsequently, we analyzed the mean activity with its variance and skewness using a classical statistical method. In addition, we assessed the rest-activity patterns and circadian phases using a nonparametric analysis method. Nonparametric analysis does not have a priori assumptions about daily activity patterns but instead extracts parameters based on raw activity counts [29].
Patient-derived dermal fibroblast
To perform ex vivo research and the potential generation of induced pluripotent stem cells (iPSCs) harboring the same genetic background of participants, we cultured and established patient-derived dermal fibroblast cells. A subset of participants agreed and donated skin biopsies for patient-derived dermal fibroblast sampling. A skin biopsy was obtained within four weeks of the baseline assessment. We planned and modified our biopsy and culture protocol based on previous studies and our preliminary experiences [30-32]. In brief, a skin biopsy (3 mm3) was taken from the upper inside arm under local anesthesia and aseptic conditions using a disposable punch. The tissue was immediately immersed in 5 mL of warmed culture medium and directly transferred to the laboratory at the same institution. Then, we placed the biopsy piece into a 100 mm dish and cut the tissue into small pieces with a scalpel with a small amount of medium to avoid drying. After 1 min of attachment, we added 10 mL of Dulbecco’s modified Eagle medium (high glucose), supplemented with 20% fetal bovine serum and 1% penicillin/streptomycin. After one week, we changed the culture medium every two to three days. Once enough fibroblasts were identified around biopsy pieces, we trypsinized and passaged the 100 mm dish into another 100 mm dish for further processing (passage 1). Finally, we characterized and validated our fibroblast culture using the fibroblast marker protein SERPINH1 immunocytochemistry (Anti-SERPINH1 monoclonal antibody, Aviva, OACA06643).
Statistical analysis
Continuous variable data were reported as the mean and standard deviation (SD), and categorical data were reported as the number of participants and percentage. We used a one-way analysis of variance (ANOVA) for continuous variables and the chi-squared test for categorical variables for group comparisons. For subsequent subgroup comparisons, we applied the Tukey method. Statistical analyses were performed using R Statistical Software, version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p<0.05.
RESULTS
Demographic characteristics of participants
As of December 2020, a total of 1,013 participants were enrolled in BICWALZS. The demographic characteristics of the participants’ group based on clinical diagnosis are described in Table 1. The mean (SD) age of participants was 72.8 (7.3) years, education years was 7.9 (4.8), depressive symptom score was 6.1 (4.9), and GDS score was 3.3 (1.0). Of all participants, 5% were female, 24% presented with diabetes, and 56% were diagnosed with hypertension. Approximately 28% of participants were apolipoprotein E (APOE) e4 allele carriers. For group comparison based on clinical diagnosis, we performed an ANOVA with subgroup post hoc tests using the Tukey method. Detailed group comparison results are presented in Table 1. In brief, as expected, the AD and vascular dementia (VD) groups were older than the SCD or MCI groups. In addition, the AD and VD groups also exhibited more progressed disease features on the clinical dementia rating sum of the box score, MMSE score, and disability score by S-IADL. Finally, as expected, a higher proportion of the AD group were APOE e4 allele carriers compared to the SCD, MCI, or VD groups. We also assessed and described the demographic characteristics based on cognitive status and two neuroimaging biomarkers (Supplementary Table 2 in the online-only Data Supplement).
MTL neurodegeneration, WMH, and cortical amyloid burden
A total of 817 and 713 participants agreed and underwent brain MRI and amyloid PET, respectively. We first assessed MTL neurodegeneration using Schelten’s (zero to four) scale, and a score of two or higher was considered moderate or above neurodegeneration. As a result, approximately 55.9% of the total participants who underwent brain MRI exhibited moderate or above MTL neurodegeneration. In detail, about 74.2% of participants in the AD group had MTL neurodegeneration that was moderate or above. In contrast, 31.3%, 47.8%, and 91.8% of participants showed moderate or greater MTL neurodegeneration in the SCD, MCI, and VD groups, respectively (Table 1). In addition, we assessed WMH using the modified criteria of Fazekas et al. [23], and participants in the VD group had more severe WMH in their deep white matter and periventricular regions (Table 1). We also analyzed amyloid PET and found that 35.6% of participants had 0.634 or higher SUVR on their amyloid PET, suggesting problematic cortical amyloid deposition. In detail, about 84.9% of participants in the AD group exhibited amyloid positivity on imaging. In contrast, 8.5%, 26.8%, and 14.5% of participants showed amyloid positivity in the SCD, MCI, and VD groups, respectively. We also assessed and described MTL neurodegeneration, WMH, and cortical amyloid burden based on cognitive status and two neuroimaging biomarkers (Supplementary Table 2 in the online-only Data Supplement).
Neuropsychological test
We performed neuropsychological tests to assess the multidomain cognitive function of the study participants and compared the results of SCD, MCI, AD, and VD groups (Table 2). The detailed results are presented in Table 2. In summary, DST-backward scores (attention), K-BNT scores (language), RCFT-copy (visuospatial function), SVLT-delayed recall (verbal memory), RCFT-delayed recall (visuospatial memory), Stroop test (frontal/executive function), and COWAT (frontal/executive function) were significantly different between all groups, except between the AD and VD groups (SCD>MCI> AD or VD, p<0.001 for all five tests). In addition, the RCFT-delayed recall score representing visuospatial memory function was different between all four groups (SCD>MCI>VD>AD, p<0.001). We also assessed the neuropsychological test results based on cognitive status and two neuroimaging biomarkers (Supplementary Table 3 in the online-only Data Supplement).
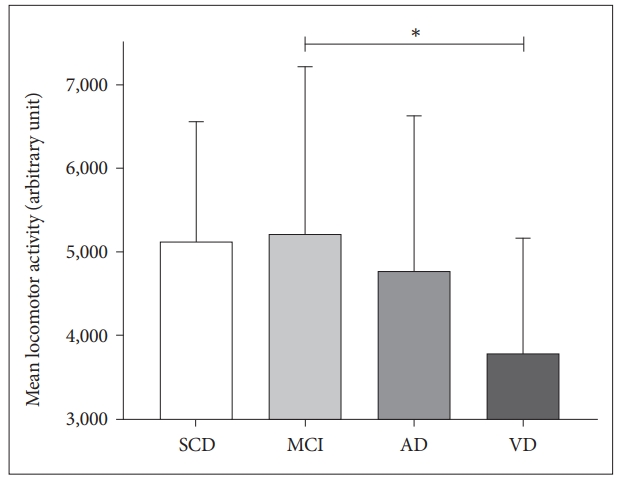
Locomotor activity
Using actigraphy, activity counts in 1 min epochs from the first four consecutive days of data were analyzed to assess the locomotor activity of the participants. We assessed the group differences in mean locomotor activity with skewness. Significant differences in the mean activity were noted between the MCI and VD groups (mean±SD, 5122±1433 vs. 3775±1384, respectively, p=0.02) (Figure 1). However, the skewness did not have a group difference. In addition, the mean activity and skewness showed a large variance between participants. Considering this large variance, locomotor activity should be analyzed with potential confounders, such as sex, body mass index, and comorbidities. In addition, various characteristics such as rest-activity patterns or circadian phase need to be considered and analyzed with clinical characteristics and neuroimaging biomarkers such as disability, cognitive function, cortical amyloid burden, and MTL neurodegeneration.
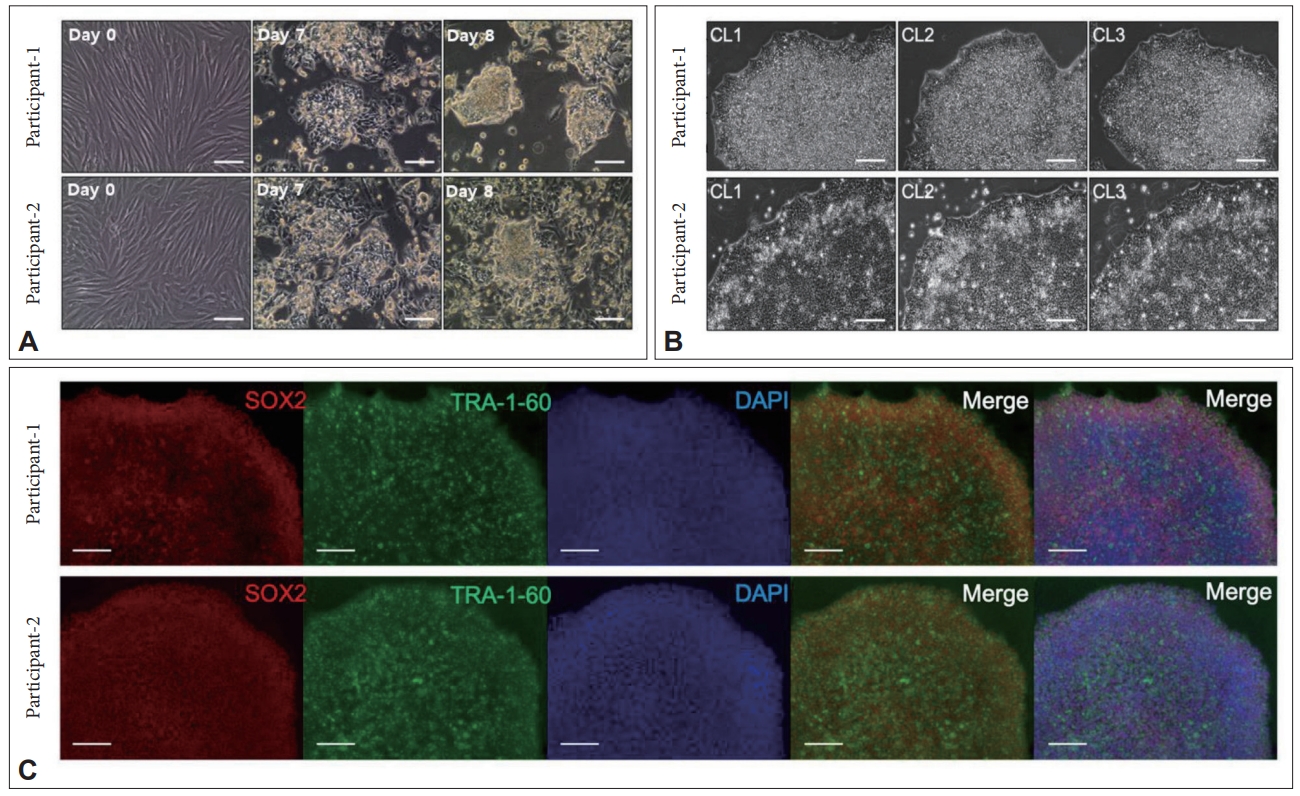
Patient-derived dermal fibroblast
For the purposes of possible ex vivo research and potential generation of iPSCs or brain organoids harboring the same genetic background of participants, we performed skin punch biopsy and retained patient-derived dermal fibroblasts. Stabilized patient-derived dermal fibroblasts exhibited a typical cylindrical morphology with good proliferative potential (Figure 2). As a preliminary experiment, we generated six clones of iPSCs from two derived dermal fibroblasts using the conventional technique with the Sendai virus and checked the typical morphology of iPSCs with basic marker proteins for iPSCs (SOX2 and TRA-1-60). Finally, we performed karyotypic analysis, and there were no chromosomal abnormalities or loss of genetic integrity.
DISCUSSION
Considering the multifactorial nature of neurodegenerative disorders and their heterogeneous clinical presentations, gathering, and integration of multi-layered clinical information, biospecimens, and patient-derived characteristics are critical steps for finding new biomarkers and developing disease modeling processes. In the BICWALZS, we recruited 1,013 older adults who complained of cognitive decline and established a multi-layered dataset including demographic, peripheral bloodbased, neuropsychological, and neuroimaging variables of the study participants. In addition, we performed SNP genotyping arrays, locomotor activity assessments and established patient-derived dermal fibroblasts in a subset of participants. We hope that our integrated clinical data structure, biospecimen, genome-wide genetic information, and patient-derived cells will facilitate optimal biomedical research for neurodegenerative disorders and disease modeling processes not only in South Korea but also abroad.
Characterization of participants’ demographic, neuropsychological, and neuroimaging results compared to similarly designed dementia cohorts might help identify and consider the cohort characteristics and possible selection bias of BICWALZS. For this, we compared our participant characteristics (age, sex, education year, MMSE score, APOE e4 allele carrier, and amyloid positivity on PET) with meta-analysis results assessing 29 cohorts, including 1,897 dementia patients and 1,849 control participants [33]. As a result, AD participants in BICWALZS were slightly older than previous meta-analysis patients with AD (mean±SD, 74.1±7.8 and 69.4±9.3 years, p<0.001). However, the age of VD participants in BICWALZS was similar to the age of meta-analysis VD patients (mean± SD, 75.1±7.0 and 74.5±8.5 years, respectively, p=0.57). We also noted that AD participants in BICWALZS were less educated than meta-analysis patients with AD (mean±SD, 8.4±5.0 and 13.8±3.6 years, p<0.001). The education difference of the VD group showed a similar pattern (mean±SD, 6.4±4.7 and 10.1± 4.2 years, respectively, p<0.001). We believe that the difference in education years reflects cultural differences and may have resulted in slightly lower MMSE scores of the participants with AD or VD in BICWALZS compared to the other meta-analysis patients (data not shown).
We also compared the two most well-known AD biomarkers, the proportion of APOE e4 allele carriers and amyloid positivity on PET. In BICWALZS participants, 46.4% of AD participants and 21.2% of VD participants were APOE e4 allele carriers. Meta-analysis results showed a higher proportion of APOE e4 allele carriers in patients with AD and VD but a relatively preserved e4 allele carrier ratio between patients with AD and VD (61.1% in AD and 28.0% in VD). This allele frequency difference was consistent with previous studies that reported a relatively lower APOE e4 allele frequency in Asian populations [34-36]. Concerning amyloid positivity, we noted that the proportion of amyloid-positive participants was similar in BICWALZS AD participants and meta-analysis patients with AD (85.4% and 87.8%, respectively, p=0.43). Similarly, the proportion of amyloid positivity in the VD group was not significantly different between BICWALZS VD participants and meta-analysis patients with VD (34.6% and 30.4%, respectively; p=0.58). Taken together, although BICWALZS AD participants were slightly older than the mean age of AD patients in 26 dementia cohorts, other participant characteristics such as higher education years, a higher proportion of APOE e4 allele carriers, and higher amyloid positivity in AD participants were generally similar to those of other dementia cohort participants. Finally, we also compared participants’ characteristics of MCI in BICWALZS with an independent nationwide cohort in Korea called KBASE-V [21]. In summary, MCI participants in BICWALZS had similar age and education years as MCI participants in KBASE-V (p=0.63 for age, p=0.09 for education years). The proportion of APOE e4 carriers and amyloid positivity in MCI participants was similar between the BICWALZS and KBASE-V cohorts (p=0.61 for APOE e4 carrier, and p=0.10 for amyloid positivity). Thus, we think that the baseline characteristics of the BICWALZS participants in the MCI, AD, and VD groups are generally acceptable and consistent with worldwide dementia cohorts and independent cohorts in Korea.
Assessing locomotor activity by actigraphy in BICWALZS participants was based on our hypothesis about a possible association between rest-activity patterns, circadian phase, and neurodegeneration in older adults. Although there is controversy on the causality of circadian disruption on neurodegeneration, several previous studies, including our report, suggest a possible association between rest-activity patterns or circadian phase changes with neurodegeneration in patients with cognitive decline [37,38]. A recent report also suggested a possible association between rest-activity patterns, white matter degeneration, and clinical risk factors in individuals at risk for dementia [39]. Integrated analysis assessing the possible association of circadian rest-activity pattern changes with multiple neuroimaging biomarkers (gray matter density, white matter microstructure, resting-status functional connectivity, perfusion, and amyloid deposition in the cortex or subcortex) are in progress in our laboratory and co-work research teams.
Patient-derived dermal fibroblasts are invaluable biospecimens that have great potential for ex vivo research and disease modeling using iPSCs or brain organoid generation [15,40,41]. One of our research teams is performing ex vivo research using patient-derived dermal fibroblasts to assess the cellular circadian rhythm of BICWALZS participants. In this biochemical experiment, we transfected a lentiviral vector (pABpuro-BluF) into patient-derived dermal fibroblasts and successfully measured Bmal1 transcriptional activity using a real-time luminometer [42]. In addition, we successfully generated six clones of iPSCs from two participants and identified two iPSC marker proteins and normal karyotypic properties. We hope that the patient-derived dermal fibroblasts of BICWALZS participants will facilitate optimal biochemical and disease modeling research in the neurodegenerative research field.
In conclusion, we constructed a BICWALZS cohort including patients with SCD, MCI, AD, and VD. The baseline characteristics of the BICWALZS participants in the MCI, AD, and VD groups are generally acceptable and consistent with worldwide dementia cohorts and independent cohorts in Korea [21,33]. We gathered demographic, neuropsychological, and neuroimaging variables as well as genome-wide SNP genotyping arrays, locomotor activity assessment using actigraphy, and patient-derived dermal fibroblast sampling. We hope that our integrated and multi-layered data structure and invaluable biospecimens will facilitate optimal biomedical research for neurodegenerative disorders and disease modeling experiments.