INTRODUCTION
Schizophrenia characterized by disturbances in various aspects such as perceptual, cognitive, social, emotional, and linguistic is a sort of severe mental disorder with high recurrence rate, and disability rate [1]. About 0.3%-0.7% schizophrenia patients worldwide are diagnosed according to epidemiological data [2]. Some studies showed that schizophrenia is actually a typical brain connection disorder, resulting in hallucination and delusion, which is considered as typical positive psychotic symptoms of schizophrenia [3]. However, the pathophysiological mechanism of classification of schizophrenia has still not been clarified [4].
In recent years, an increasing number of neuroimaging studies have focused on the use of resting state functional magnetic resonance imaging (rsfMRI) to explore the pathophysiology of neurodevelopment in schizophrenia [5]. Regional homogeneity (ReHo), a highly reliable rsfMRI measurement method, measures the similarity between a given voxel and its nearest BOLD signal time series in a voxel way through KendallŌĆÖs coefficient of concordance (KCC), providing important information about time synchronization of brain regions [6,7]. Evidence indicates that the underlying pathophysiological mechanism of schizophrenia may be associated with several brain neural networks, including default network (DMN), visual network (VN) and salience network (SN) [8]. However, the consequences of schizophrenia focused on ReHo study are inconsistent. For example, some studies have reported increased ReHo in frontal lobe in schizophrenia [9,10], however, others have shown the opposite results [11,12]. Moreover, the abnormal brain regions identified in these local consistency studies were multiple. A rsfMRI meta-analysis confirmed that the brain dysfunction in each stage were distinct [4]. As is known to all, schizophrenia falls into two categories: drug-naive first episode schizophrenia (Dn-FES) and chronic schizophrenia. The difference between the two categories mainly lies in the course of disease and the influence of drugs, in addition, compared with Dn-FES, patients with chronic schizophrenia experience more social stress and stressors and indicated more extensive brain damage. Therefore, aggregating the eligible studies to achieve consistent results makes a lot of sense for identifying the respective neurobiological markers, which needs to be done by effective means of meta-analysis. Activation likelihood estimation (ALE), a coordinate-based meta-analysis, reveals image-specific markers by avoiding laboratory bias in the most consistent spatial changes of brain structure and function across studies [13].
To our knowledge, a few meta-analysis of rsfMRI studies have revealed local neural connectivity abnormalities in schizophrenia. Kuhn et al. [14] performed a meta-analysis on the resting brain activity of schizophrenia and depression patients. Xiao et al. [15] conducted a meta-analysis of local abnormal connections in schizophrenia and their unaffected relatives. Nevertheless, existing studies did not detailly clarify the difference between Dn-FES and chronic schizophrenia, possibly because of the unavailability of data. As a result, it is necessary to use ALE algorithm to make a quantitative meta-analysis of the consistent brain alterations on patients with schizophrenia classified according to their course of illness.
Hence, the purpose of the present study was to conduct two group comparsions: 1) all schizophrenia (Dn-FES and chronic schizophrenia) and healthy controls (HCs); 2) chronic schizophrenia and HCs. It was hypothesized that: the findings of all schizophrenia patients and chronic patients would show the special ReHo abnormalities which belong to the current known network.
METHODS
Literature selection
The meta-analysis of neuroimaging studies was conducted according to the PRISMA statement and recorded using the suggested checklist.
Search strategy
We have systematically searched all articles in Pubmed, Embase, Web of science and Cochrane Library. The search strategy was performed with Medical Subject Heading (MESH) keywords and their related phrases in ŌĆ£SchizophreniaŌĆØ [MeSH] OR ŌĆ£SchizophreniasŌĆØ [Title/Abstract] OR ŌĆ£Schizophrenic disordersŌĆØ [Title/Abstract]) OR ŌĆ£disorder schizophrenicŌĆØ [Title/Abstract] OR ŌĆ£disorders schizophrenicŌĆØ [Title/Abstract]) OR ŌĆ£Schizophrenic DisorderŌĆØ [Title/Abstract] OR ŌĆ£Dementia PraecoxŌĆØ [Title/Abstract] or ŌĆ£schizophr*ŌĆØ [Title/Abstract]; AND ŌĆ£ReHoŌĆØ [Title/Abstract] OR ŌĆ£Regional homogeneityŌĆØ [Title/Abstract]) OR ŌĆ£local consistencyŌĆØ [Title/Abstract] OR ŌĆ£coherenceŌĆØ [Title/Abstract]; AND ŌĆ£functional magnetic resonance imagingŌĆØ [Title/Abstract] OR ŌĆ£fMRIŌĆØ [Title/Abstract]) OR ŌĆ£resting stateŌĆØ [Title/ Abstract] (Supplementary Table 1 in the online-only Data Supplement).
Inclusion and exclusion criteria
Studies will be included if the article met the following conditions: 1) the research target had been diagnosed with schizophrenia; 2) studies were rsfMRI study, use of ReHo; 3) studies based on whole-brain analysis; 4) studies were compared with patients with schizophrenia and HCs group; 5) studies were reported cluster information (e.g. coordinates, cluster size, thresholding approaches); 6) studies were published on English language journal.
Studies will be excluded if the article met the following conditions: 1) studies were not imaging study; 2) without peer review; 3) not whole brain study (e.g. region of interest, volume of interest, support vector machine); 4) articles were not provided coordinate data or even after contacting the authors by email remained unavailable; 5) studies were not original study (e.g. letters to the editor, review articles, case reports, and animal experimental studies); 6) studies were not published in English journals; 7) cohe ReHo (coherent regional homogeneity) was used instead of KCC ReHo; 8) unable to obtain full text.
Data extraction and quality evaluation
We extract useful data from the selected studies as follows: author, years of publication, gender distribution, sample size, diagnosis and classification system of schizophrenia, diagnosis, age (mean┬▒SD), scanner (magnetic field strength), eye state, repetition time/echo time, thickness, slice gap, full-width at half-maximum (FWHM, threshold), and drug states, furthermore, we collected x, y, and z coordinates reported using Talairach or Montreal Neurological Institute (MNI), which have statistically significant findings. If necessary, information is missing, we will contact the author to obtain original article. We used a 10-point checklist that included specific methods for clinical and demographic and imaging to assess the quality of the literature included basic information and suitable studies (Supplementary Table 2 in the online-only Data Supplement). Literature search, study selection and data collection were performed independently by two psychiatrists (W.Y.M. and W.W.X.), and any differences were judged by two experienced psychiatrists (W.Y. and R.R.Z.).
Statistical analysis
The data analysis was dealt with GingerALE software (www.brainmap.org) [16]. ALE is a widely used coordinated based meta-analysis method that regards the focus of the report as a spital distribution centered on a given coordinate [17,18]. ALE technology regards the focus of the report as a spatial probability distribution centered on a given coordinate, rather than a spatial probability distribution focused on a point [19]. This method allows the creation of an activated probability map using the focus of different articles and compares it with a random spatial distribution, and the analysis carried out in MNI space [20]. In order to assure statistical conspicuousness, we used 1,000 simulations to test arrangement of randomly distributed focuses, the cluster level Family Wise Error (FWE) of ALE map was p<0.001 and the cluster-forming threshold was p<0.001 [21]. To illustrate this, We use the neuroimaging and brain network visualization software BrainNet Viewer (http://www.nitrc.org/projects/bnv/) to visualize the brain maps of ALE [21].
We first conducted ALE meta-analysis on all schizophrenia patients, then excluded four diagnoses as the Dn-FES (the duration of the disease was less than 2 years) patients experiments (because the research on the first episode schizophrenia patients are relatively small, the significance of combination is not significant, so this study did not combine the first episode patients) and a partial drug-naïve study, after that, conducted meta-analysis on the chronic schizophrenia patients (the duration of the disease was less than 2 years).
RESULTS
Included studies and sample features
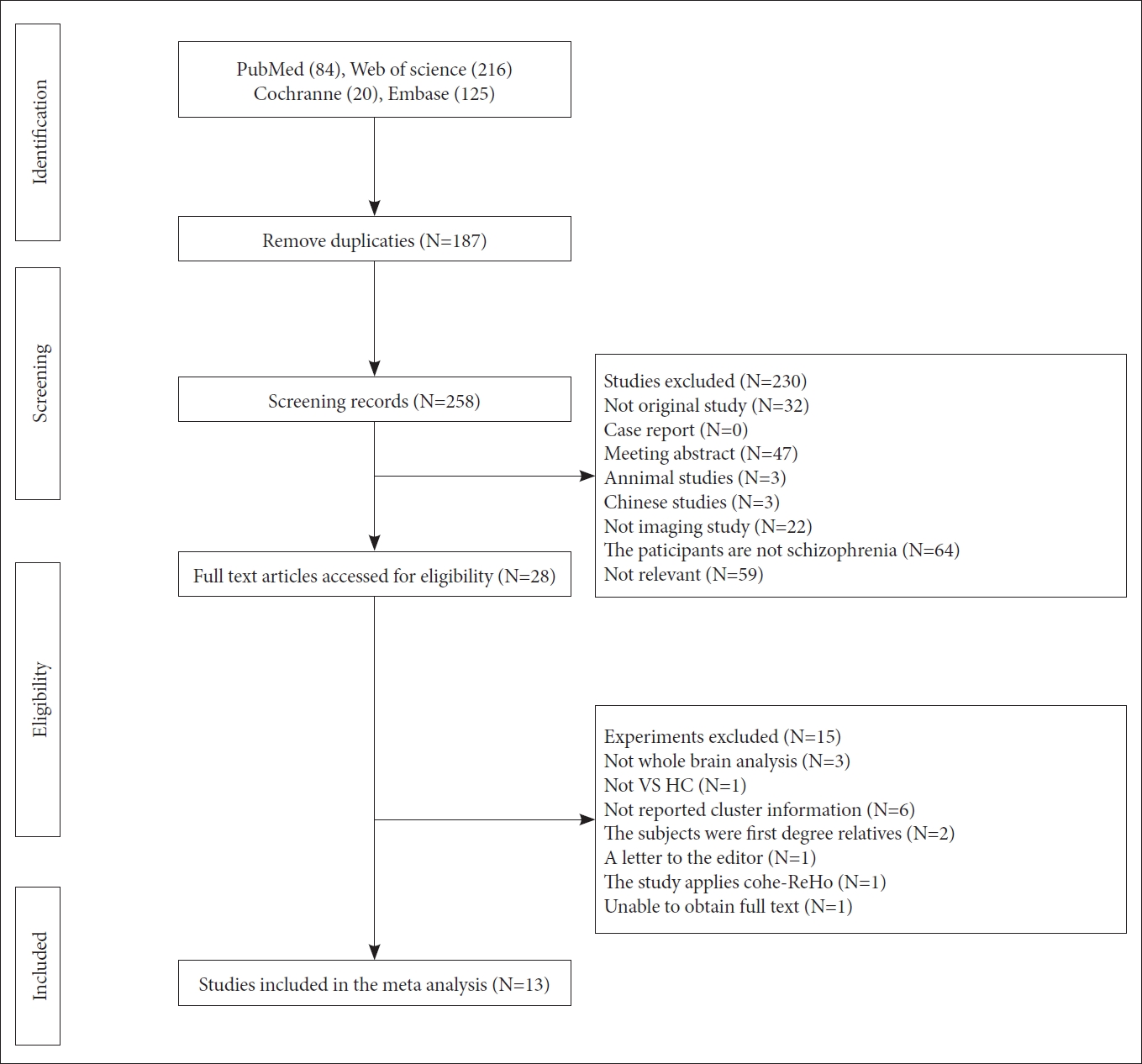
Through literature search of four databases (pubmed, web of science, embase, cochrane library), we have retrieved 445 documents. After initially removing the duplicates and browsing the title and summary, we found that 28 studies met the inclusion criteria, furthermore, after a detailed review of the full text, a total of 13 studies met the inclusion criteria [8,9,11,12,22-30]. Figure 1 illustrates the identification and exclusion flow chart for the study. The included research reported ReHo differences in 511 schizophrenia (193 with FES and 318 with chronic schizophrenia), and compared with 452 HCs. The research characteristics and quality scores included in this meta-analysis are presented in Tables 1 and 2.
ReHo brain alterations comparison between all schizophrenia and HCs
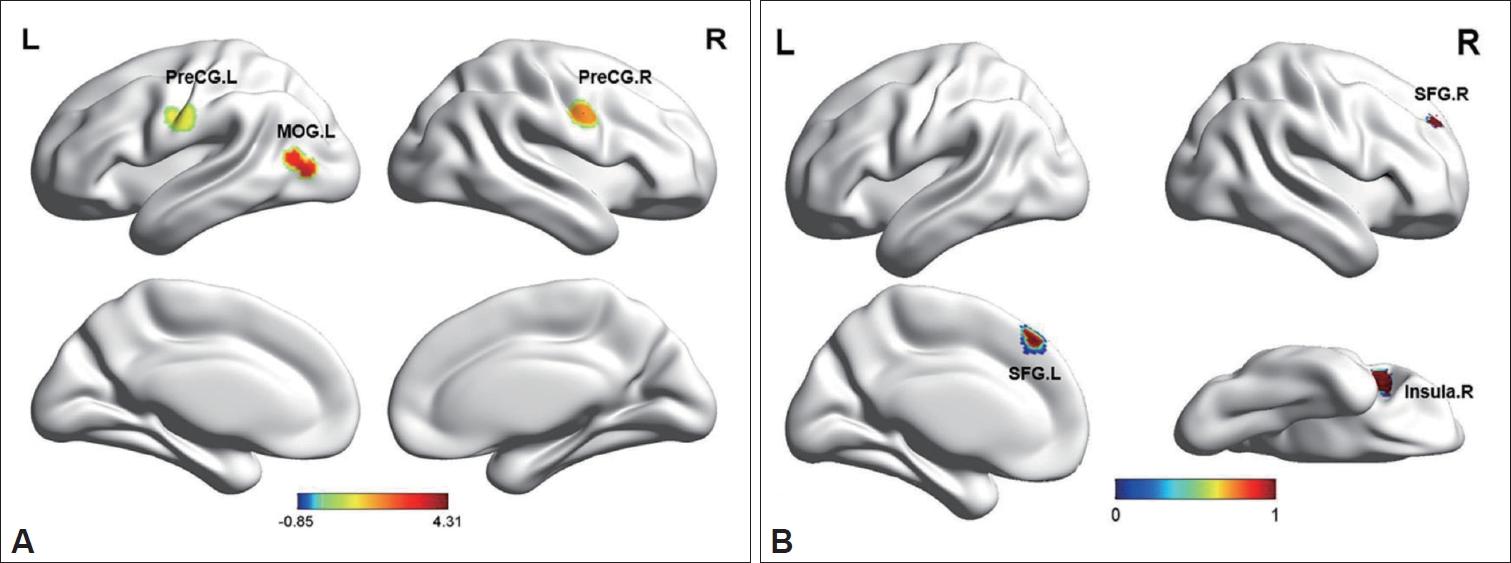
The comparison of ALE meta-analysis results between all schizophrenia group and HCs group are briefly summarized in Figure 2 and Table 3. The comparison between all schizophrenia and healthy control group showed decreased ReHo in bilateral precentral gyrus (PreCG) and left middle occipital gyrus (MOG), whereas increased ReHo in bilateral superior frontal gyrus (SFG) and right insula (Table 3, Figure 2).
ReHo brain alterations comparison between chronic schizophrenia and HCs
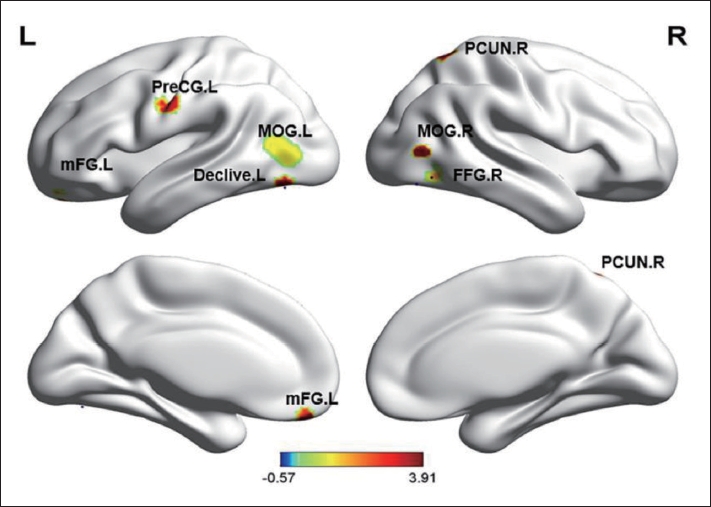
The comparison of ALE meta-analysis results between all schizophrenia group and HCs group are summarized in Figure 3 and Table 4. We found that decreased ReHo in bilateral MOG, right fusiform gyrus (FFG), left PreCG, left cerebellum, right precuneus (PCUN), left medial frontal gyrus and left anterior cingulate (ACC) (Table 4, Figure 3). No significant abnormal increased brain areas were found in the chronic schizophrenia.
DISCUSSION
Our study is the first quantitative meta-analysis, which combines the whole brain ReHo results of rsfMRI study in different stages of schizophrenia in a voxel way. Our advantage lies in the systematic and comprehensive understanding of schizophrenia in three groups (all schizophrenia group, chronic group, HCs group).
The Dn-FES in comparison with chronic patients indirectly
As assumed, both the two groups had regional abnormal of varying degrees. The significant finding of our meta-analysis is that there are obvious alterations in frontal and occipital regions in all schizophrenia. Meanwhile, in chronic schizophrenia, there are more extensive local consistent changes, involving frontal, temporal, parietal, and occipital regions and even cerebellum. Compare with all schizophrenia group, the results showed that both the Dn-FES and chronic schizophrenia suffered from the common damage of occipital lobe and frontal lobe, which were not affected by the course of disease and medication. It is suggested that these brain regions may be abnormal in the early stage of schizophrenia, as well as not affected by the occurrence and development of disease.
Specific imaging abnormal markers
Our meta-analysis found consistent areas of decreased ReHo in the MOG in all schizophrenia patients compared with HCs and chronic schizophrenia patients compared with HCs. Occipital lobe lesions that cause hallucinations, color blindness, or agraphia have been confirmed [31]. As the core area of the VN, MOG is mainly responsible for processing visual function [31]. In schizophrenia, structural and functional abnormalities of VN have been previously reported [32]. For example, the association between visual hallucinations and VN damage in schizophrenia patients has been confirmed, and the total volume of occipital gyrus has been reduced, and the white matter magnetic transfer rate and fractional anisotropy adjacent to the visual processing area have been reduced [31,32]. The occipital cortex of schizophrenia patients showed activity deficits compared with the control group in task-related fMRI studies [33]. Occipital cortex may be the neurobiological basis of visual processing defects in the early stage of schizophrenia [34]. In conclusion, the function and structure of occipital lobe may also be related to schizophrenia, which appears in the early course of schizophrenia and persists throughout the course of the disease.
Another area of interest observed in all schizophrenia patients and chronic schizophrenia patients compared with HCs is PreCG, which is an unique region of local functional connectivity alteration [35]. Evidences confirmed that PreCG plays an important role in social cognition [35]. Watanuki and his collegues show that the excessive activity of the central anterior gyrus can lead to the emotional processing dysfunction of schizophrenics [36]. A recent study has shown that the severity of clinical symptoms in schizophrenics is related to the disorder of local functional connection in the PreCG [37]. In a word, the local consistency of PreCG in schizophrenia may be related to the pathophysiological mechanism and clinical symptoms.
We also found increased ReHo in the insula in all schizophrenia patients. Insula is one of the most important parts of the SN, responsible for emotional processing and working memory [38]. Both Increased ReHo and decreased ReHo were reported in the insula in patients with schizophrenia [11,39], while some other studies showed negative results [29,40]. The reason may be attributed to the heterogeneity of the sample, statistical methods and sample size. A multicenter structural magnetic resonance meta-analysis showed significant thinning of the insula cortex and a significant correlation with drug dose, disease duration and age of onset [41]. Compared with HCs, functional imaging studies demonstrated reduced local function in the left insula in schizophrenia [11]. Therefore, insula is unstable in patients with schizophrenia, while the increase of ReHo in the insula of all schizophrenia patients may act a key role in the functional compensation for the systematic structural anomalies.
Interestingly, our study observed inconsistent activation of the frontal lobes. In the all schizophrenia group, we found that the frontal lobe was highly activated, while in the chronic schizophrenia group, the frontal lobe was low activated. Previous studies has demonstrated bilateral frontal gray matter volume is negatively correlated with hallucinations which is one of the main symptoms of schizophrenia [42]. Many patients commit suicide which is a serious complication of schizophrenia under the influence of hallucinations and delusions [43,44]. Converging lines of evidence indicate that the phenomenon is directly related to the dysfunction of circuits based on the prefrontal cortex. In conclusion, there are abnormalities of frontal lobe structure and function in schizophrenia, which are related to clinical symptoms and cognitive dysfunction. We speculated that frontal lobe damage is a stable biomarker in schizophrenia. Therefore, the decrease of ReHo in the frontal lobe of patients with chronic schizophrenia may be related to the psychotic symptoms, while the increase of ReHo in the frontal lobe of the first-episode patients may act a pivotal in the compensation of psychotic symptoms of schizophrenia.
In addition to the areas of the brain that were commonly damaged, our study found that in the chronic schizophrenia group decreased ReHo in the PCUN and ACC also was observed, which are mainly located in the DMN [45]. As we know, DMN is responsible for the consciousness maintenance, emotional processing, self-introspection, and episodic memory extraction [46]. Once in disorder, DMN may cause dysfunction, and thus lead to metal illness [46]. Bluhm et al. [47] found that the decreased functional connectivity between the cingulate gyrus and multiple default network brain regions in schizophrenia. As a result, the findings of our study are highly credible. Other abnormal brain region like cerebellum also play an important role in chronic schizophrenia. The representative characteristics of damaged cerebellum involve deficits in executive function, linguistic learning, visual spatial processing and regulation of affect [48].
Limitations
In our study, some limitations must be pointed out: 1) because there are only three studies on the FES, we have not combined the studies on the FES and can not directly compare the differences between the FES and the chronic patients; 2) individual heterogeneity test cannot be completed by ALE and ALE technology cannot evaluate the significance level of contribution results; 3) as suggested by Eickhoff, we used p<0.001 as the threshold for cluster formation and 0.001 for cluster level inference. Most results were significant only before correction for multiple comparisons in false discovery rate (FDR), but our results could not be corrected by FDR, however, in previous simulation work, we determined that uncorrected p<0.001 was empirically equivalent to corrected p<0.05 in our approach, we will use a more stringer correction for multiple comparisons in future study; 4) our meta-analysis samples are all Chinese, which may limit the application of these findings in other populations, further efforts are needed to extend the ReHo method to other patients with schizophrenia; 5) because of the limitation of the study method we could not put other factors (such as PANSS scores, head motion) as covariates into ALE analyses and could not assess the effect of these factors, partially limiting the interpretability and generalizability of the results.
Clinical implications
Correct understanding of any brain changes in schizophrenia can deepen the understanding of brain development changes related to the occurrence or development of the disease. Based on the meta-analysis of voxels, we found that some brain regions of schizophrenia had local functional connectivity abnormalities. The abnormal spontaneous brain activity may reflect the neuropathological characteristics of schizophrenia, as well as lay a foundation for the establishment of objective diagnostic markers of schizophrenia. Furthermore, our study results give us an enormous assist to determine the course of disease and the role of drugs in different stages of neurodevelopmental disorders in schizophrenia.
Conclusion
Our meta-analysis showed that the common local abnormal brain areas of the drug-naïve patients and chronic patients were MOG, PreCG, frontal lobe and insula, while the brain damage of the chronic patients was more extensive, including PCUN, ACC and cerebellum, which indirectly compared the first and chronic patients. Major damaged brain networks include DMN, VN and SN, contributing to our understanding of the progressive pathophysiology of schizophrenia.