INTRODUCTION
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder whose core symptoms include developmentally inappropriate levels of inattention, impulsivity, and hyperactivity [1]. ADHD was previously called attentiondeficit disorder in the Diagnostic and Statistical Manual of Mental Disorders III (DSM-III) in 1980 but was renamed ADHD in the Diagnostic and Statistical Manual of Mental Disorders III-Revised (DSM-III-R) in 1987 [2]. The International Statistical Classification of Diseases and Related Health Problems 10th edition [3] uses the specific diagnostic term of hyperkinetic disorder to describe the syndrome of ADHD [4]. Despite the centrality of hyperactivity in the diagnosis of ADHD, research on objective tests measuring hyperactivity has been very limited [5]. The continuous performance test (CPT) has been widely used as an objective test to assess the impulsivity and inattention of patients with ADHD, whereas assessments of hyperactivity currently rely on subjective reports from parents/teachers and the observations of clinicians [6]. Diagnosing ADHD can be challenging, as the description of hyperactivity differs among informants due to its situational variability, as high activity levels are inconsistent and occur under conditions of low environmental stimulation [7].
The Quantified Behavioral Test (QbTest; Qb Tech, Stockholm, Sweden) was recently approved by the Food and Drug Administration as an effective tool to aid in the clinical assessment of ADHD. The QbTest measures the motor activity of the participantŌĆÖs head during a CPT test using an infrared camera [8]. However, a recent study reported that the QbTest was insufficient as a diagnostic test for ADHD, as it is unable to differentiate ADHD from other neurodevelopmental disorders [9]. A recent meta-analysis reported medium-to-large effect sizes using an actigraphy (standardized mean difference 0.64, 95% confidence interval 0.43-0.85) to differentiate individuals with ADHD from controls [4]. However, no standardized protocol exists regarding the application of clinical actigraphy, and no normative data are available on activity according to age and gender [10].
The Robot-assisted Kinematic Measure for ADHD (RAKMA) was developed as an objective tool to assess movement in patients with ADHD. A robot assists the process to increase the engagement of the participant and detect his/her movements. The purpose of this study was to evaluate the clinical utility of the RAKMA in patients with ADHD. We hypothesized that the performance variables of the RAKMA would differentiate between individuals with ADHD and healthy controls (HCs) and that there would be significant correlations between RAKMA variables and parent-reported clinical scale scores.
METHODS
Participants
In total, 35 patients with ADHD and 50 HCs were enrolled during December 2016 to April 2017. Patients with ADHD visited the psychiatry and pediatrics outpatient clinics of the Hanyang University Medical Center. The ADHD diagnosis was confirmed according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) by a thorough interview of both the child and parent administered by board-certified psychiatrists. The exclusion criteria for ADHD were: a psychiatric diagnosis other than ADHD; abnormalities in sight, hearing, or hand movement; metal allergies; and lack of cooperation. Patients with ADHD who were already taking medication were re-evaluated by a board-certified psychiatrist after a washout period of 3 days (considering that the longest half-life among ADHD medications is 6.8 hours) [11]. The HCs were recruited following the same exclusion criteria with the addition of a diagnosis of ADHD.
Written informed consent was obtained from all parents/guardians, and the children provided verbal consent to participate after sufficient explanation of the study prior to enrollment. All study protocols were approved by the Institutional Review Board of the Hanyang University Medical Center (IRB Approval no. HY17-226-2). The authors assert that all procedures contributing to this study complied with the ethical standards of the relevant national and institutional committees on human experimentation and with the 2008 revision of the 1975 Declaration of Helsinki.
Clinical assessments
The CBCL is a screening tool used to measure various problem behaviors in children based on parental self-reporting; the Korean version (K-CBCL), which has well-established reliability and validity [12], consists of 120 items that are rated on a scale of 0 to 2 (0=no behavior, 1=occasional behavior, and 2=frequent behavior). The results were transformed into T-scores with a mean of 50 and a standard deviation of 10. Higher T scores indicate a greater degree of psychopathology. We used the attention problems subscale and the DSM-oriented attention problem scale scores to measure ADHD symptom severity.
ADHD symptom severity was also assessed using the Korean Attention-Deficit/Hyperactivity Disorder Diagnostic Scale (K-ADHDDS) [13]. The K-ADHDDS was developed based on the DSM-IV diagnostic criteria and the Gilliam Attention Deficit Hyperactivity Disorder Test [14]. It consists of 36 items, with 13 items measuring hyperactivity, 10 items measuring impulsivity, and 13 items measuring inattention. Parents or teachers are instructed to rate each item on a three-point Likert scale (0-2), with higher scores indicating greater severity. The K-ADHDDS has an internal consistency of 0.94 and a test-retest reliability of 0.92.
The Robot-assisted Kinematic Measure for ADHD
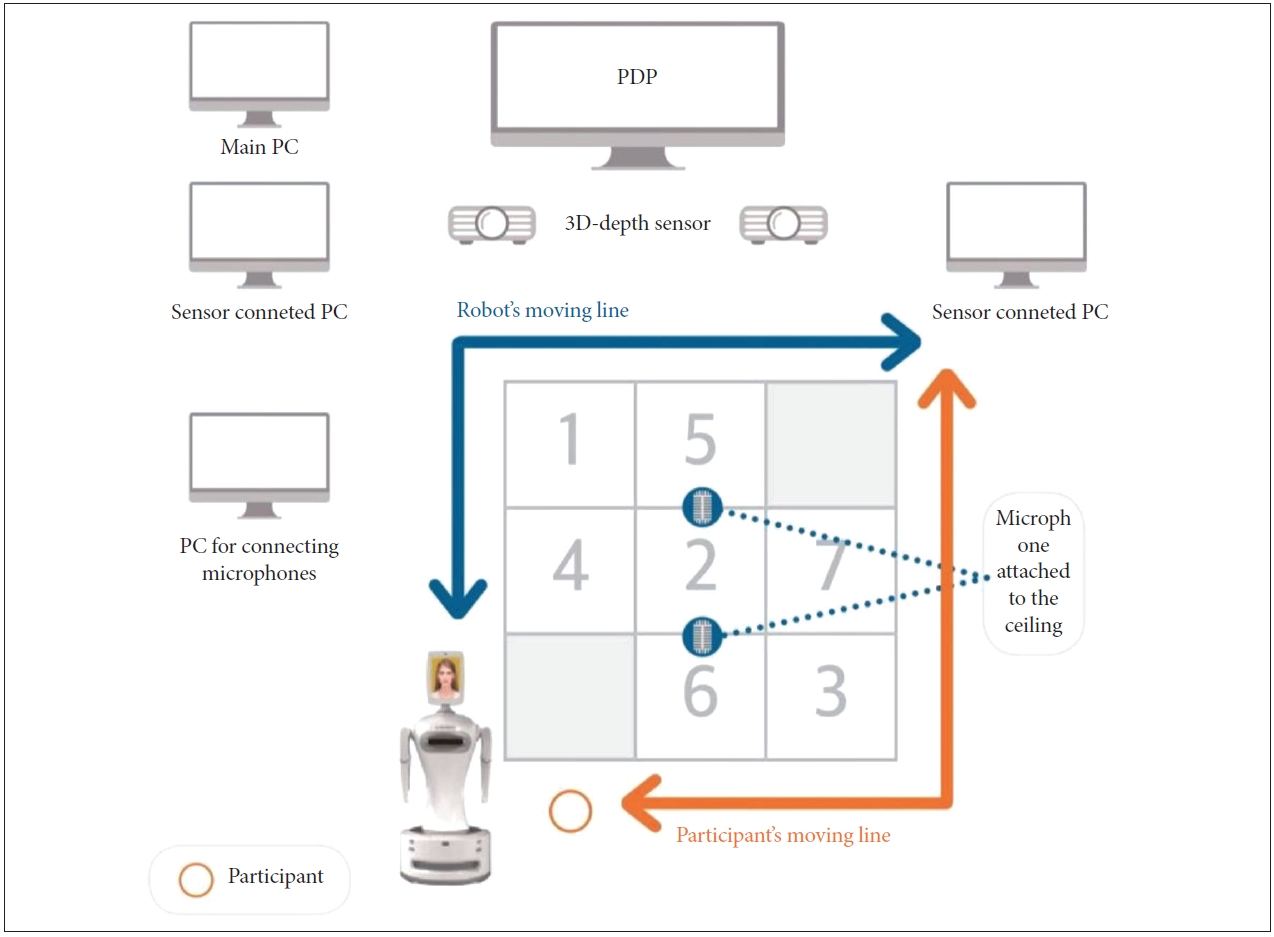
The robot was designed by Robocare (Seoungnam, South Korea) and was named Silbot (http://robocare.co.kr/index.php/silbot/) (Figure 1). The face of the robot was presented on a touch screen that showed an avatar with various facial expressions. We attached a three-dimensional (3D) camera on the chest area to detect the movements of the participants and attached LED sensors to each hand. Touch sensors and distance sensors were attached to the abdominal area to maintain distance and protect the robot from colliding with surrounding objects. We placed a 3D depth sensor around the robot to measure the participantsŌĆÖ movement, a large-screen TV was used to present visual stimuli during the task, and a computer was used to collect movement data (Figure 2).
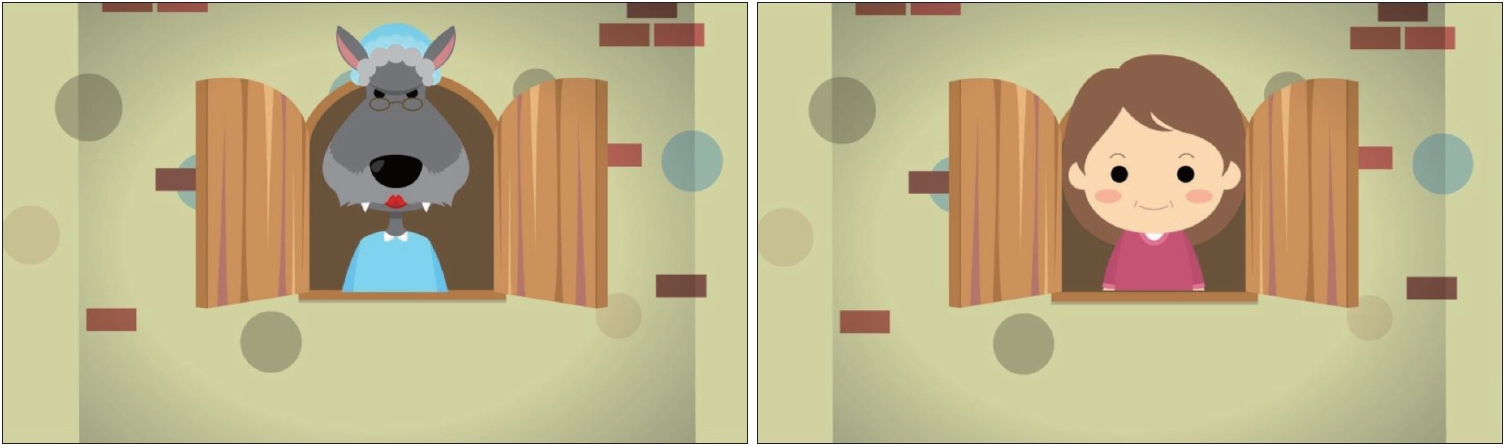
RAKMA is a 15-30-min test (5-10 min per trial, a total of 3 trials) that combines a task measuring inattention and impulsivity with motor activity measurements using a robot. The robot instructs the participant to observe and then follow its movement across a 3├Ś3 mat filled with numbers from 1 to 7 (Figure 2). As the participant moves across the mat, an auditory stimulus (ŌĆ£It is little red riding hoodŌĆØ) and a visual stimulus (a person or a wolf on a TV screen) are presented simultaneously (Figure 3). When the visual stimulus is a person, the participant is instructed to wave; however, when a wolf is presented, the participant is instructed to sit down. If the participant responds correctly, a beep sound is provided, and the participant continues moving across the number mat toward the finish line. If the participant responds incorrectly, the trial ends. The participant repeats these steps three times. During trial 1, the robot takes three steps to move from the ŌĆśstartŌĆÖ point to the ŌĆśfinishŌĆÖ line. During trial 2, the robot takes four steps; during trial 3, the robot takes five steps from the ŌĆśstartŌĆÖ point to the ŌĆśfinishŌĆÖ line. The auditory and visual stimuli were presented once in trials 1 and 2 and twice in trial 3.
We measured the stimulus-response performance based on the following four variables: 1) correct reactions (number of correct responses to simultaneous auditory and visual stimuli); 2) commission errors (number of incorrect responses to simultaneous auditory and visual stimuli, a measure of impulsivity); 3) omission errors (number of failures to respond to simultaneous auditory and visual stimuli, a measure of inattention); and 4) trial completion (number of correct responses to both the stimuli and the robot).
Movement was measured in terms of the following three variables: 1) reaction time (the average interval from stimulus presentation to the beep indicating a correct response during the three trials), 2) migration distance (the average difference between the participantŌĆÖs travelling distance and the robotŌĆÖs travelling distance during the three trials), and 3) migration speed (the average speed across the numbered mat during the three trials). DSM-5 defines hyperactivity as ŌĆ£frequent fidgeting of hands or feet, difficulties in remaining seated, inappropriate running or climbing, and/or acting as if driven by a motor.ŌĆØ In previous studies measuring hyperactivity using actigraphy or the QbTest, hyperactivity was measured by the amount of total movement [4,8]. Therefore, we defined hyperactivity as increased migration distance, which reflects to total amount of movement of the participant. Reaction time is related to processing speed and inattention, whereas migration speed would be most related to impulsivity.
Statistical analysis
The demographic and clinical characteristics of the ADHD and HC groups were compared using independent t-tests for continuous variables and chi-square or FisherŌĆÖs exact tests for categorical variables. Due to the predominance of boys in the ADHD group, we compared the measures between the ADHD group and HC group in boys, separately using Mann-Whitney test. We applied SpearmanŌĆÖs correlation analysis to investigate the correlations between ADHD clinical variables and the variables measured using the RAKMA as well as the correlation between the RAKMA stimulus-response variables and the movement variables. All statistical analyses were performed using SPSS ver. 22.0 software (IBM Corp., Armonk, NY, USA), and a p-value<0.05 was considered significant.
RESULTS
The demographic and clinical characteristics of the ADHD and HC groups are presented in Table 1. A higher proportion of male participants was observed in the ADHD group (p=0.014), and the ADHD group exhibited significantly more CBCL attention problems, DSM-oriented attention problems, and K-ADHDDS scores (all p<0.001). The ADHD group had significantly fewer correct reactions, more commission errors, more omissions errors, slower reaction times, longer migration distances, and faster migration speeds.
Table 2 presents the correlations between the ADHD clinical variables and the RAKMA performance variables. Correct reactions and migration distances were significantly negatively correlated with all three clinical variables, whereas commission errors and omission errors had significant positive correlations with all three clinical variables. Migration rates were positively correlated with CBCL DSM-oriented attention problems scores as well as with K-ADHDDS scores.
Supplementary Table 1 (in the online-only Data Supplement) compares the parameters in the ADHD and HC groups in boys. The boys in the ADHD group showed more commission errors, longer reaction time, migration distance and also migration speed compared to the HC group. These results were similar to the main results, except that correction reactions and omission errors were no longer significant.
Table 3 shows the correlation between the RAKMA stimulus-response variables and the movement variables. Reaction times were positively correlated with trial completions. Migration distances were positively correlated with correct reactions and trial completions but negatively correlated with commission errors and omission errors. Migration speeds were negatively correlated with correct reactions but positively correlated with commission errors and omission errors.
DISCUSSION
Our results suggest that the RAKMA is clinically useful as an ADHD diagnostic aid. Patients with ADHD provided fewer correct responses and more omission errors (greater inattention) and commission errors (greater impulsivity) than the HCs, but there were no differences in trial completions. Patients with ADHD also had slower reaction times, greater migration distances, and faster migration speeds, which indicates higher levels of inattention, hyperactivity, and impulsivity, respectively. Trial completions and reaction times were not correlated with the clinical scale scores, suggesting that these two variables are less useful than the other RAKMA variables for diagnosing ADHD. Migration distance, a measure of hyperactivity, was significantly correlated with clinical scores rated by the parents, suggesting high criterion validity. The neuropsychological performance of patients with ADHD can be confounded by their diagnosis [15]. Barkley [16] hypothesized that hyperactive patients would perform worse on executive tasks, such as those involving delayed reactions, problem solving, flexibility, and sustained attention, whereas inattentive patients would be more impaired on tasks involving memory, focused attention, and timed information processing. Another study reported that inattentive children have more problems with selective attention and slow processing, whereas hyperactive children have more difficulties with executive and inhibitory functions [17]. Barkley [18] postulated that hyperactivity is connected to dopaminergic dysfunction whereas hypoactivity is a norepinephrine phenomenon. These changes are accompanied by different neuropsychological profiles. Therefore, objective measures of both hyperactivity and neuropsychological functioning (e.g., the RAKMA) may be more useful than simple neuropsychological function tests for differentiating among ADHD subtypes. Future studies with sample sizes large enough to conduct subanalyses according to ADHD subtype are warranted.
Previous infrared-based motion-tracking tools were limited by the fact that they measured only head movement. The McLean Motion and Attention Test System, a precursor to the Qb test, measures head immobility duration, head movement, head displacement, head area, head spatial complexity, and head temporal scaling [19]. The Qb test presents data on head movement using five raw parameters: time active, distance, area, microevents, and motion simplicity [8]. An actigraph measures movement on only the part of the body on which the actigraph is applied. The RAKMA is unique, as it tracks the movements of the whole body during the 10-min task. However, there is no gold standard regarding the area of body measurement. Further studies should be conducted to examine which regions of the body are best to measure when determining hyperactivity in patients with ADHD.
Another strength of the RAKMA is its use of a robot to assist the patient with the task. Research on the use of socially assistive robotics (SAR) in child psychiatry has been mainly focused on autism spectrum disorder (ASD), and the application of SAR to ADHD is novel [20]. SAR refers to a robot that provides assistance to the user in social interactions [21]. SAR is useful for eliciting target behavior for purposes of diagnosis and treatment, modeling and teaching skills, and quantifying observed behavior in children with ASD. SAR has also been demonstrated to improve cognitive attention and cortical neuron activity and has the ability to alleviate stress in patients with dementia [22]. Moreover, as patients needed less supervision while interacting with the robot, their caregivers experienced less stress. This is the first study to apply robotic techniques to diagnose ADHD.
Our study had several limitations. First, the sample size was small, limiting statistical power. A significant difference in gender distribution was observed between the ADHD and HC groups, and there were only five female participants in the ADHD group, which could have confounded the results. However, a subgroup analysis of boys rendered similar results to that of both genders combined. We included all subtypes of ADHD due to the sample size limitation, making it a heterogeneous group with variable behavioral characteristics. We did not perform an IQ test and therefore could not exclude children with intellectual disabilities. Further studies should examine RAKMA performance according to subtype to reduce the confounding effect of subtype.