Current Challenges and Future Opportunities for Child and Adolescent Psychiatry in Japan
Article information
Abstract
Japan has been facing a serious shortfall of child and adolescent psychiatric workforce relative to increasing service needs. Likely because of a combination of limited workforce supply and limited trust or perception of effectiveness, mental health services are under-utilized by the educational and child welfare systems. Child and adolescent psychiatry (CAP) has not been a formally established specialty in Japan. The lack of basic structure in the specialty most likely contributes to a lack of training facilities, limited exposure to and interest in the specialty, and hence an inadequate workforce. To date, there exists no standardized training program for CAP in Japan and each training hospital determines its own teaching curriculum and training content. Clinical experience in CAP varies greatly among hospitals. To solve current problems in child and adolescent psychiatry in Japan, we advocate for the development and establishment of a more standardized child and adolescent psychiatry training system that is akin to what exists in the US and that teaches and evaluates according to specific competencies. Through standardizing care and education and ultimately improving workforce, the quality of mental health services can be raised. The tragic and costly consequences of unidentified and untreated mental illness in youth can be avoided by taking timely evidence based actions in partnership with others.
INTRODUCTION
Japan has been facing a serious shortfall of child and adolescent psychiatric workforce relative to service needs.12 Recent large scale epidemiological studies have demonstrated that the prevalence rate of neurodevelopmental disorders, such as Autism Spectrum Disorder (ASD) and Attention Deficit Hyperactivity Disorder (ADHD), continues to increase.3456 This trend is similarly observed in Japan.789 According to the World Health Organization, approximately 10–20% of youth experience mental health disorders.10 Furthermore, 70% of mental health disorders have their onset prior to the age of 25 years.11 The Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study1213 revealed that the onset of Major Depression was earlier than previously presumed, with the first episode most frequently occurring in adolescence.14 Untreated mental health problems in childhood can be transmuted into various psychiatric diseases.151617181920 Moreover, there are several psychiatric disorders (i.e., early onset neurodevelopmental disorders) that are most often diagnosed in childhood and that require early interventions.2122 There is growing awareness of the importance of early intervention in psychosis, especially in adolescents.2324 Recently, internet overuse has become a serious problem among adolescents in Asian countries.2526272829 While Japan succeeded in reducing the total number of completed suicides to less than 300,000 per year,30 the rate of suicide in teenagers was unchanged.313233 One of the reasons for the continued high adolescent suicide rate might be the widespread and growing use of smartphones that could serve as a vehicle for on-line or cyber-bullying.3435 School refusal (futoukou in Japanese) is a problem that is relatively unique in Japan and that often requires medical intervention.3637383940 A nationwide survey conducted by the Ministry of Education, Culture, Sports, Science and Technology (MECSST) in 2015 reported that the rate of school refusal was 2.76% among junior high school students in Japan.41 In this context, MECSST defined school refusal as a protracted school absence (without documented need to receive medical care), typically more than 30 days per year, caused by psychological factors such as fear, anxiety, anger, and sense of refusal. Continuous avoidance of social situations in school may result in severe social withdrawal, named hikikomori, in adulthood.4243444546474849 All of these mental health problems typically occur in childhood or adolescence and increase societal demands for child and adolescent psychiatry services in Japan.
AIM AND METHODS OF THIS REVIEW
The authors of this review paper are primary and supporting members of the Consortium on Academic Child and Adolescent Psychiatry in the Far East (CACAP FE).50 The multinational survey conducted by CACAP FE revealed that, although Japan has advanced medical technology and an overall high quality of care in medicine, CAP remained unrecognized as an established subspecialty, and there were no national guidelines for CAP training. To address the significant shortages of youth mental health services in Japan, the authors chose to further describe, via this paper, the underlying challenges and potential solutions.
Because CAP appears to have had the longest history of establishment as a specialty in the United States and Europe, and also because Japan has been significantly influenced by training and service models from these places, we chose to also include, in this review, and update on the current status of CAP training and services in the United States and Europe.
CURRENT GAPS IN CHILD AND ADOLESCENT MENTAL HEALTH SERVICES IN JAPAN
The 2.76% among junior high school students in Japan translates into 95,000 youth, excluding those identified with an illness. Furthermore, 68.4% of these youth stay out of for over one year.41 The students included in these high numbers are not receiving treatment–notwithstanding the fact that they had reasons to withdraw from school. It is clear that better prevention programs are needed to address the issue.
Furthermore, in Japan, the “school counselor” is deployed in over 75% of all junior high schools.51 Their defined role is to optimize child welfare by establishing a connection between schools and mental health services. In view of this fact, it appears that the rate of withdrawn students who do not receive mental health services–notwithstanding the existence of a theoretical mechanism to facilitate referrals–is unacceptably high.
Bullying is a serious concern identified in Japanese schools.49525354 The Japanese government reported that the number of bullying incidents was about 188,000.55 Although the victims are provided with support, no interventions for the perpetrator exist. There likely are insufficient child and adolescent mental health service staff. Public education is not enough to counteract this serious and growing mental health problem.
In Shiga Prefecture, which is fairly representative of other prefectures, welfare agencies were consulted for over 5,000 children and adolescents in 2014. Among these youth, only 7% had consulted with mental health services, and only an additional 2% had been encouraged to consult with mental health services but had not yet done so.56 It appears that the system of cooperation between welfare and mental health services is not effective, as illustrated in Figure 1.
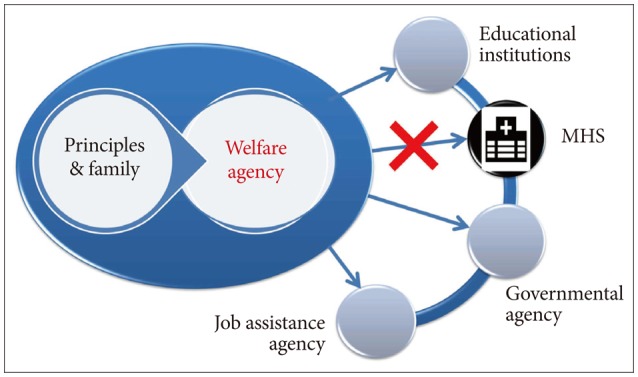
Failure of cooperation between welfare and mental health service (MHS).
In addition to stigma in child and adolescent mental health services,5758 child welfare agencies seem not to trust them, and likewise, there are not enough mental health providers to build and solidify trust through their services. In child welfare agencies' impression, following referrals to mental health services, the rate of “improved and the problem was solved” as an outcome is only 18%, and the cumulative rate of “no change” and “worsened” as outcomes is 38%.56
It appears that, currently in Japan, the quality and accessibility of mental health services are not sufficient, and due to a lack of information, there is a fundamental misunderstanding of mental health services' role and a lack of skill development in this area (Figure 2).
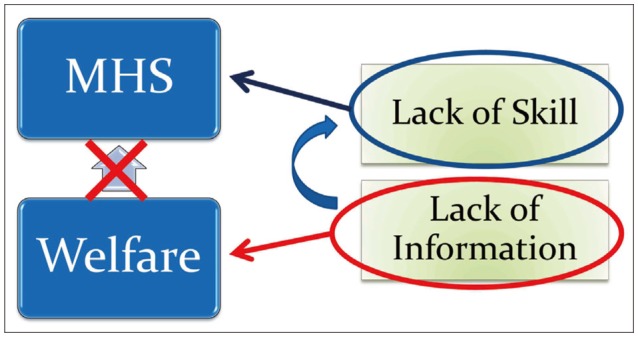
Lack of information diminishes cooperation between welfare and MHS. MHS: mental health service.
CHILD AND ADOLESCENT PSYCHIATRIC TRAINING AND WORKFORCE CHALLENGES IN JAPAN
Unfortunately, child and adolescent psychiatry (CAP) has not been a formally established specialty in Japan. CAP is considered a subspecialty of Psychiatry and Pediatrics.159
To date, there exists no standardized training program of CAP in Japan. Because each training hospital determines its own teaching curriculum, training content and clinical experience in CAP varies greatly among hospitals. However, there are several academic societies related to CAP that have respective certification systems for specialist in CAP: The Japanese Society for Child and Adolescent Psychiatry (JSCAP), Japanese Society for Adolescent Psychiatry (JSAP), Japanese Society of Pediatric Psychiatry and Neurology (JSPPN), and Japanese Society of Psychosomatic Pediatrics (JSPP).
JSCAP certification requirements include: more than 5 years of clinical experience in medicine, including over two years in general psychiatry and over three years in CAP; submission of a list of 30 CAP cases seen in the preceding three years; and three case reports. The clinician certified by the JSCAP is regarded as a specialist in CAP in Japan when statistical data on the CAP workforce are presented.
According to data from the Japanese Ministry of Health, Labor and Welfare, about 5% of all medical doctors (about 300,000 in total) are psychiatrists. Among them only 289 are JSCAP-certified CAP specialists (JSCAP website; as of May 10, 2016). Japan, with a total population exceeding 120 million people, is facing a serious shortfall of child psychiatrists, despite increasing social demands and a need to increase the number of clinicians who deal with children's mental health problems. Clearly, there is a need to produce and retain a child and adolescent psychiatric workforce that can fully respond to current mental health needs.
As summarized by Hirota and colleagues,50 recognition of CAP as an official subspecialty and existence of systematized training did not necessarily depend on income levels among countries in Far East Asia. For example, at the time of writing, there were no national guidelines for CAP training in such high income countries as Japan and Singapore.160
Unfortunately, in Japan, the lack of basic structure in the specialty most likely contributes to lack of training facilities, lack of an adequate workforce, off-label use of medications, and ultimately lack of access to child and adolescent mental health services. Clearly, the training and certification system does not reflect the needs of the public.
The Japanese Society of Psychiatry and Neurology (JSPN) started a specialist accreditation system in 2006.616263 The requirements for application are as follows: 1) Clinical training exceeding three years under the supervision by certified instructors; 2) a logbook with a list of required case experiences signed by supervisors; 3) passage of a written examination; 4) passage of an oral examination; and 5) submission of case reports. For JSPN certification as a psychiatry specialist, trainees are required to experience at least two CAP cases (versus minimum 10 cases of schizophrenia, 5 of mood disorders, 4 of organic psychosis, 5 of neurosis and stress related disorders) and to submit one CAP case report.
Fifty-eight percent of the instructors for the JSPN psychiatry specialist system are based in private psychiatric hospitals, 14% in clinics, 15% in university hospitals, and 12% in public hospitals.62 In terms of age, 10% of the instructors are in their 30's, 33% in their 40's, 33% in their 50's, 18% in their 60's, 5% in their 70's, and 1% in their 80's.
In a survey on child and adolescent psychiatry practice, early-career psychiatrists in Japan indicated that, notwithstanding moderate interest in CAP (5.34 on a scale of 1–9), they had insufficient experience with (3.05) and knowledge of (3.43) CAP.1 Surveys of CAP interest indicated a decline in interest before (33.3% interest) and after (20.5%) one-year clinical training in general psychiatry and low ratings of CAP experience (3.46 on a 6-point scale).264 Surveys of clinical experience rated child and adolescent psychiatry lower than the other specialties (2.8 on a 5-point scale versus 3.2 to 4.0 for other areas, including schizophrenia, mood disorders, substance and alcohol, organic psychosis, neurosis and stress related disorders, and personality disorders).61 Overall, surveys found that during ordinary psychiatry training, psychiatric trainees will experience insufficient CAP cases. Furthermore, senior/supervising psychiatrists might need to teach in all psychiatric fields including CAP, even if they did not experience enough CAP cases in their own training or practice. It appears that psychiatry training with adequate CAP cases would be necessary to attract more early-career psychiatrists to CAP.
From the point of view of clinical education, it is important to think not only about training for young staff, but also about lifelong education (also known as CPE or continuous professional education) for practicing physicians. Currently, one can update one's certification only through attending congress meetings, which occur only five times in five years. The current Japanese training system has challenges and inadequacies both in the training of new specialists and in lifelong education.
COMPARISON WITH OTHER MODELS FOR CHILD AND ADOLESCENT PSYCHIATRIC TRAINING
Child and adolescent psychiatry has been established as a clinical subspecialty in the US, where it constitutes a major part of psychiatric practice. Systematic education and training and research opportunities are also widely available in this specialty. In the US, pathways towards child and adolescent psychiatric certification include traditional training programs (3 years of general psychiatry plus 2 years of CAP), integrated training programs (5 years of training in general psychiatry and CAP at the same time), triple-board programs (2 years of pediatrics, 1.5 years of general psychiatry, and 1.5 years of CAP), and post-pediatric portal programs (3 years of training in general psychiatry and CAP following completion of pediatrics residency). Required experiences for traditional CAP training include: didactic sessions, faculty preceptorship (2 hours, including 1 individual), formulation, pediatric neurology, developmental disorders, psychiatric emergencies, acutely/severely disturbed children and adolescents (4–10 months), consultation (medical, school, and legal), community systems, normal development, and outpatients from each age group (>1 year).
As reviewed by Mian et al.,65 child and adolescent psychiatry training and teaching in Europe66 and the United States has increasingly become more standardized. In the US, as specified by the Accreditation Council for Graduate Medical Education (ACGME),67 all CAP training programs must incorporate training and assessment in six major competency areas: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice.68 In Europe, notwithstanding variability in specific training pathways across countries,69 the European Union of Medical Specialists (UEMS) has outlined a standard CAP curriculum that includes a minimum length of three years, certain basic competency goals, and an approval and auditing process by relevant government authorities responsible for education and training.70
In response to the many burdens that still need to be overcome in providing adequate child mental health care, important initiatives in US are: 1) improving the assessment of and recognition of mental health needs in children, 2) promoting scientifically-proven and evidence based interventions, and 3) increasing access to and coordination of quality mental health care services. Furthermore, in response to the increased emphasis on quality and accessibility of care within graduate medical education (the Clinical Learning Environment Review, or CLER initiative), US child and adolescent psychiatric training programs have adopted: quality improvement programs with ongoing feedback about clinical outcomes, standardized curricula that teach and evaluate specific competencies using progressive methods such as problem-based learning or PBL,71727374 and training experiences in telepsychiatry and primary care integration models.75
UPCOMING NEW MOVEMENT OF CAP IN JAPAN AND OTHER RECOMMENDED SOLUTIONS
To solve current problems in child and adolescent psychiatry in Japan, we advocate for the development and establishment of a more standardized child and adolescent psychiatry training system that is akin to what exists in the US and that teaches and evaluates according to specific competencies.
Overall, the certification system will become more standardized, and a new semi-official license system will start in 2018. In 2011, the Investigative Commission for Medical Specialist was established in the Ministry of Health, Labor and Welfare. In 2014, the Japanese Medical Specialty Board was established, and now they are programming a new training system for every medical discipline, including child and adolescent mental health (CAMH). This programming will include not only initial certification but also lifelong education.
In collaboration with the Japanese Medical Specialty Board (JMSB), which includes psychiatry as one of its 19 approved specialties, the JSPN will initiate new post-graduate psychiatry training in 2018. To harmonize this significant movement in medicine, four CAP-associated academic societies, the JSCAP, JSAP, JSPPN, and JSPP, will unify their respective specialist certification systems to one official specialist certification: a specialist for child mental health. In the transitional period, applicants who have society-specific specialist certification and JSPN specialist accreditation or accreditation by the Japan Pediatric Society (JPS) can take lectures followed by written and oral examinations in order to be certified as a CAP specialist. This will be the great first step toward establishment of a uniform training program in CAP.
In the upcoming new training system, several teaching hospitals will create an alliance to educate psychiatry residents (Figure 3). Clinical training by rotating through various teaching hospitals and psychiatry clinics will increase the opportunities to be exposed to child cases with mental and/or developmental problems. We propose that the training consortium model will raise the standards of clinical practice and improve recruitment into the specialty. An increased workforce will, in turn, increase the availability of specialized clinical services that are currently in short supply (including inpatient child and adolescent psychiatric care) and will be available to teach and train subsequent generations of physicians.

In the new specialty training system starting in 2017, training hospitals make a group to provide a better training program. The union of hospitals with various subspecialties will make the training program substantial and increase the exposure to CAP cases. CAP: child and adolescent psychiatry.
Through standardizing care and education and ultimately improving workforce, we can raise the quality of mental health services. But is doing so enough? The problem of “lack of information” is still left. We propose to create a system to transparently share our treatment results to the public and government. The public are generally unaware of treatment efficacy and should be provided with the appropriate information. To document technical improvement, appropriate comparisons between therapists or clinics should be made.56
Mental illness is treatable, and the best outcomes occur with early identification and intervention. The tragic and costly consequences of unidentified and untreated mental illness in youth can be avoided by taking timely evidence based actions in partnership with others.
CONCLUSION
Despite increasing social demands, Japan has been facing a serious shortage of child and adolescent psychiatry (CAP) specialists. In this paper, we reviewed the current status of CAP training system in Japan. To avoid tragic consequences of unidentified and untreated mental illness in youth, we need to provide enough CAP workforce and appropriate accessibility to mental health services in partnership with the educational and child welfare systems. We advocate for the establishment and development of a standardized CAP training system that is similar to what exists in the US. In 2018, the Japanese Medical Specialty Board will initiate new specialty training system including psychiatry. The new movement in general psychiatry will accelerate the development of CAP training system.