Social Behavioral Problems and the Health-Related Quality of Life in Children and Adolescents with Epilepsy
Article information
Abstract
Objective
The purpose of this study was to investigate the impact of specific behavioral problems on the health-related quality of life (HRQOL) in children and adolescents with epilepsy.
Methods
Children and adolescents with epilepsy (n=92; age range=6–17 years) and their mothers completed questionnaires about behavioral problems, HRQOL, socio-demographics, and epilepsy-related variables. To determine significant predictor variables of the HRQOL, the stepwise regression analyses and partial correlations were performed to adjust for other behavioral problems and covariates.
Results
The analyses revealed that an increase in social behavioral problems and delinquent behavior was associated with a decrease in the HRQOL. Lower levels of maternal education and the number of antiepileptic drugs were also associated with a decline in the HRQOL; the HRQOL and social behavioral problems remained significantly correlated after adjusting for maternal education level, number of antiepileptic drugs, and non-social behavioral problems.
Conclusion
Parents and practitioners should provide intervention if behavioral problems, particularly social behavioral problems, are observed in children or adolescents with epilepsy.
INTRODUCTION
Epilepsy is a common chronic illness of childhood. Traditionally, clinicians have focused on treating the physical aspects of epilepsy; however, there are other factors, including psychological facets, which can also affect the health-related quality of life (HRQOL). Research using HRQOL assessments in chronic disease has had important implications for epilepsy management and overall outcomes. It has been found that children and adolescents with epilepsy have a lower HRQOL than healthy controls1 and an increased risk for maladjustment and poor quality of life (QOL) in different domains than do children with other chronic health problems, such as diabetes or asthma.234 Psychological or psychosocial problems, such as emotional, behavioral, or environmental problems and social stigma, are faced by children and adolescents with epilepsy.567
In a recent study, it was hypothesized that psychological co-morbidity, child characteristics, and environmental factors influence epileptic outcomes more than epilepsy-specific variables.8 Ferro et al.9 reported that behavioral and cognitive problems in children with epilepsy are the strongest predictive factors of the HRQOL. Studies have shown that the prevalence of behavioral problems in pediatric epilepsy ranges from 16% to 77%1011 compared with 9% in the general pediatric population.12 Thus, children with epilepsy and emotional or behavioral problems tend to have both a poor epilepsy outcome and reduced QOL. Stevanovic et al.13 and Adewuya and Oseni14 reported that depression and anxiety disorders were strong predictors of the QOL in children and adolescents with epilepsy. Malhi and Singhi15 found that total psychopathology scores were significant predictors of QOL in pediatric epilepsy.
While recent studies have investigated factors influencing the HRQOL, few studies have evaluated which particular behavioral problems contributing to the HRQOL in children and adolescents with epilepsy in Korea. The purpose of current study examined the impact of behavioral problems, socio-demographics, and epilepsy-related variables on the HRQOL of Korean children and adolescents with epilepsy and identified the behavioral problems associated with the HRQOL controlling other significant variables. In addition, we examined the differences in awareness of HRQOL between children and adolescents with epilepsy and their parents. The identification of specific behavioral problems with impact on life outcomes may assist parents and practitioners in recognizing and supplying appropriate interventions to increase the HRQOL for children and adolescents with epilepsy.
METHODS
Participants
Children and adolescents (n=92; age range=6–17 years), who had been diagnosed and treated for epilepsy, were recruited at the epilepsy clinics of Ewha Womans University Mokdong Hospital to participate in this study. Inclusion criteria, in addition to the clinical diagnosis of epilepsy, were: 1) elementary, middle, or high school students able to understand and answer the questionnaires and; 2) the absence of severe neurological impairments, sequelae of traumatic brain damage in brain magnetic resonance imaging (MRI), combined psychiatric disorders [e.g., psychotic disorder, autism spectrum disorder or attention deficit/hyperactivity disorder (ADHD)], mental retardation, or other chronic illness. The mothers of the participants were also included in the study.
To exclude cognitive problems and combined psychiatric disorders that could influence the HRQOL, children and adolescents with epilepsy tested the Korean-Wechsler Intelligence Scale for children and examined brain MRI scans. Also participants checked the Child Depression Inventory and Children's Manifest Anxiety Scale-Revised. Mothers of participants checked the Conner's Parent Rating Scales. And then, child psychiatrist interviewed participants who have combined psychiatric problems at a clinical level. Of the 122 children and adolescents screened, 5 with a full-scale IQ of lower 70 on the Korean-Wechsler Intelligence Scale for children, five with sequelae of traumatic brain injury in brain MRI, sixteen with ADHD on the Conner's Parent Rating Scales and psychiatric interview with child psychiatrist, and four with incomplete questionnaires were excluded.
Measures
After outpatient examination at epilepsy clinic, neurologist explained to the patients and their mothers the purpose of the study, obtained their informed consent, and administered a self-report questionnaire to the patients and their mothers, under guidance. The self-report questionnaires for children under the age of 13 were age appropriately adapted. A trained research nurse assisted children and adolescents in completing the self-report questionnaires when necessary.
Socio-demographic information, such as the level of maternal education, parent's marital status, and family income, was collected from the mothers. We also gathered information on epilepsy-related variables, such as age at epilepsy onset, epilepsy duration, type of seizure, etiology of seizure, frequency of seizures, and type and number of antiepileptic drugs from interview of neurologist and medical files.
The HRQOL of children and adolescents with epilepsy was assessed using the Health-Related Quality of Life in Children with Epilepsy questionnaire developed by Ronen.16 This HRQOL instrument was chosen due to its parallel measures for children (the Child Self-Report Scale) and parents (the Parent-Proxy Response Scale), which allows both child and parent perceptions of the QOL16; a few studies comparing child and parent report of the QOL have found that children and parents had different perspectives of the QOL for children with epilepsy.171819 The scales include the domains of Interpersonal/Social Consequences, Worries and Concerns, Intrapersonal/Emotional Issues, Epilepsy My Secret, and Quest for Normality.20 On the parent scale, Worries and Concerns include both present and future worries, which are not part of the child scale. The Quest for Normality domain, which is only present on the child scale, includes issues about the ability to live a normal life and treatment by peers and family. Each scale has five subscales with a possible score of 5–20 for each subscale. The total the HRQOL score is the sum of all the parent and child responses. Thus, the total score for both parent and child scales ranges from 50 to 200, and higher total HRQOL scores reflect a better HRQOL. In this study, participants and their mothers checked the Child Self-Report Scale and Parent-Prosy Response Scale of the HRQOL in Children with Epilepsy questionnaire respectively.
The Child Behavior Checklist (CBCL) has been commonly used to evaluate behavioral problems in children and adolescents with epilepsy.521 The Korean version of the CBCL, which has been standardized in Korea,2223 was used to measure behavioral problems. The checklist is a 118-item scale on which parents rate their children's behavioral problems during the past 6 months. Each item is rated on a 3-point scale: 0 (not true), 1 (somewhat or sometimes true), and 2 (very true or often true). It is composed two subscales: the Broadband scale, which consists of internalizing problems, externalizing problems, and total behavior problems; and the Syndrome scale, which contains eight further subscales (anxious/depressed, withdrawn, somatic complaints, aggressive behavior, delinquent behavior, thought problems, attention problems, and social problems). Raw scores for the behavioral problems are converted to a standardized t score and normed for age and gender. In this study, mothers of participants completed the CBCL. The total behavior problem score, based on the t scores, included the internalizing, externalizing, thought, attention, and social problems subscales. For the syndrome scales, the at-risk range was defined as t>67 and the clinical range was defined as t>70.2223
Data analyses
T-tests and one-way analysis of variance (ANOVA) were also used to examine differences in the total HRQOL scores for discrete variables. To determine significant predictor variables of the HRQOL, Pearson correlation analysis was performed for continuous variables. Predictor variables included socio-demographic variables, epilepsy-related variables, and the eight subscales of CBCL.
Variables with statistically significant correlations (p<0.05) with the total HRQOL score were selected as independent variables for stepwise regression analyses. Three stepwise regression analyses (the total HRQOL, parent, and child scale scores) were performed to identify predictor variables from the behavioral, socio-demographic, and epilepsy-related measures. Qualitative dependent variables were converted to dummy variables for stepwise analysis. Eight partial correlations between each subscale of the CBCL and the total HRQOL were used to adjust for other behavioral problems and significant variables. Data were analyzed using Statistical Package for the Social Sciences (SPSS 20.0; SPSS Inc., Chicago, IL, USA); significance was set at 0.05.
RESULTS
Socio-demographic and epilepsy-related data
The socio-demographic and epilepsy-related characteristics of the participants are shown in Table 1. The main antiepileptic drugs used included sodium valproate, carbamazepine, lamotrigine, and topiramate. Among the socio-demographic and epilepsy-related variables, there were two significant associations with the HRQOL: maternal education level (p=0.014) and number of antiepileptic drugs (p=0.012). A low maternal education level and an increased number of antiepileptic drugs were associated with a decline in the HRQOL of children and adolescents with epilepsy.
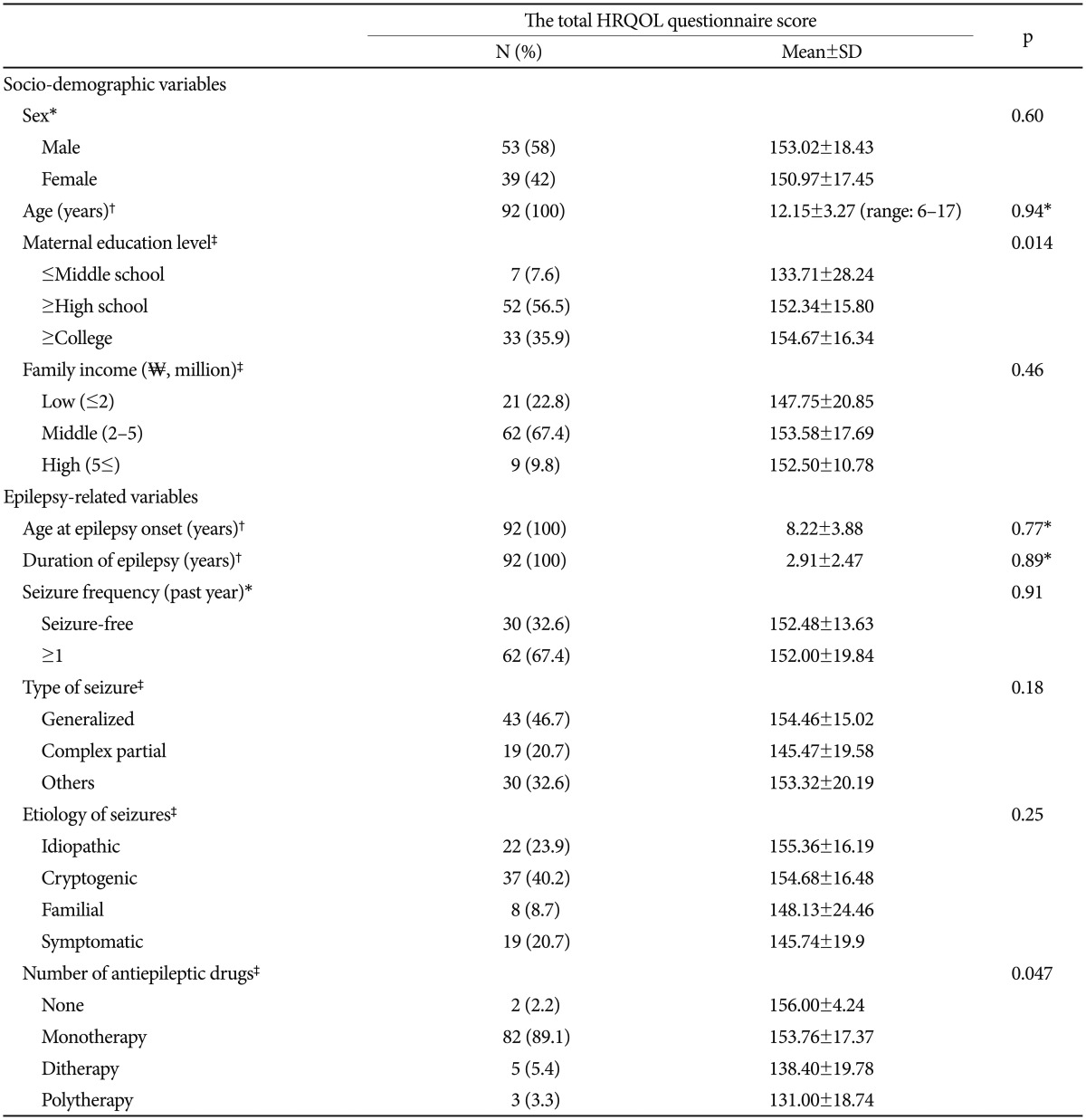
Socio-demographic and clinical characteristics of participants (N=92)
The Health-Related Quality of Life and Child Behavior Checklist scores
Table 2 shows the total and subdomain scores of the HRQOL questionnaire. There were no significant differences between the mean score of parent and child scales except in the intrapersonal/emotional subdomain. Mothers rated children's intrapersonal/emotional QOL higher than the children and adolescents with epilepsy did.
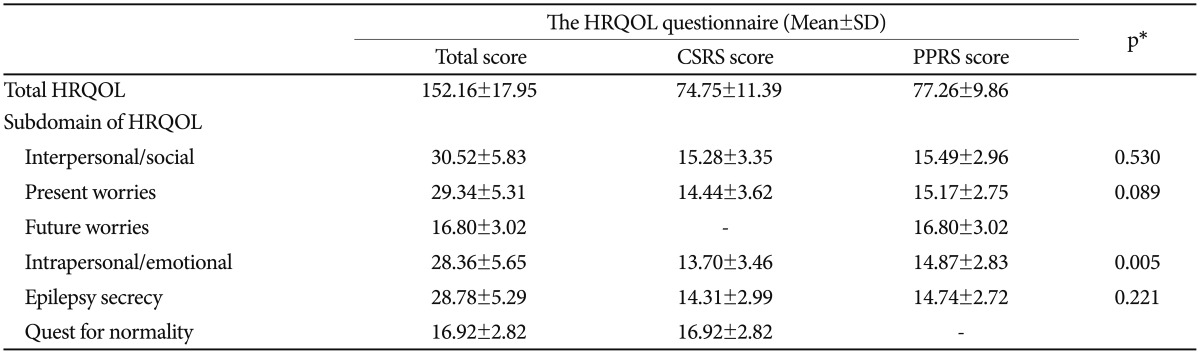
The total and 6 subdomains scores of the HRQOL questionnaire
The mean t scores for each of the eight subscales of the CBCL are in Table 3. There were moderate negative correlations between all eight subscales of the CBCL and the HRQOL questionnaire; this indicated increases in behavioral problems were associated with a decrease in the HRQOL.
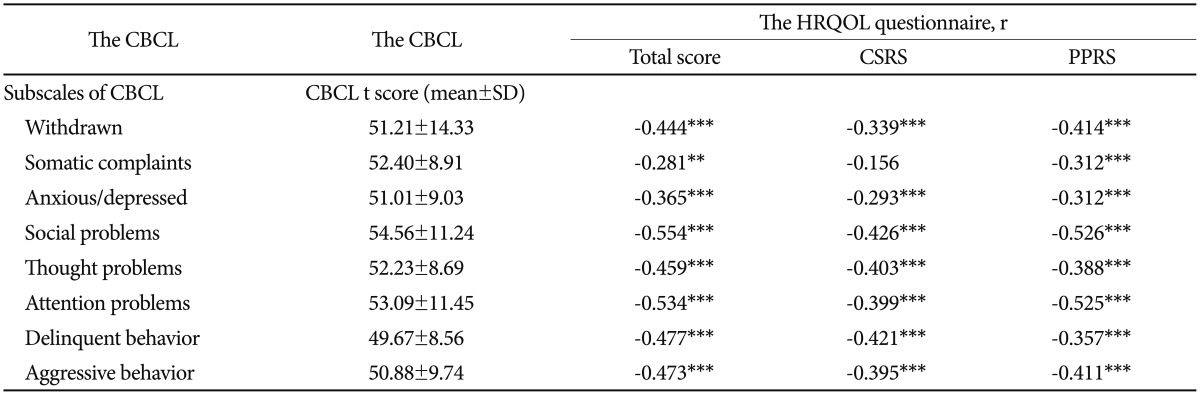
Correlations between the 8 subscales of CBCL and the HRQOL questionnaire
The correlations between the six subdomains of the HRQOL and the eight subscales of the CBCL, presented separately for child and mother reports, are shown in Table 4. Almost all behavioral problems were negatively correlated with the HRQOL with the exception those in the epilepsy secrecy domain on the child scale and present worries and epilepsy secrecy on the parent scale.
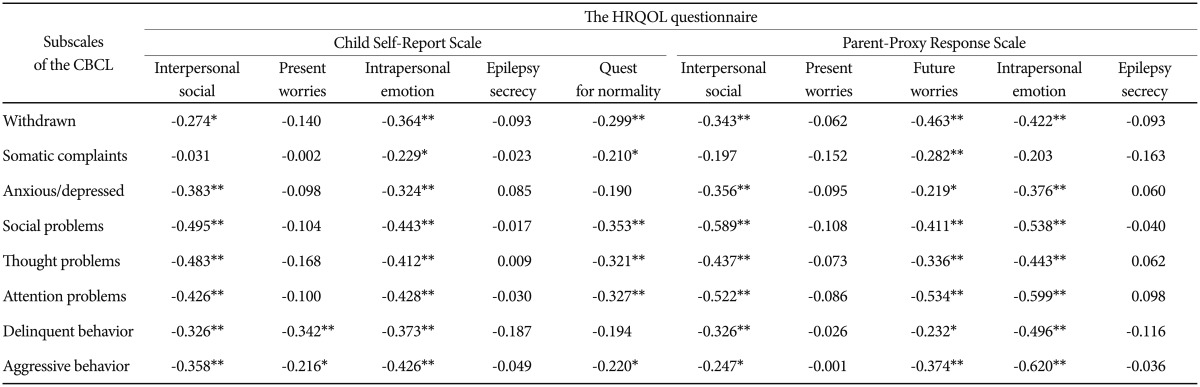
Correlations between for 6 subdomains of the HRQOL questionnaire and 8 subscales of the CBCL
Significant variables associated with the health-related quality of life scores
Partial correlation analysis adjusting for the significant predictors, maternal education level, and the number of antiepileptic drugs, showed the eight subscales of the CBCL had moderate negative correlations with the total HRQOL score: withdrawn (r=-0.387, p<0.001), somatic complaints (r=-0.254, p=0.018), anxious/depressed (r=-0.339, p=0.001), social problems (r=-0.483, p<0.001), thought problems (r=-0.388, p<0.001), attention problems (r=-0.467, p<0.001), delinquent behavior (r=-0.413, p<0.001), and aggressive behavior (r=-0.424, p<0.001). Only social behavioral problems had a significant negative correlation with the total HRQOL (r=-0.237, p=0.035) after controlling for all other behavioral problems, maternal education level, and the number of antiepileptic drugs.
Stepwise regression analysis revealed that social behavioral problems, delinquent behavior, and maternal education level were significant predictors of the variation in the total HRQOL scores. The scale for children and adolescents showed similar pattern (Table 5). Social behavioral problems were a strong predictor of the HRQOL, and accounted for these accounted for 29.8%, 26.8%, and 17.2% of the variance on the total, parent scale, and child scale scores, respectively.
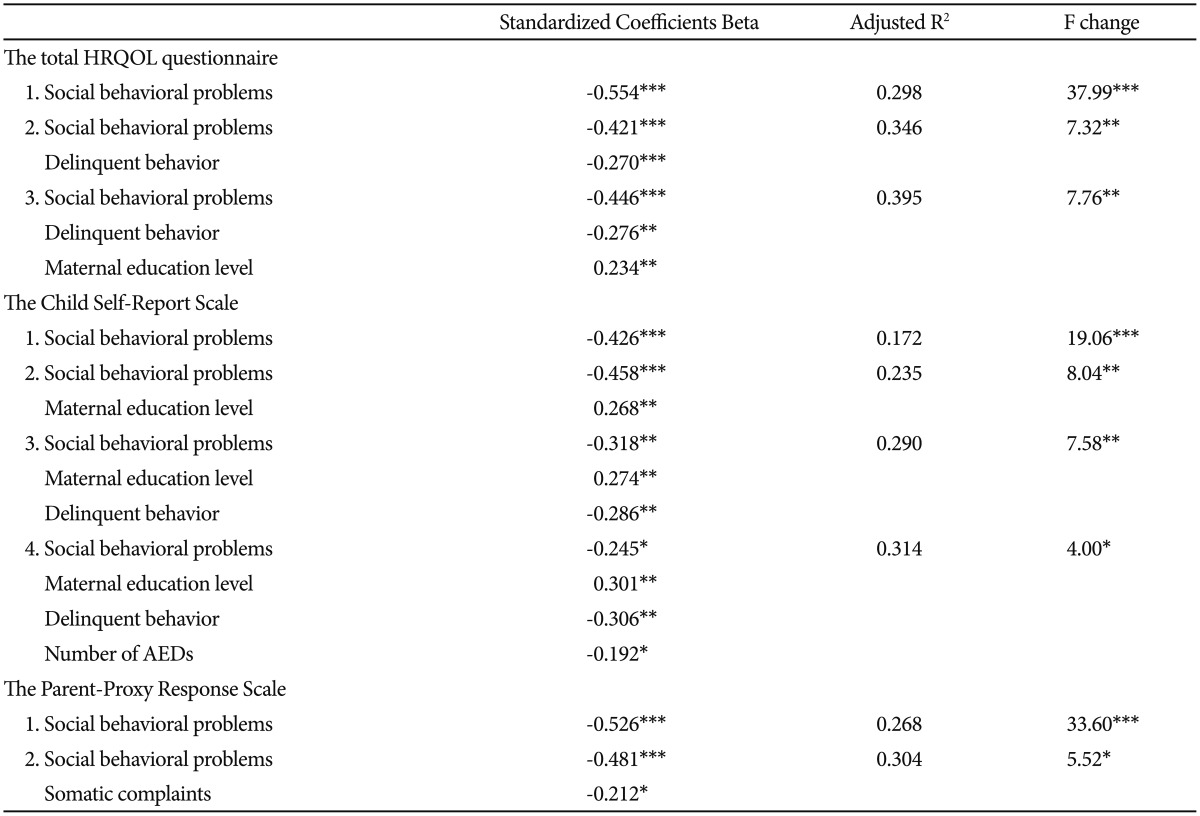
The 3 stepwise regression analyses for significant predictors of the HRQOL questionnaire
DISCUSSION
The present study found significant negative correlations between the HRQOL in Children with Epilepsy and behavioral problems. The regression analysis identified social behavioral problems, delinquent behaviors, and maternal education level as significantly independent contributors to the variance in the HRQOL of children and adolescents with epilepsy. Children and adolescents also reported a significant association between the number of antiepileptic medications and the HRQOL. Mothers reported that social behavioral problems and somatic complaints were significantly associated with the HRQOL.
We found that increased social behavioral problems appear to significantly impact the HRQOL of children and adolescents with epilepsy. This category included statements such as "acts too young for his/her age" and "socially immature and unsociable." Children's social functioning has been suggested as the best indicator of current and future behavioral and emotional problems24; an increased frequency of maladjustment, lower social skills, and social problems have been reported in pediatric epilepsy.42526 Moreover, these problems were relatively more likely to affect children with epilepsy than their siblings or children with other chronic conditions.11 Our findings are consistent with previous results showing that children with epilepsy have more social problems and a lower QOL.27 Children with epilepsy may suffer from social difficulties and other attendant problems, such as emotional, thought (lower self-concept or negative attitude toward epilepsy), adjustment (concealment of their condition or avoidance of age-appropriate activities), interpersonal/social, or cognitive problems.1027282930313233343536373839 In particular, developmental tasks of school-age children are engaging with their peers and growing social skills. And socioculturally, Asians has socially oriented subjective well-being, while Euro-Americans have individually oriented subjective well-being.40 In recent cross-cultural study to evaluate differences in the life satisfaction between Korean and U.S. adolescents, satisfaction with school contributed significantly to global life satisfaction only for Korean adolescents.41 Therefore, these complex problems and factors may inhibit development and contribute to a decreased HRQOL for children and adolescents with epilepsy.
Our findings suggest that delinquent behavior and the level of maternal education are associated with the HRQOL; however, the explanatory power of these variables was relatively small. Similar to the results of other studies,342 delinquent behavior was relatively uncommon in our participants. Delinquent behaviors included having friends who are perceived as having a negative influence, lying, school refusal, and running away from home. Disruptive behaviors in children with epilepsy appear to have a negative impact on their overall functioning and may lead to a decrease in the HRQOL. Therefore, these findings suggest that clinicians need to be aware of the presence of delinquent behaviors in this population, even though these are relatively uncommon in children and adolescents with epilepsy.
In this study, low maternal education level was associated with a decreased HRQOL; this finding is consistent with the results of a previous studies15 that reported a low levels of in mothers' with children or adolescents with epilepsy was associated with a lack of knowledge, negative attitude, and uncertainty about epilepsy.4344 Therefore, mothers with low education may have inadequate parenting skills or low confidence and mastery in managing the epilepsy and behavior of their children, which may have a negative influence on children and family.
The polytherapy showed significantly negative association with HRQOL only in children and adolescents' report. This finding is consistent with previous studies that found an association between the QOL of children with epilepsy and the number of antiepileptic drugs.145 In recent studies, smaller number of medications showed a strong positive impact on quality of life in Korean pediatric epilepsy,46 and receiving polytherapy were independent factors predicting Korean adolescents with epilepsy's perception of stigma.47
Social behavioral problems, maternal education level, delinquent behavior, and the number of antiepileptic drugs demonstrated a significant negative impact of the HRQOL reported by the children and adolescents; these variables accounted for 31.4% of the variation in the HRQOL score. The pattern of these results was similar to the total HRQOL score. On the parent report, social behavioral problems and somatic complaints were the only significant predictors of the HRQOL. Delinquent behavior and level of maternal education were not significantly associated with the parent report scale, unlike their role as predictors of the total HRQOL and the child quality of life scales. In previous studies, internalizing problems, such as symptoms of depression and anxiety, were emphasized as strong predictors of the HRQOL for children and adolescents with epilepsy,1314 whereas externalizing or other behavioral problems were not addressed relatively.
There were some differences observed between the parent and child HRQOL ratings in this study, which may have important clinical implications. First, discrepancies between parent and child reporting may reflect a different understanding or point of view of behavioral problems. The externalizing problems, delinquent and aggressive behaviors, have correlations with present worries only in the child report. Mothers of children and adolescents with epilepsy rated the intrapersonal/emotion subdomain of the HRQOL higher than their children did. Thus, the emotional problems may be hiding other problems and delinquent behaviors that can be overlooked by mothers. At the same time, the somatic complaints could be overestimated in the parent's perspective, although even the higher parent ratings did not have a significant influence on the child's HRQOL score. These gaps could represent a double hardship for children and adolescents with epilepsy.
This study has several limitations. First, the subjects were recruited from a single university hospital; therefore, the results may not be generalizable to other settings. Second, there are various methodological limitations: the study was cross-sectional, had a small number of participants, no comparison group, and a heterogeneous seizure group. Third, our study used the CBCL as the tool to evaluate behavioral problems, instead of a more structured instrument. Although the CBCL is a well-standardized measure of behavioral problems in children and is commonly used in pediatric epilepsy, it has been reported to have a false-negative rate of 10% and a false-positive rate of 20% compared with the Diagnostic Interview Schedule for Children.48 Finally, the collinearity of the variables, especially among subscales of the CBCL, suggests that the results should be interpreted with caution. We assessed collinearity with the variance inflation factor and condition index in a regression model; all variance inflation factors were less than 2.0, which suggest there was no significant collinearity among predictors of the HRQOL.
Despite all these limitations, to close attention for the effects of specific behavioral problems on the HRQOL in children and adolescents with epilepsy in Korea. Especially, factors that impact on the behavioral problems, such as cognitive problems or ADHD, were excluded thorouthly. In addition, we estimated the HRQOL using a self-report measure that allowed independent ratings by children and a proxy report from their parents. This study demonstrated that social behavioral problems were significantly associated with the HRQOL for children and adolescents with epilepsy, even when other factors were controlled. Assessment and management of possible behavioral problems, especially social behavioral problems and delinquent behavior, are important to increase the HRQOL for children and adolescents with epilepsy. Targeted psychosocial interventions should be considered for children with epilepsy and social or delinquent behavior problems. In addition, appropriate education and support for parents of children with epilepsy is necessary and parents should be considered as part of the HRQOL management team for children and adolescents with epilepsy.