Development of Korean Version of PTSD Checklist for DSM-5 (K-PCL-5) and the Short Form (K-PCL-5-S)
Article information

Abstract
Objective
This study presents the reliability and validity of the Korean version of the post-traumatic stress disorder (PTSD) checklist for the Diagnostic and Statistical Manual for Mental Disorders-fifth edition (DSM-5) (K-PCL-5) and the short form (K-PCL-5-S).
Methods
Seventy-one subjects with PTSD, 74 subjects with mood or anxiety disorders, and 99 healthy controls were enrolled. The Korean version of the Structured Clinical Interview for DSM-5-research version was used to confirm the presence of PTSD. The Beck Depression Inventory-II (BDI-II), Beck Anxiety Inventory (BAI), Impact of Event Scale-Revised (IES-R), and Spielberger State Trait Anxiety Inventory (STAI) were used to evaluate the concurrent validity of the K-PCL-5 and K-PCL-5-S.
Results
It presented good internal consistency (Cronbach’s α=0.93) and test-retest reliability (r=0.90). The K-PCL-5 and K-PCL-5-S were highly correlated with the BDI-II, BAI, IES-R, STAI-S, and STAI-T. The suggested cutoff score for PTSD was 33 for the K-PCL-5 with a sensitivity of 88.51 and specificity of 89.09, and 6 for the K-PCL-5-S with a sensitivity of 91.95 and specificity of 89.09. The data were best explained with a one-factor model.
Conclusion
These results demonstrated the good reliability and validity of the K-PCL-5 and K-PCL-5-S, and their suitability as simple tools for PTSD assessment.
INTRODUCTION
The post-traumatic stress disorder checklist (PCL) is one of the most widely used self-report scales for screening and measurement of symptom severity in post-traumatic stress disorder (PTSD) in research as well as clinical practice [1,2]. The PCL was revised in accordance with changes in the diagnostic criteria of PTSD in the fifth edition of the Diagnostic and Statistical Manual for Mental Disorders-fifth edition (DSM-5) [3]. In the DSM-5, PTSD is described in four categories: intrusion, avoidance, negative alterations in cognition and mood, and alterations in arousal and reactivity [4]. Previous PCL existed in three versions depending on the responding populations (that is, civilians, veterans, and specific stressful experiences), but it was changed to single type, PTSD checklist for the DSM-5 (PCL-5).
Although PCL‐5 has good psychometric properties [2,5], one weakness is its length; the scale has 20 items and it takes approximately 5–10 min to complete [6]. This is not a problem when only measuring the severity of PTSD symptoms. The large number of items and long test time may interfere with screening when evaluating other comorbid mental disorders together. To meet this demand for brevity, several short-forms of PCL-5 have been created [7,8]. In particular, as a short-form PCL-5 (PCL-5-S) by Zuromski et al. [8] was developed using both machine learning and conventional scale development methods, it is highly likely to be used.
PCL-5 showed sound psychometric properties in studies conducted on various population groups, which is sufficient compared to studies with a previous version of the PCL [9-11]. However, cut-off points for PCL-5 vary from study to study, ranging from 33 to 38 [2,5,12,13]. In Korea, one study on the reliability and validity of PCL-5 was conducted for the elderly Korean veterans of the Vietnam War, but the findings were not generalizable because the target population was elderly combat veterans [14]. In addition, there have been studies to examine the reliability and validity of the PCL-5 in the general population. The studies used non-clinical samples, and PTSD symptoms were not assessed with interview-based instruments such as the Clinician-Administered Post-traumatic Stress Disorder Scale for DSM-5 (CAPS-5) or the Structured Clinical Interview for DSM-5-research version (SCID-5-RV) [15,16].
In this study, we aimed to develop and validate the Korean version of PCL-5 (K-PCL-5) and the short-form PCL-5 (KPCL-5-S). After translating K-PCL-5 into Korean while maintaining its basic structure, we assessed the validity and reliability of the K-PCL-5 and K-PCL-5-S to test their usefulness in Korean patients with PTSD.
METHODS
Subjects
We used data from the study on the reliability and validity of the Korean version of CAPS-5 [17]. A total of 274 participants were recruited from eight medical institutions throughout Korea, from February 2016 to March 2017. The 274 participants comprised 71 with PTSD, 74 with mood disorder or anxiety disorder as a psychiatric control group, and 99 as a healthy control group. PTSD and other psychiatric disorders were diagnosed using SCID-5-RV [18], which is a semi-structured interview guide for making DSM-5 diagnoses including depression, anxiety, and PTSD. Interviewer training consisted of lectures on the SCID-5-RV and related questionnaires, observation of an evaluation performed by an experienced psychiatrist, and group evaluation of videos of patients with PTSD. The diagnoses of the subjects in the psychiatric control group included major depressive disorder (n=44), panic disorder (n=6), and generalized anxiety disorder (n=24). The healthy control group included 88 randomly selected individuals who visited the institutions for regular health screening. All the healthy controls demonstrated a lack of history of psychiatric disorders in SCID-5-RV.
The exclusion criteria for psychiatric disorders included age lower than 18 or higher than 70 years, current or past diagnosis of psychotic disorders, and unable to complete K-PCL-5. To assess test-retest reliability, a non-random sample of participants with PTSD who agreed to the second assessment was included.
Measurement instruments
PCL-5 is a 20-item self-report questionnaire developed by Weathers et al. to measure PTSD symptoms in DSM-5 [6]. PCL-5 is helpful for individual screening and diagnostic evaluation of PTSD and is suitable for the purpose of observing PTSD symptom changes. For example, symptoms during past months experienced by the respondents were rated on a 0 to 4 Likert scale, with a total score ranging from 0 to 80.
Zuromski et al. [8] developed PCL-5-S using both machine learning and conventional scale development methods. It includes one item assessing each DSM‐5 criteria, B‐E: B3 (suddenly feeling or acting as if the stressful experience were happening again), C2 (avoidance of external reminders of the stressful experience), D6 (distant or cutoff from other people), and E1 (irritable or aggressive behavior) [3]. Thresholds in the PCL-5-S scale were selected to make prevalence estimates equivalent to those using the full PCL‐5. At a threshold of 6, the PCL-5-S would detect an even higher proportion of cases using the conservative PCL-5 threshold of 38 with an even lower false-positive rate [8].
After obtaining permission from the National Center for PTSD, three bilingual psychiatrists and one psychologist initially translated PCL-5 into English and Korean, followed by a process of back translation and revisions. Two other bilingual Korean psychiatrists and one psychologist performed a blind back translation. Finally, a translation committee, which consisted of five Korean psychiatrists, one Korean language and literature professor, and one psychologist, created the final version of K-PCL-5 [19].
The Korean version of SCID-5-RV (K-SCID-RV) was used to assess convergent validity of K-PCL-5. We used SCID-RV as the gold standard assessment of DSM-5 PTSD. SCID-5-RV is a semi-structured interview guide for making DSM-5 diagnoses of depression, anxiety, and PTSD. It was administered by trained mental health professionals who were familiar with the DSM-5 classification and diagnostic criteria.
The Beck Depression Inventory-II (BDI-II) [20], Beck Anxiety Inventory (BAI) [21], Impact of Event Scale-Revised (IES-R) [22], and Spielberger State Trait Anxiety Inventory (STAI) [23] were also used to assess the correlations with the scores of the KPCL-5 and K-PCL-5-S. BDI-II, a 21-item self-administered questionnaire, was designed to evaluate the severity of depression and the BAI with 21 items to evaluate the severity of anxiety. IES-R, a 22-item self-reporting questionnaire composed of eight questions for intrusion, eight for avoidance, and six for hyperarousal, was used to assess the severity of PTSD symptoms. The STAI, with 40 self-check questions, was developed to assess the severity of state and trait anxiety. The Korean versions of the BDI-II, BAI, IES-R, and STAI have previously been shown to exhibit excellent psychometric properties, and their internal consistency coefficients (Cronbach’s alpha) were reported to be 0.85 [24], 0.90 [25], 0.76 [26], and 0.91 [27], respectively.
Statistical analyses
Among the PTSD, psychiatric control, and normal control groups, demographic variables and clinical characteristics were compared using analysis of variance (ANOVA) or χ2 analyses, depending on the type of variables. To measure the internal consistencies of K-PCL-5, Cronbach’s alpha coefficients were computed, and the item-total correlation coefficients of these scales were measured to confirm whether all items on these scales also exhibited internal consistency. Test-retest and inter-rater reliability were calculated using intraclass correlation coefficients. Test-retest reliability was evaluated by the same interviewers who performed the two testing sessions within five days. Pearson correlation coefficients were used to evaluate the concurrent validity of K-PCL-5, K-PCL-5-S, BDI-II, BAI, IES-R, and STAI. Exploratory factor analysis was performed using principal component analysis with varimax rotation to determine the factor structure of the K-PCL-5. The optimal cutoff scores of the K-PCL-5-S and the best predicted current PTSD by SCID-5-RV were estimated by receiver operating characteristic curve (ROC) analysis. To measure the diagnostic accuracy of K-PCL-5, K-PCL-5-S, and IES-R for PTSD, the area under the ROC curves (AUCs), standard errors, and 95% confidence intervals (CI) were calculated. Sensitivity, specificity, positive predictive value, negative predictive value, and overall efficiency were measured for each threshold score of K-PCL-5 and K-PCL-5-S.
Analyses were performed using SPSS version 23.0 (SPSS, IBM Corp., Armonk, NY, USA). Statistical significance was set at p<0.05.
Ethics statement
This study was approved by the public Institutional Review Board of the Ministry of Health and Welfare of Korea (P01-201508-21-002). All subjects were informed of the study purpose and methods, and provided written informed consent.
RESULTS
Demographics and clinical characteristics
The mean ages of the PTSD, psychiatric control, and normal control groups were 46.9±14.3, 43.7±12.1, and 44.6±9.2 years, respectively. The numbers of male in the three groups were 42 (60.0%), 34 (45.9%), and 37 (37.4%), respectively. No significant differences were found in age (F=1.433, p=0.241), although a significant difference in sex ratio was found among the three groups (χ2= 8.452, p=0.015). There were no significant differences in marital status among the three groups. The mean duration of symptoms in the PTSD group was 22.31± 29.17 (range, 1.10–126.67) months. The worst traumas experienced in the PTSD group were serious accidents such as automobile or man-made disasters (n=51, 72.9%), physical assault (n=7, 10.0%), sexual abuse (n=6, 28.6%), combat experience (n=2, 2.9%), life-threatening medical disease (n=2, 2.9%), and witnessing an accident (n=2, 2.9%).
Reliability
Cronbach’s α was used to evaluate the internal consistency of the K-PCL-5 in the 71 patients with PTSD. The internal consistency for the K-PCL-5 total score was 0.93 at baseline. The alpha coefficients for intrusion, avoidance, cognition/ mood, and arousal/reactivity were 0.85, 0.59, 0.84, and 0.82, respectively. Based on the criterion of 0.30 as an acceptable corrected item-total correlation [19], all 20 items performed adequately (range, 0.62–0.88) (Table 1).

Item-total correlation and explorative factor analysis of the items in the Korean version of the PTSD checklist for DSM-5
Among the 71 participants with PTSD, 34 were recruited for the evaluation of test-retest reliability, which was determined to be 0.90 (p<0.001).
Validity
The total scores±standard error (SE) of the K-PCL-5 in the PTSD group, psychiatric controls, and normal controls were 47.10±16.42, 18.49±13.75, and 3.98±4.92, respectively. These values were significantly different according to ANOVA (F= 272.19, p<0.001). The total scores±SE of the K-PCL-5-S in the PTSD group, psychiatric controls, and normal controls were 9.33±3.77, 3.22±2.87, and 0.85±1.22, respectively. These values were significantly different according to ANOVA (F=214.94, p<0.001). Tukey’s post-hoc test showed significant differences among the three groups. These results showed the good construct validity of the K-PCL-5.
The total K-PCL-5 score correlated with the BDI-II (r=0.75, p<0.001), BAI (r=0.89, p<0.001), IES-R (r=0.93, p<0.001), STAI-S (r=0.14, p=0.029), and STAI-T (r=0.19, p=0.003). The total K-PCL-5-S score correlated with the BDI-II (r=0.73, p< 0.001), BAI (r=0.83, p<0.001), IES-R (r=0.88, p<0.001), STAIS (r=0.14, p=0.030), and STAI-T (r=0.19, p=0.002). Thus, the correlation of the K-PCL-5 was strong with the IES-R, relatively weak with the STAI-T, and intermediate with the BDIII (Table 2).

Pearson’s correlations in the Korean version of the PTSD checklist for DSM-5 (K-PCL-5): K-PCL-5-S, BDI, BAI, IES-R, and STAI in patients with PTSD
Factor analysis
Explorative factor analysis with varimax rotation on the items of the K-PCL-5 yielded one factor with an eigenvalue of 1.0 or higher (Table 1). The eigenvalue of factor 1 was 13.68, accounting for 68.38% of the total variance, and most of the variance was explained by factor 1. The explanatory variance of factor 1 was very high; therefore, it can be viewed as a single-factor structure. In the non-rotated state, the factor loading of each item for factor 1 was 0.62 to 0.88.
Diagnostic accuracy and optimal cutoff scores
Figure 1 shows the ROC curve of the K-PCL-5, K-PCL-5-S, and IES-R compared with the SCID-RV PTSD as the gold standard. The AUC of the K-PCL-5 was 0.95 (SE 0.13, 95% CI 0.92–0.97). The AUC of the K-PCL-5-S was 0.94 (SE 0.16, 95% CI 0.91–0.97). Lastly, the AUC of IES-R was 0.95 (SE 0.13, 95% CI 0.93–0.98).
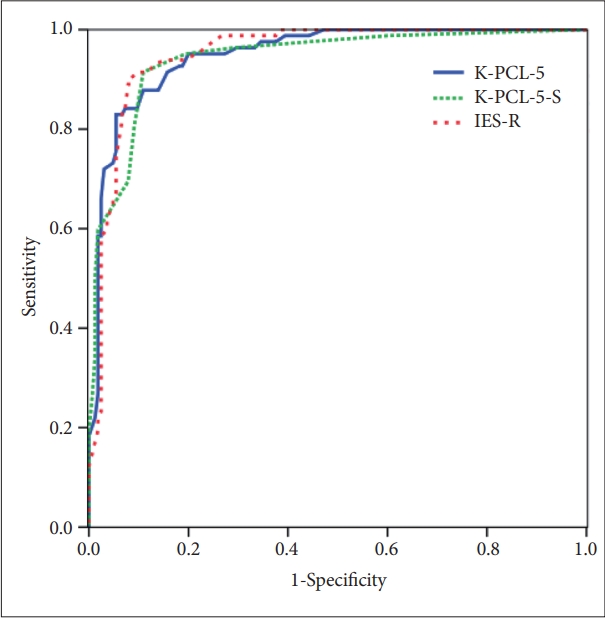
ROC curve analysis depicting K-PCL-5, K-PCL-5-S, and IES-R. IES-R, Impact of Event Scale-Revised; ROC, receiver operating characteristic curve.
Table 3 shows the values of the accuracy indices (sensitivity, specificity, positive predictive value, and negative predictive value) according to various cutoff scores of the K-PCL-5 and K-PCL-5-S. In this study, the cutoff of 33 of the K-PCL-5 had a sensitivity of 88.51 and specificity of 89.09. Moreover, in the case of the K-PCL-5-S, its cutoff of 6 had a sensitivity of 91.95 and specificity of 89.09.

Comparing the diagnostic utility of the Korean version of the PTSD checklist for DSM-5 (K-PCL-5) cutoff score with the KPCL-5-S cutoff score
DISCUSSION
This was a cross-sectional multicenter survey to test the psychometric properties of the K-PCL-5. K-PCL-5 is a useful tool that should be standardized for PTSD studies and the clinical field because it measures the severity of PTSD symptoms. K-PCL-5 and K-PCL-5-S showed excellent internal consistency, test-retest reliability, concurrent validity, and criterion-related validity.
First, K-PCL-5 presented high reliability. The internal consistency of K-PCL-5 was demonstrated by a Cronbach’s α of 0.93, which was in the excellent range [21-23]. Each coefficient of the four PTSD symptom clusters was within the optimal range. The test-retest reliability of K-PCL-5 was 0.90. The test-retest interval in this study was two weeks. In clinical situations, longer test-retest intervals may cause greater changes in PTSD symptoms. PTSD in most of the participants included in this study was chronic, with a mean duration of symptoms of 4.2 years.
In the comparison of the three groups in severity scores of K-PCL-5, the PTSD group showed the highest average, followed by the psychiatric control and normal groups. K-PCL-5 includes cognition/mood items and other items such as intrusion, avoidance, and arousal/reactivity. In addition, PTSD symptoms are known to be partially correlated with depressive or anxiety symptoms; therefore, the total severity scores of the K-PCL-5 of the psychiatric control group were higher than those of the normal control group [10].
K-PCL-5 was highly correlated with the IES-R due the similar constructs, but less strongly correlated with other less relevant measuring constructs, such as depressive and anxiety symptoms. These correlations demonstrated the reasonable discriminant validity of this task as a measure for assessing PTSD symptoms.
In the factor analysis of K-PCL-5, one factor was generated through the explained variance (68.4%). This is similar to the results of the original PCL-5 study [28]. In the original PCL-5 study, the eigenvalue of one factor was 12.2, accounting for 61% of the total explanatory value [28].
The AUC calculated to evaluate the sensitivity and specificity of K-PCL-5 was 0.95. The cutoff value of the K-PCL-5 was 33. Studies on the cutoff value of PCL-5 have shown various results. Hoge et al. [13] reported that the cutoff of the PCL-5 was 38. Similarly, Belvins et al. [2] reported 37 and Wortmann et al. [5] and Bovin et al. [12] suggested the cutoff to be 33. In a study on the elderly who participated in the Vietnam War in Korea, the cutoff of PCL-5 was 37. [14] According to the study, the cause of the difference might be due to the difference in time after trauma exposure and severity of the exposed trauma.
The AUC calculated to evaluate the sensitivity and specificity of the K-PCL-5-S was 0.94, which is a high value. The cutoff value of the K-PCL-5-S was 6. The original study of the PCL-5-S did not suggest a cutoff score [8]. It reported that the threshold of 6+ of the PCL-5-S would detect an even higher proportion of cases using the conservative PCL‐5 ≥38 thresholds with an even lower false positive rate.
The present study has several limitations. First, the number of index traumatic events in the PTSD group was relatively small; thus, no difference among PTSD symptoms could be distinguished according to each index traumatic event. Second, the proportion of male in the PTSD group was higher than that in the other groups. Female are more vulnerable to PTSD and more likely to develop PTSD than male [29]; therefore, a future study with a slightly higher proportion of female with PTSD will be more representative. Finally, the normal group did not experience any traumatic event that satisfied the DSM-5 criteria for PTSD.
In conclusion, K-PCL-5 and K-PCL-5-S have good psychometric properties and may be used as reliable and valid instruments for screening and assessing PTSD according to the DSM-5. More studies are needed to compare patients with PTSD and controls in the same index traumatic event using K-PCL-5 and K-PCL-5-S.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
Daeho Kim, a contributing editor of the Psychiatry Investigation, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Author Contributions
Conceptualization: Won-Hyoung Kim, Joo Eon Park. Formal analysis: Won-Hyoung Kim, Joo Eon Park. Investigation: Young-Eun Jung, Daeyoung Roh, Daeho Kim, Joo Eon Park. Methodology: Won-Hyoung Kim, Joo Eon Park. Resources: Young-Eun Jung, Daeyoung Roh, Daeho Kim, Joo Eon Park. Software: Won-Hyoung Kim, Joo Eon Park. Supervision: Joo Eon Park, Daeho Kim, Jeong-Ho Chae. Validation: Joo Eon Park, Daeho Kim, Daeyoung Roh, Jeong-Ho Chae. Visualization: Won-Hyoung Kim. Writing—original draft: Won-Hyoung Kim. Writing—review & editing: Joo Eon Park, Daeho Kim, Daeyoung Roh.
Funding Statement
This work was supported by a grant from the Korean Mental Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HM15C1058).