Insomnia Disorder Among Coronavirus Disease Survivors: A South Korean Nationwide Cohort Study
Article information

Abstract
Objective
We investigated the prevalence and associated factors of insomnia disorder among survivors of coronavirus disease of 2019 (COVID-19).
Methods
This population-based cohort study used data from the National Health Insurance Service COVID-19 cohort database from January 1 to June 4, 2020. COVID-19 patients were defined as individuals whose test confirmed that they were infected, regardless of the severity, and survivors were defined as individuals who recovered from the infection.
Results
A total of 299,968 individuals were included in the final analysis, and 6,934 were considered as COVID-19 survivors, while the control group comprised 292,764 individuals. In the multivariable model after covariate adjustment, COVID-19 survivors had a 3.33-fold higher prevalence of insomnia disorder than the control group (odds ratio [OR]: 3.33, 95% confidence interval [CI]: 2.98–3.73; p<0.001). In the sensitivity analysis, the COVID-19 survivors with no specific treatment and the survivors with specific treatment were associated with a 3.16-fold (OR: 3.16, 95% CI: 2.77–3.59; p<0.001) and 3.89-fold (OR: 3.89, 95% CI: 3.17–4.78; p<0.001) higher prevalence of insomnia disorder than the control group.
Conclusion
In South Korea, 5.4% of COVID-19 survivors were diagnosed with insomnia disorder at 6 months follow-up. Thus, insomnia disorder is a public health issue for COVID-19 survivors.
INTRODUCTION
On March 11, 2020, the World Health Organization declared the coronavirus disease of 2019 (COVID-19) a global crisis [1]. Although vaccines are being administered since December 8, 2020 [2,3], it is a time consuming process to achieve herd immunity against the infection worldwide, because of the limited production volume and speed of administration of the vaccine. Therefore, COVID-19 is still considered a global health crisis.
Globally, approximately 2.2% of individuals diagnosed with COVID-19 have died due to the infection [4]; the remaining 97.8% recovered and have returned to regular life. Therefore, the sequelae of COVID-19 survivors have emerged as an important issue that could assist in enhancing the quality of life of the survivors [5]. Insomnia disorder, the most common type of sleep disorder, is a clinical condition often seen in hospitalized patients and outpatient clinics [6]. Its prevalence ranges from 35% to 50% in the United States [7] and 5.78% in South Korea [8]. Moreover, the increase in clinical insomnia disorder in the Chinese population has been observed as an impact of COVID-19 [9]. In China, the estimated immediate prevalence of insomnia disorder during the COVID-19 pandemic was reported as 20.05% [9]. Additionally, the prevalence of insomnia disorder during the COVID-19 pandemic has been reported to be 37.6% in the Greek, 19.1% in the French, and 50.4% in the Turkish population [10-12]. However, previous studies have focused on the prevalence of insomnia disorder among the general population, including medical staff, in addition to COVID-19 patients with a shorter follow-up period [9-12]. Therefore, the impact of COVID-19 on the development of insomnia disorder as a sequela among survivors has not yet been investigated. In South Korea, the National Health Insurance Service (NHIS) COVID-19 database (DB) has been developed to conduct medical research on COVID-19 patients in the country.
Using this database, we aimed to investigate the prevalence and associated factors of developing insomnia disorder among COVID-19 survivors in South Korea. We hypothesized that COVID-19 survivors might have a higher prevalence of insomnia disorder than other populations with some significant risk factors.
METHODS
Ethical statement
This population-based cohort study follows the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology [13]. The Institutional Review Board (IRB) of Seoul National University Bundang Hospital exempted the deliberation of the study protocol (X-2009-636-902). Furthermore, the NHIS data sharing service approved the use of data from the NHIS-COVID-19 DB (NHIS-2021-1-070). The requirement for informed consent was waived by the IRB as the data were extracted retrospectively using anonymized data derived from the NHIS-COVID-19 DB.
Database (NHIS-COVID-19 DB)
The Korea Disease Control and Prevention Agency (KDCPA) and NHIS collated the NHIS-COVID-19 DB for medical research purposes on June 26, 2020, and it was last updated by the NHIS on December 1, 2020. First, the KDCPA provided the data of all individuals whose polymerase chain reaction (PCR) test from January 1 to June 4, 2020, confirmed that they were COVID-19 positive. Individuals who were confirmed as COVID-19 positive were defined as COVID-19 patients regardless of the disease severity. The data obtained comprised patients’ demographics, treatment results, duration of isolation, and confirmation date of the infection. The data of COVID-19 patients currently receiving in-hospital treatment were excluded from the database as treatment results were not available yet. Second, the control population was extracted from the database of NHIS by matching. Therefore, the stratification method was used to match the control population based on the age, sex, and place of residence of COVID-19 patients, and the ratio of matching was 1:15 (COVID-19 patients: Control population). Third, the KDCPA provided data of individuals who had undergone the COVID-19 PCR test, and the results were negative. In South Korea, the KDCPA conducted COVID-19 PCR tests for individuals who had direct or indirect contact with COVID-19 patients in the community or hospital after extensive contact tracing of COVID-19 patients [14]. Therefore, the NHIS-COVID-19 DB comprised three groups: 1) COVID-19 positive group, 2) control population, and 3) negative-tested individuals. All prescription information of procedures and/or drugs and disease diagnoses according to the International Classification of Diseases, Tenth Revision (ICD-10) codes from 2015 to 2020 were also included in the database. Therefore, all underlying diseases of study participants in the NHIS-COVID-19 DB could be evaluated from January 1, 2015, to December 31, 2019 (5 years).
Study participants: COVID-19 survivors and control group
In the NHIS-COVID-19 DB, the individuals diagnosed with COVID-19 and discharged alive from the hospital after treatment were defined as COVID-19 survivors. Additionally, COVID-19 patients who were not admitted to the hospital due to mild symptoms or no symptoms were also defined as COVID-19 survivors if they recovered as confirmed by a PCR test. In South Korea, all COVID-19 patients are isolated by the government until their COVID-19 treatment is terminated in the hospital or they recover from COVID-19, as confirmed by a negative PCR test. Therefore, the COVID-19 survivors include two groups: 1) those admitted in the hospital after the diagnosis of COVID-19 and discharged alive, and 2) those who were not admitted to the hospital due to mild symptoms or had no symptoms after diagnosis of COVID-19, and isolation was terminated after a confirmed negative PCR test. In South Korea, COVID-19 patients with severe symptoms, such as pneumonia, were admitted to the hospital. However, those who had mild or no symptoms were isolated and closely monitored in government-managed centers. The control group in this study comprised the control population (matched according to the baseline data of COVID-19 patients) and PCR test-negative individuals. Individuals >20 years old and those who had a previous history of insomnia disorder till December 31, 2019, were excluded from the final analysis.
Endpoint: development of insomnia disorder
Insomnia disorder was identified using the ICD-10 codes G47.0 (disorders of initiating and maintaining sleep, insomnia) and F51.0 (non-organic insomnia). It was evaluated from January 1 till December 1, 2020. In South Korea, the ICD-10 codes of insomnia disorder require registration by physicians or psychiatrists for patients to receive financial coverage for the treatment.
Measurement as confounder
The following clinico-epidemiological characteristics were identified as confounders in this study. Age and gender were considered as demographic variables, and residence (Seoul, Gyeonggido, Daegu, Gyeongsangbukdo, and other areas) and annual income level in 2020, using quartile ratio, were considered as socio-economic status-related information. Regarding information about underlying diseases, the underlying disability (mild to moderate or severe) and Charlson comorbidity index (CCI) scores were used. The CCI was calculated using the individual comorbidities with the registered ICD-10 codes from 2015 to 2019, as is seen in Supplementary Table 1 (in the online-only Data Supplement). In South Korea, all disabilities have to be registered in the NHIS database to receive benefits from the social welfare system. Disabilities were divided into 15 types as follows: physical and brain lesion disabilities; visual disturbances; hearing and speech disabilities; autism; intellectual, mental, renal, heart, and respiratory disorders; hepatopathy; intestinal and urinary fistulae; and epilepsy. Each disability was assigned a grade within a range of six, based on the severity, and two severity groups were considered (1–3: severe disability and 4–6: mild to moderate disability). In addition to comorbidity information, the underlying psychiatric illnesses such as anxiety disorder, depression, bipolar disorder, substance abuse, and post-traumatic stress disorder (PTSD) were considered confounders, as insomnia disorder is commonly associated with psychiatric disorders [15]. Finally, treatment information of COVID-19 patients was collected, including supplemental oxygen therapy, mechanical ventilator use, continuous renal replacement therapy (CRRT), extracorporeal membrane oxygenation (ECMO) use, and high-flow oxygen therapy. If COVID-19 survivors received any specific treatment according to the treatment information, they were considered as a part of the specific treatment group.
Statistical analysis
The clinico-epidemiologic characteristics of all participants in this study were presented as mean values with standard deviations for continuous variables (CCI) and numbers with percentages for categorical variables (all other variables except for CCI). To compare the characteristics of the COVID-19 survivors and the control group, t-tests and chi-square tests were used to determine the continuous and categorical variables, respectively. Univariate and multivariate logistic regression analyses were conducted to determine if COVID-19 survivors were associated with a higher prevalence of insomnia disorder than the control group. For multivariable logistic regression modeling, all covariates were included in the analysis for adjustment. Next, we constructed multivariable Models 2, 3, and 4 for sensitivity analyses. In multivariable Model 2, the COVID-19 survivors were divided into two groups; that is, the no specific treatment group and specific treatment group, and investigated the effect of treatment experience on the development of insomnia disorder among survivors. The treatment information was included in the multivariable Model 3 to examine the effect of the experience of each specific type of treatment on the development of insomnia disorder among survivors. The duration of isolation due to COVID-19 was included in multivariable Model 4 as a continuous variable. A multivariable logistic regression model was constructed for the development of insomnia disorder after excluding all individuals who died in 2020, as the deaths in 2020 (evaluation period) may have impacted the development of insomnia disorder in both the COVID-19 survivor and the control group in this study. Finally, subgroup analyses were performed according to underlying psychiatric illness, gender, age, and CCI. All multivariable models confirmed that there was no multicollinearity between the variables (variance inflation factor of <2.0), and Hosmer–Lemeshow tests confirmed that the goodness of fit in the models was appropriate at p>0.05. The results of the logistic regression models are presented as odds ratios (ORs) with 95% confidence intervals (CIs). The R software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria) has been used for all analyses, and a p-value <0.05 was considered statistically significant.
RESULTS
Study population
The NHIS-COVID-19 DB initially contained information regarding 351,377 individuals (COVID-19 patients, 8,070; control population, 121,050 individuals; and negative-tested, 222,257 individuals). However, 23,003 individuals <20 years old, 11,566 individuals who had mental illness before 2020, and 179 COVID-19 patients who died due to the infection during hospitalization were excluded from the final analysis. Therefore, a total of 299,968 individuals were included in the final analysis. Among them, 6,934 were considered COVID-19 survivors, while the control group comprised 292,764 participants (Figure 1). The clinico-epidemiological characteristics of the total population in this study are presented in Supplementary Table 2 (in the online-only Data Supplement). Among the total study population, 7,992 (2.7%) individuals were newly diagnosed with insomnia disorder in 2020. The results of comparing clinico-epidemiological characteristics between COVID-19 survivors and the control group are presented in Table 1. The prevalence of insomnia disorder was significantly higher in the COVID-19 survivor group (5.4%, 377 of 6,934) than the control group (2.6%, 7,615 of 292,764) (p<0.001).
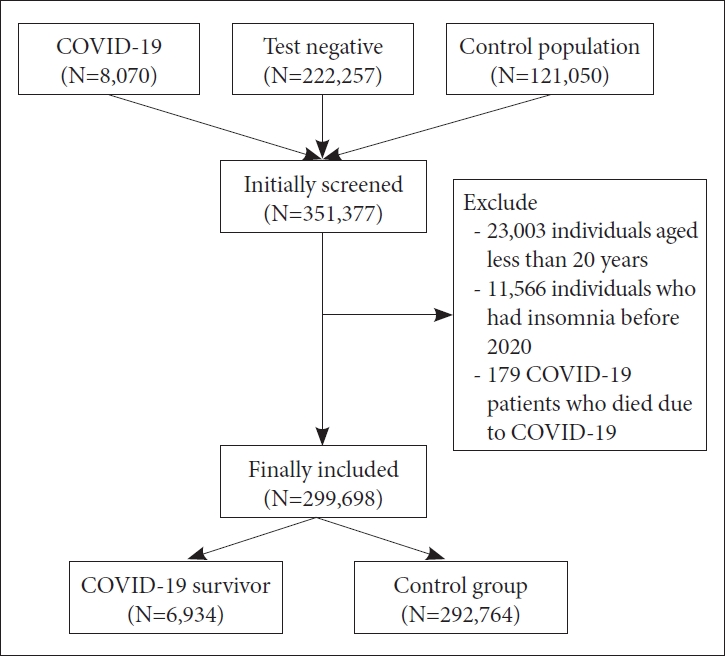
Flow chart depicting the participant selection process. COVID-19, coronavirus disease of 2019.

Comparison of clinico-epidemiological characteristics between COVID-19 survivor and the contol group
Insomnia disorder in COVID-19 survivors
Table 2 shows the results of the logistic regression analysis for the development of insomnia disorder in 2020. In the unadjusted univariable analysis, COVID-19 survivors indicated a 2.15-fold higher prevalence of insomnia disorder than the control group (odds ratio [OR]: 2.15, 95% confidence interval [CI]: 1.94–2.38; p<0.001). In multivariable Model 1, after covariate adjustment, COVID-19 survivors indicated a 3.33-fold higher prevalence of insomnia disorder than the control group (OR: 3.33, 95% CI: 2.98–3.73; p<0.001). In multivariable Model 2, the COVID-19 survivors with no specific treatment and COVID-19 survivors with specific treatment were associated with a 3.16-fold (OR: 3.16, 95% CI: 2.77–3.59; p<0.001) and 3.89-fold (OR: 3.89, 95% CI: 3.17–4.78; p<0.001) higher prevalence of insomnia disorder than the control group. In multivariable Model 3, the prevalence of insomnia disorder in the oxygen therapy group and mechanical ventilator use group was associated with a 2.42-fold (OR: 2.42, 95% CI: 2.28–2.56; p<0.001) and 1.34-fold (OR: 2.42, 95% CI: 2.28–2.56; p<0.001) higher prevalence of insomnia disorder, respectively, as compared to the control group. In multivariable Model 4, the increase in the duration of isolation due to COVID-19 by 1 day, was associated with a 2% higher prevalence of insomnia disorder (OR: 1.02, 95% CI: 1.01–1.03; p<0.001). Other variables in the multivariable logistic regression Model 1 are presented in Supplementary Table 3 (in the online-only Data Supplement). In Table 3, similar trends were observed in the sensitivity analyses, such as logistic regression analyses for the development of insomnia disorder in 2020, and this excluded the 9,097 individuals who died in 2020 (n=291,706).

Logistic regression analysis for development of insomnia disorder in 2020

Logistic regression analysis for development of insomnia disorder in 2020, excluding 9,097 individuals who died in 2020 (N=291,706)
Subgroup analyses
Table 4 shows the results of subgroup analyses according to the presence of underlying psychiatric illness, gender, age, and CCI. In individuals with psychiatric illness (n=88,742), the COVID-19 survivors indicated a 2.85-fold (OR: 2.85, 95% CI: 2.41–3.37; p<0.001) higher prevalence of insomnia disorder than the control group. Individuals without psychiatric illness (n=210,956) had a 3.80-fold (OR: 3.80, 95% CI: 3.28–4.41; p<0.001) higher prevalence of insomnia disorder than the control group. The COVID-19 survivors had a 3.00-fold (OR: 3.00, 95% CI: 2.48–3.63; p<0.001) and 3.54-fold (OR: 3.54, 95% CI: 3.08–4.06; p<0.001) higher prevalence of insomnia disorder in the male and female groups, respectively. In the subgroup analyses according to age, the COVID-19 survivors showed a 2.74-fold (OR: 2.74, 95% CI: 2.02–3.72; p<0.001), 4.16-fold (OR: 4.16, 95% CI: 3.50–4.95; p<0.001), and 2.97-fold (OR: 2.97, 95% CI: 2.52–3.51; p<0.001) higher prevalence of insomnia disorder in the 20–39, 40–59, and ≥60 years groups, respectively. In the subgroup analyses according to CCI, the COVID-19 survivors showed a 4.25-fold (OR: 4.25, 95% CI: 3.59–5.04; p<0.001) and 2.88-fold (OR: 2.88, 95% CI: 2.48–3.34; p<0.001) higher prevalence of insomnia disorder in the 0–2 and ≥3 in the CCI group, respectively.

Subgroup analysis
DISCUSSION
In this population-based cohort study, 5.4% of the COVID-19 survivors were diagnosed with insomnia disorder during the six-month follow-up period. After adjustment for covariates, the COVID-19 survivors showed a 3.33-fold higher prevalence of insomnia disorder than the control group. Furthermore, both the COVID-19 survivor groups, including those who required specific treatment for COVID-19, were associated with a higher prevalence of insomnia disorder, suggesting that even survivors with mild or no symptoms experienced insomnia disorder with a higher prevalence than the control group. Interestingly, in subgroup analyses, higher ORs of COVID-19 survivors for development of insomnia disorder were observed in individuals without psychiatric illness or the lower CCI group than in the individuals with psychiatric illness or higher CCI group.
In this study, insomnia disorder was identified using the ICD-10 codes G47.0 and F51.0, and the prevalence of insomnia disorder was 2.7%. In a recent study in South Korea, the prevalence of insomnia disorder in 2013 was 5.78% among those >20 years old [8], which was higher than that in this study. As outpatient clinic visits decreased due to the COVID-19 pandemic crisis in 2020 [16,17], the diagnosis of insomnia disorder might be lower in 2020 than the previous period. Furthermore, this study might have been influenced by detection bias [18] because we used registered ICD-10 codes for insomnia disorder. For example, individuals who were living in areas with better hospitals or outpatient clinics might be more likely diagnosed by a physician as insomnia disorder than those in areas with poorer access to medical facilities. Therefore, this result should be interpreted regarding detection bias and the COVID-19 pandemic crisis in 2020.
Insomnia disorder is associated with diseases of the central nervous system (CNS) [19,20], and a reduction in gamma-aminobutyric acid levels in the brain has been reported in patients with insomnia disorder [21]. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), a true pathogen of COVID-19, is known to affect the CNS system [22]. In a previous study, Zhou et al. [23] reported that some COVID-19 patients were diagnosed with viral encephalitis, and SARS-CoV-2 was detected in the cerebrospinal fluid of their patients, suggesting the neuroinvasive potential of SARS-CoV-2. As neuroinflammation, in addition to systemic inflammation, has been reported to be related to the development of insomnia disorder [24,25], the damage to the CNS due to COVID-19 may have led to the higher prevalence of insomnia disorder in the survivors in this study.
Insomnia disorder is also known to be strongly associated with psychosocial factors [26], and the impact of mental illness and stress on the development of insomnia disorder has been reported in previous studies [27]. Previous studies have reported that COVID-19 survivors suffer from newly diagnosed psychological disorders such as depression, psychosis, PTSD, and anxiety disorders, which might affect their quality of life [28-31]. Furthermore, the higher prevalence of mental illness in the survivors could also be caused by social stigma, as reported in previous studies [32,33]. A recent study conducted in Germany reported that COVID-19 patients were at a higher risk of unemployment due to the social stigma of COVID-19 [34]. Such unemployment is attributed to the development of depression, according to a previous epidemiological study [35]. Geng et al. [36] reported a significant bidirectional relationship between insomnia disorder, PTSD, and depression among 1,492 survivors who had experienced the 2008 Wenchuan earthquake in China. Similarly, during the Middle East Respiratory Syndrome (MERS) outbreak in South Korea, 28.6% of MERS survivors were diagnosed with insomnia disorder during the 12-month follow-up period [37]. Based on these perspectives, increased assessment of insomnia disorder among COVID-19 survivors could also be attributed to psychosocial factors.
A higher association of insomnia disorder among COVID-19 survivors who had to undergo specific treatment for the infection, such as supplemental oxygen therapy and mechanical ventilation, was observed in this study, as compared to the survivors with mild or no symptoms. A recent single-center descriptive cohort study reported that survivors of critical illness arising due to COVID-19 were at a higher risk of developing post-intensive care syndrome (PICS), including psychiatric illnesses such as PTSD and depression [38]. In this study, COVID-19 patients who required supplemental oxygen therapy or mechanical ventilator support were admitted to the intensive care units in the hospital. Considering that insomnia disorder is known as an important type of PICS among survivors following critical illness [39], the results suggest that COVID-19 survivors who experienced specific therapy may have a higher probability of developing PICS than other survivors who did not have severe symptoms.
This study has several limitations. First, some variables such as body mass index, history of alcohol consumption, and smoking were not included in this study for adjustment, as the NHIS database did not contain this information. Second, the study used multivariable adjustment using confounders; however, unmeasured and unknown confounders may have affected the results. Third, although information regarding all patients suffering from insomnia disorder should be registered in the NHIS database to receive proper financial coverage from the government, it is a possibility that some cases may be missing due to lack of accessibility to health resources among the national population in South Korea. Fourth, although some treatment information of the COVID-19 survivors has been utilized, the severity of the infection is not reflected in the study’s laboratory results. Moreover, we did not include the regular prescription data of hypnotic drugs in defining insomnia disorder because the prescription information of the drug was not available from September 1, 2020, to December 1, 2020. A recent cohort study reported that 4.8% (2,206/46,167) of patients with insomnia disorder received hypnotics prescriptions only without an ICD-10 diagnosis [8]. Therefore, there might be some misplaced cases of insomnia disorder using only ICD-10 codes in this study. Although some limitations exist, this study analyzed data from a large population (299,968 individuals) to identify the association of COVID-19 survivors with the development of insomnia disorder during the 6 months follow-up period.
Summarily, it can be stated that 5.4% of COVID-19 survivors in South Korea were newly diagnosed with insomnia disorder during the 6 months follow-up period. The COVID-19 survivors showed a 3.33-fold higher prevalence of insomnia disorder than the control group, and the survivors who needed specific treatment for the infection as well as those who did not were associated with a higher prevalence of insomnia disorder, suggesting that the survivors with mild or no symptoms also experienced insomnia disorder. The results suggest that insomnia disorder is an important public health issue that needs to be addressed to enhance the quality of life of COVID-19 survivors.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.30773/pi.2021.0223.
The ICD-10 codes used by comorbidity to compute the Charlson comorbidity index
Clinico-epidemiological characteristics of total participants (N=299,698)
Other variables in multivariable logistic regression model 1
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: all authors. Data curation: In-Ae Song, Hye Yoon Park. Formal analysis: Tak Kyu Oh. Funding acquisition: Hye Yoon Park. Investigation: In-Ae Song. Methodology: all authors. Project administration: Tak Kyu Oh. Resources: Tak Kyu Oh. Supervision: In-Ae Song. Validation: Tak Kyu Oh. Writing—original draft: Hye Yoon Park, In-Ae Song. Writing—review & editing: Tak Kyu Oh.
Funding Statement
This research was supported by a grant of Patient-Centered Clinical Research Coordinating Center (PACEN) and COVID-19 Public Health Research funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI19C0481, HC20C0013).