Traumatic Effects of the COVID-19 Outbreak in Middle School Students and Caregivers
Article information

Abstract
Objective
To investigate the traumatic effects of the COVID-19 pandemic on middle-school students and their parents.
Methods
This epidemiological cross-sectional study was conducted with middle-school students in Denizli. A questionnaire consisting of the IES-R, CRIES-13 and a sociodemographic data form was delivered online. A total of 1059 participants who fully completed the questionnaire were included for analysis.
Results
The IES-R total and subdimension scores and the CRIES-13 scores were found to be significantly higher in families with an income level of ≤2,500 TL. The CRIES-13 scores of children were found to be significantly higher in divorced families. No statistically significant difference was determined between the IES-R total and subdimension scores of the parents who were healthcare workers and the CRIES-13 scale scores of their children.
Conclusion
A statistically significant, positive, moderate relationship was found between the IES-R scale total and subdimension scores of parents and the CRIES-13 scale scores of children. A low socioeconomic level was seen to increase the prevalence of anxiety in adults and adolescents. The children of divorced families were found to be at higher risk of PTSD. Successful management of mental health symptoms in parents will reflect positively on the mental health status of their children.
INTRODUCTION
of millions of people have been severely restricted because of the COVID-19 pandemic caused by the SARS-CoV-2 virus [1]. To be able to control the spread of the pandemic in Turkey, schools, universities, parks, theaters and cinemas, restaurants, etc., have been closed since the end of March 2020 and restrictions have also been imposed in other areas. The COVID-19 pandemic has had numerous negative effects on the lives of children, such as acute-chronic stress, anxiety about the family, unexpected and sudden losses, inability to attend school, increased internet and social media use, and anxiety about the economic future of their families and their country [2]. Social interactions have been disrupted because of school closures and curfews. While supporting remote education for children, parents have been working from home, with no access to other systems for support in the care and education of children (broader family, courses, etc.). In addition to these concerns, many people in all countries have lost their jobs as a result of the COVID-19 pandemic, which has created further economic problems. This issue has had a significant effect on children, adolescents and the whole family, and negative effects have been seen on mental health [3].
It is known that children show various stress reactions when they face unexpected and unknown events, and so it would wrong to think they are not affected by the trauma and consequences of the COVID-19 pandemic. Although there are studies concerning the reactions of children to traumatic events, very few studies have examined how epidemics affect children [4].
Since COVID-19 is a recent pandemic, studies related to its effect on mental health are limited and our knowledge of the effects of pandemics on mental health are based on studies conducted during epidemics caused by other infections. Studies which were conducted during the Severe Acute Respiratory Syndrome (SARS) epidemic showed an increase in stress and the frequency of diagnosis of post-traumatic stress disorder (PTSD) in individuals [5].
In studies which have examined the effect of the COVID-19 pandemic on the mental health of children, social isolation and restrictions have been seen to affect adolescents, and symptoms of anxiety have increased [6-8].
A study in the Republic of Ireland reported an increase in feelings of social isolation, depression, anxiety, and inappropriate behaviour in children because of the COVID-19 pandemic [9]. Another study in China found the most commonly seen mental health symptoms in children and adolescents during the COVID-19 pandemic to be attention problems, behavioural disorders, irritability, and fears related to infection transmission [10]. A study in Turkey showed that the mental health of children was negatively affected by separation from their parents during the COVID-19 pandemic [11].
In the light of this information, it is predicted that pandemic may have traumatic effects on children and their parents and this effect may increase the mutual traumatic impact between the child and the parent, besides traumatic effects on the parent and the child may be higher if the parent is a healthcare worker. It was thought that a high socioeconomic level of the family would reduce the traumatic impact, while a low socioeconomic level could increase the traumatic effect.
The objective of this study was to assess the traumatic effects of the COVID-19 pandemic on the mental health of children and their parents and the relationships between them. From the data obtained it was aimed to examine whether or not the COVID-19 pandemic had a traumatic effect on the parents and children. If there is a traumatic effect, it was aimed to investigate the relationship between this traumatic effect and the sociodemographic characteristics of the parents.
METHODS
Type of study and participants
This was a cross-sectional epidemiological study, with a study population of secondary school-aged children, in Pamukkale and Merkezefendi counties. The necessary permission was obtained from the Ministry of Health, Scientific Research Studies Commission, Pamukkale University Faculty of Medicine, Non-Interventional Clinical Studies Ethics Committee (09.06.2020/11) and the Provincial Directorate of National Education. The sampling calculation for the schools and students in schools was made using the sampling formula with the known universe. The universe contained 111 schools and 40,835 students and the rate of incidence was deemed to be 50%. When the calculation was made considering the deviation margin for determination of the number of schools as d=0.3 and number of students as d=0.05, it was calculated that 381 students from 11 schools had to be included in the study. A total of 11 secondary schools were selected at random from 38 public secondary schools in Pamukkale county, 44 public secondary schools in Merkezefendi county, and 29 private secondary schools. A random selection was made to include 4 schools from Pamukkale county, 5 from Merkezefendi county and 2 private schools. The total number of students in these randomly determined schools was 5,170, and it was aimed to reach the families of students, to conduct the study with all the students and their families, who met the eligibility criteria and who were willing to participate in the study and provide feedback. An online questionnaire consisting of 54 questions was delivered, consisting of the Impact of Events Scale-Revised form (IES-R) validated in Turkish, to be completed by parents, the Child Revised Impact of Events Scale-13 (CRIES-13), and a sociodemographic data form prepared by the researchers. All parents and students, who agreed to participate in study, were included with no exclusion criteria. A total of 1,107 students, aged 10 to 15 years agreed to participate in the study together with their parents, and the questionnaire was fully completed by 1,059 participants.
Data collection tools
An online questionnaire consisting of 54 questions, consisting of Impact of Events Scale -Revised form (IES-R) validated in Turkish, the Child Revised Impact of Events Scale-13 (CRIES-13), and a sociodemographic data form prepared by the researchers was sent to the study participants.
Impact of Events Scale-Revised form (IES-R)
Impact of Events Scale-Revised form (IES-R) is a self-report scale, consisting of 22 items, which was developed to measure subjective anxiety and difficulty caused by traumatic events. The scale assesses the aspects of traumatic stress syndrome, as avoidance, hyperstimulation and re-experience. The level of experience of symptoms in the last week is assessed using a Likert response of 0–4 (none-very much) with total scores ranging between 0 and 88. Higher points indicate a higher level of traumatic stress [12]. Turkish adaptation of the scale was made by Corapcioglu et al. [13] In a study of 104 subjects diagnosed with PTDS and 65 subjects without PTSD, the internal consistency of the test was calculated as 0.94, and when the cutoff value of the scale was between 24–33, sensitivity was found to be 74.0–92.2% and specificity, 70.7–81.0%. The total IES-R score is evaluated as an indicator of normal (0–23), mild (24–32), moderate (33–36) or severe (≥37) psychological effect.
Child Revised Impact of Events Scale-13 (CRIES-13)
This scale, which was adapted from the Impacts of Events Scale (IES), consists of 13 items [14,15]. It may be applied to children aged 8–18 years, who have experienced a traumatic event. The level of experience of the issues specified in the scale during the last week is assessed using Likert responses between 0 and 5 (0: almost none, 1: rarely, 3: sometimes, 5: frequently). Scores, which may be obtained from the scale The total score ranges between 0 and 65, with a score of ≥30 indicating a risk for Post-Traumatic Stress Disorder (PTSD) [14]. Turkish adaptation of the scale was made by Çeri et al. [16].
Sociodemographic data form for children and their families
Sociodemographic data form for children and their families this form was created by the researchers to examine the sociodemographic characteristics of the participating children and parents.
Ethical aspect of study
The necessary permission for the study was obtained from the Ministry of Health, Scientific Research Studies Commission, Pamukkale University Faculty of Medicine, Non-Interventional Clinical Studies Ethics Committee (dated June 9, 2020 and numbered 11) and the Provincial Directorate of National Education. The link to the study questionnaires was delivered to the population sample online. Brief information was provided about the study and participants were asked whether they wanted to participate in the study.
Data analysis
Data was analyzed using SPSS 25.0 package program (IBM Corp., Armonk, NY, USA). Continuous variables are given as mean±standard deviation, median (minimum-maximum values) and categoric variables as number and percentage. Kolmogorov Smirnov test and Histograms were used for determination of normal distribution. For independent groups comparisons, we used Mann-Whitney U test. Spearman correlation analysis was used for analyzing the relationships between continuous variables. The difference between categorical variables was analyzed with chi-square analysis. Statistical significance was determined as p<0.05.
RESULTS
A total of 1,107 students participated in the study together with their parents, of which 1,059 completed the questionnaire fully and so were included in the analysis. Of the 1,059 respondents, the questionnaire was completed by the mother in 80.1% (n=848) of cases, by the father in 17.9% (n=190), and by a caregiver other than the mother or father in 2% (n=21). The sociodemographic data of the respondents are shown in Tables 1, 2 and 3.

Demographic data of children

Demographic data of family

Average ages of parents and children
The mean score of the IES-R, completed by parents, was 30.03±16.72 (min-max: 0–80). The scores of 37.3% of the parents (n=395) were in the normal range, 21.6% (n=229) were mild, 7.5% (n=79) were moderate, and 33.6% (n=356) were severe. The IES-R total and subdimension scores of the parents were not found to vary according to the gender of children. In the IES-R completed by fathers, the scores were found to be significantly lower than those completed by mothers and non-parent caregivers (p=0.0001). The obtained data are shown in Table 4. The IES-R total and subdimension scores were found to be statistically significantly lower in families with an income of ≥10,000 TL (p=0.001). The IES-R total and subdimension scores were found to be statistically significantly higher in families with an income of ≤2,500 TL (p=0.001). The obtained data are shown in Table 5.

IES-R scores by mother, father or caregiver

Relationship between IES-R scores and family income
The mean score of the CRIES-13 was 18.44±13.26 (min-max: 0–65) with 20.9% (n=221) of the children scoring ≥30 points. The CRIES-13 points showed no difference according to the gender of the children. The CRIES-13 scores were found to be significantly higher for the children of divorced families (p=0.047), and in families with an income of ≤2,500 TL (p= 0.028). The obtained data are shown in Table 6.
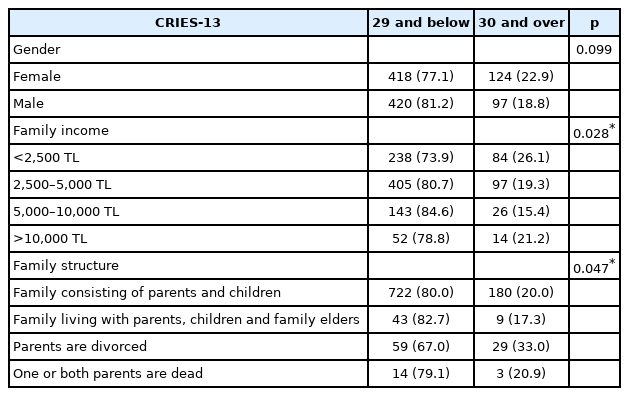
Relationship between CRIES-13 scores and gender, family income, family structure
When the scores for the 3 subdimensions of the IES-R were examined, the mean score for repeated experience was 9.62± 7.09 (min-max: 0–32), the mean score for avoidance was 14.36±7.08 (min-max: 0–32), and the mean score for hyperstimulation was 6.06±5.54 (min-max: 0–24).
A statistically significant positive moderate correlation was determined between the repeated experience, avoidance, and hyperstimulation subdimension scores of the IES-R and the CRIES-13 scale scores (p=0.0001, r=0.525; 0.522; 0.506). A statistically significant, positive, moderate correlation was determined between the total IES-R scale points of the parents and the total CRIES-13 scale points of the children (p=0.0001, r=0.616). The child’s trauma was seen to increase with an increase in parental trauma and the parent’s susceptibility to trauma was seen to increase with an increase in trauma of the child. The obtained data are shown in Table 7.
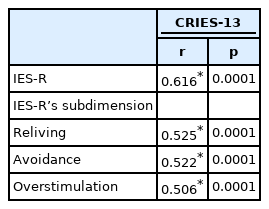
Correlation value between IES-R sub-dimension score and CRIES-13 score
The data showed that 7.5% of the parents (n=79) were healthcare workers, of which 1.4% (n=15) were actively working in COVID-19 wards and clinics. No statistically significant difference was determined between the IES-R total and subdimension scores of healthcare worker parents and non-healthcare worker parents and the CRIES-13 scale scores of their respective children, although the total and subdimension scores of the healthcare workers were observed to be higher. The obtained data are shown in Table 8. Among the healthcare workers, there was no statistically significant difference between the scale scores of parents actively working in COVID-19 wards and those who were not, and their respective children.

IES-R and CRIES-13 scores according to whether the parents are Healthcare Worker or not
DISCUSSION
This study aimed to examine the traumatic effects of the COVID-19 pandemic on the mental health of parents and children. Evaluation was made of a total of 1,059 students and their parents from an initial 1,107 students from 11 schools in 2 counties in Denizli provincial center.
According to the IES-R scores, 21.6% of parents were mildly, 7.5% moderately, and 33.6% were severely affected. In a similar study conducted in Italy, 33.2% of parents were found to be severely affected [1]. In CRIES-13, a score of 30 and over defines a risk for PTSD [14].
According to the CRIES-13 scores, 20.9% of the children had scores of ≥30. The CRIES-13 points showed no difference according to the gender of the children. In the study in Italy 30.4% of the children had scores of ≥30 [1].
A statistically significant positive moderate correlation was found between the parent IES-R scale total scores and the repeated experience, avoidance and hyperstimulation IES-R subdimension scores and the CRIES-13 scale scores of the children. This result supported our hypothesis. The child’s trauma was seen to increase with an increase in the parent’s trauma and the parent’s susceptibility to trauma increased with the child’s trauma. In the study conducted in Italy, a similar positive correlation was seen between the two scale scores [1]. Correlation between child and parent scale scores is a predictable and expected result, which may be explained by the similarity in mood and emotional interaction capacity in parents and children, genetic susceptibility and environmental factors. This result shows the strong bond between the mental health of parents and children.
In the current study, the parents of 7.5% of the participants were healthcare workers, of which 1.4% actively worked in COVID-19 wards and clinics. The mean IES-R score of nonhealthcare worker parents was 29.92 and the mean IES-R score of healthcare worker parents was 31.49. These results are consistent with other studies, conducted in Italy and Wuhan- China [1,17,18]. No statistically significant difference was determined between the IES-R total and subdimension scores of healthcare worker parents and non-healthcare worker parents and the CRIES-13 scale scores of their respective children. This result did not support our hypothesis. No statistically significant difference was determined between the IES-R total and subdimension scores of healthcare worker parents who worked actively in COVID-19 wards and clinics and those of parents who were not working actively in COVID-19 wards and clinics and the CRIES-13 scale scores of their respective children. In another study, it was determined that healthcare workers had higher scores in IES-R compared to non-healthcare workers, and this difference was caused by the healthcare workers working actively with COVID-19 patients [1]. In the current study, although the scores of healthcare workers were not statistically significant, they were higher than the scores of non-healthcare worker parents. However, no difference was seen between parents who were healthcare workers and worked in COVID- 19 wards and clinics and those who did not, and their respective children. This may be explained by the fact that only 7.5% of the participants were healthcare workers and 1.4% were active healthcare workers in COVID-19 wards and clinics, and therefore the sample was small. The high IES-R points of healthcare workers may be attributed to the healthcare workers working under risk during the pandemic. However, while the non-healthcare worker parents were at less risk in respect of exposure to COVID-19, in addition to the quarantine measures, they might have been affected by social stress, such as closure of workplaces, isolation, etc. In a study conducted in Singapore during the SARS epidemic, it was reported that 17.7% of healthcare workers displayed psychiatric symptoms. In that study, the cutoff point of the IES scale was accepted as 26 points [19]. In another study, 17.3% of healthcare workers reported symptoms and in a 1-year follow-up, this rate was reported as 15.4% [20]. Other studies related to the COVID-19 pandemic [1,17,18], have provided higher scores. The global nature of the pandemic, and the effect of cultural differences on emotional symptoms, might have caused this difference.
In the IES-R completed by fathers, the scores were found to be significantly lower, compared to the IES-R completed by mothers and non-parent caregivers. In literature, it has been reported that mood and anxiety disorders, and in some studies, post-traumatic stress disorder, were seen more frequently in women compared to men both among healthcare workers and in the general population [17,21].
The parent IES-R total and subdimension scores were found to be statistically significantly lower in families with an income of ≥10,000 TL. The parent IES-R total and subdimension scores were found to be statistically significantly higher in families with an income of ≤2,500 TL. The CRIES-13 scores in families with an income of ≤2,500 TL were found to be significantly higher. This result supported our hypothesis. A low socioeconomic level is known to increase the incidence of anxiety and depression in adults [22-24]. In a study, it was seen that 96 % of young people in families of a lower socioeconomic level had anxiety and depression and they were mentally more fragile. Factors such as the divorce of parents and parental psychopathology affect the mental health of young people, yet the study results showed the greatest correlation to be with parental income [25]. Although it is known that socioeconomic factors affect depression and anxiety symptoms in young people, the current study is one of the few studies to have demonstrated that such socioeconomic inequalities are related to anxiety in children and adolescents [25-28].
The CRIES-13 scores were found to be significantly higher for the children in divorced families. A divorce is a life event that creates socioeconomic changes and to which children can have difficulty adapting [29]. Children who have been subjected to chronic stress and traumatic experiences in infancy and childhood are known to be mentally more fragile [30]. A previous study reported that the children of families with divorced parents and ongoing conflicts between parents, had more frequent PTSD symptoms [31]. It has been found that in children of divorced families, sensitivity to anxiety was higher [32], and higher anxiety sensitivity increased susceptibility to mental disorders, such as panic disorder, agoraphobia, PTSD, major depressive disorder, social anxiety and substance abuse [33-35]. In the current study, in line with literature, it was determined that children of divorced families were at higher risk of developing PTSD. Although there are studies in literature concerning the reactions of children to traumatic events, there are very few studies which have examined how epidemics affect children [4]. In many studies, it has been reported that due to negative life events and stress, symptoms such as anxiety, depression, lethargy, disturbed social interaction, and loss of appetite, are seen in children [36-40]. Children who have become distant from their social circles and their friends with the closure of schools, experience a significantly restricted social life, and with the decrease in activities, not only become isolated at home and may become increasingly anxious about contracting infection. In this context, the role of parents in the alleviation of the psychological effects of isolation, is very important. Children rely on their parents for protection, and learn by adopting the danger assessment manner of parents as a model [18,41-45]. When a parent has difficulty in coping with anxiety, the level of anxiety increases in the child. The correlation between parent IES-R scores and the CRIES-13 scores of the children, explains this issue. Successful management of mental health symptoms in parents will be positively reflected in the mental health status of children. Pandemics must be accepted as trauma and there is a need for public health initiatives to be increased to be able to improve the mental strength of families. There are growing concerns that children will suffer from mental effects of the COVID-19 pandemic, rather than physical effects.
Limitations
The most important limitation of this study was that not all students could be reached due to the online collection of data. As face-to-face education has not yet been re-started in Turkey, the online collection of data was mandatory and safe due to the continuing COVID-19 pandemic. Nevertheless, the number of respondents was considered to be sufficient.
Strengths
To be able to better reflect the general population, the number of schools and students in those schools to be included in the study was calculated using the sampling of the known universe formula. Therefore, the number of study participants was high.
Acknowledgements
Authors want to thank Hande ŞENOL for the statistical contribution.
Notes
The authors have no potential conflicts of interest to disclose.
Authors’ contribution
Conceptualization: Merve Aktaş Terzioğlu, Ahmet Büber. Data curation: Merve Aktaş Terzioğlu, Ahmet Büber. Formal analysis: Merve Aktaş Terzioğlu, Ahmet Büber. Investigation: Merve Aktaş Terzioğlu, Ahmet Büber. Methodology: Merve Aktaş Terzioğlu, Ahmet Büber. Project administration: Merve Aktaş Terzioğlu, Ahmet Büber. Software: Merve Aktaş Terzioğlu, Ahmet Büber. Supervision: Merve Aktaş Terzioğlu, Ahmet Büber. Validation: Merve Aktaş Terzioğlu, Ahmet Büber. Visualization: Merve Aktaş Terzioğlu, Ahmet Büber. Writing—original draft: Merve Aktaş Terzioğlu, Ahmet Büber. Writing—review & editing: Merve Aktaş Terzioğlu, Ahmet Büber.