The Usefulness of the Korean Version of Penn State Worry Questionnaire for Screening Generalized Anxiety Disorder: A Receiver Operating Characteristic Analysis
Article information
Abstract
Objective
Excessive worry about minor matters and a state in which this worry is experienced as uncontrollable are known to be key symptoms of generalized anxiety disorder (GAD). Given the importance of pathological worry in GAD, the need for psychometrically sound measures of this construct has increased. The purpose of this study was to investigate the usefulness of the Korean version of Penn State Worry Questionnaire (K-PSWQ) for screening GAD.
Methods
Two hundred and forty six patients were initially screened, from which 102 GAD patients and 118 patients with anxiety disorder not otherwise specified (anxiety disorder NOS) were finally enrolled. Patients were diagnosed by a structured clinical interview for the DSM-IV Axis I. We also enrolled 114 control subjects who had no medical or psychiatric history. Pathological worry in both patients and control subjects were assessed at baseline using the PSWQ and we estimated optimal cutoff score by the receiver operating characteristic (ROC) analysis.
Results
We found that in the first ROC analysis, a score of 53 could simultaneously optimize sensitivity and specificity in order to discriminate GAD patients from control subjects. From the second receiver operating characteristic analysis, when both sensitivity and specificity were optimized, we can suggest a score of 61 as being the cutoff for differentiating GAD patients from patients with anxiety disorder NOS.
Conclusion
The Korean version of PSWQ is a useful method for screening GAD patients, although ethnic and cultural differences may affect the cutoff score of PSWQ for GAD.
INTRODUCTION
Estimates of the lifetime prevalence rate of generalized anxiety disorder (GAD) in the general population vary between 3% and 6%.1 The third edition of the Diagnostic and Statistical Manual of Mental Disorder (DSM-III) defined GAD as persistent anxiety, and GAD was most often used as a residual diagnosis for individuals who did not meet diagnostic criteria for another anxiety disorder.2 Although the presence of worry was identified as one of GAD symptoms in the DSM-III, in subsequent editions, the concept of worry gained increasing centrality to the diagnosis of GAD. In the DSM-IV, GAD is characterized by chronic, excessive, and uncontrollable worry about a variety of topics that has occurred most days over a period of at least six months.
Although worry is associated with all anxiety disorders, excessive worrying about minor matters and a sense that this worry is uncontrollable have risen as the factors that distinguish worry in GAD from that in other anxiety disorders.3 Given the importance of the construct of pathological worry in GAD, the need for psychometrically sound measures of this construct is increasing. Among several self-report instruments that measure worry (i.e., the Worry Domains Questionnaire, WDQ; the Student Worry Scale, SWS; the Penn State Worry Questionnaire, PSWQ), the PSWQ is the most widely and frequently used self-report measure for assessing pathological worry in both clinical and non-clinical populations. The PSWQ is a 16-item inventory designed to capture the generality, excessiveness, and uncontrollability of pathological worry. Individuals diagnosed with GAD will have a significantly higher score on the PSWQ than do those who have anxiety disorder not otherwise specified (anxiety disorder NOS) and other anxiety disorders such as social phobia or obsessive-compulsive disorder.4,5
The purpose of this study was to investigate the usefulness of the Korean version of PSWQ (K-PSWQ) for screening GAD. We used ROC analyses between GAD patients and normal control subjects and between GAD patients and patients with anxiety disorder NOS.
METHODS
Subjects
From the total of 246 patients who were diagnosed as having either GAD or anxiety disorder NOS at the Samsung Medical Center from 2008 to 2011, 109 GAD patients and 137 patients with anxiety disorder NOS were screened for the study via a retrospective chart review. All of these patients were diagnosed by a structured clinical interview for the DSM-IV Axis I (SCID-I), administered by trained clinical psychologists. Patients with comorbid psychotic disorders or any form of dementia were excluded from the study. We also excluded individuals with Hamilton Anxiety Rating Scale (HAM-A) scores of less than 14 in both the GAD and anxiety disorder NOS groups since the HAM-A score of less than 14 is generally regarded as the cutoff score for reaching a partial remission state of anxiety disorders.6,7
Of the 246 patients who were initially screened 102 GAD patients and 118 patients with anxiety disorder NOS were finally enrolled in the study. More than half of the GAD patients (75.49%) met the criteria of one or more comorbid axis-I disorders. The most common comorbid diagnoses were depressive disorder (52.33%), dysthymic disorder (23.38%), panic disorder (13.75%), somatoform disorder (2.60%), obsessive-compulsive disorder (2.60%), and social phobia (2.60%). Also more than half of the anxiety disorder NOS patients (56.78%) had one or more comorbid axis-I disorders. The most common comorbid diagnoses were depressive disorder (46.27%), somatoform disorder (13.43%), dysthymic disorder (9.00%), and pain disorder (1.50%).
Considering age and gender of the study subjects, we recruited normal control subjects through advertisement. The control subjects voluntarily agreed to participate in the study and a gift card was given to them for their participation. Finally, we enrolled 114 control subjects who had no medical or psychiatric history. Both patients and control subjects gave their informed consent after being provided with complete information on the study, which was approved by the institutional review board of Samsung Medical Center.
Assessment
The PSWQ is a 16-item self-report scale designed to assess the pathological worry construct present in GAD, in which each item is scored from 1 (not at all like me) to 5 (very like me). The total PSWQ score ranges from 16 to 80, with higher scores reflecting higher levels of worry. We used the Korean version of PSWQ, which Lim et al.8 reported to have a high internal consistency (0.92).
The HAM-A is a clinician-rating scale, which consists of 14 items designed to measure the severity of anxiety symptoms.9 The HAM-A consists of two factors: general psychological anxiety symptoms and cognitive symptoms, and its items are rated with 4-point Likert scales. The total HAM-A score ranges from 0 to 56.
The BAI is a self-report scale, which includes 21 items designed to assess the anxiety symptoms over a 1-week period.10 Each item is rated with a 4-point Likert scale ranging from 0 (not at all) to 3 (almost always), and the total BAI score ranges from 0 to 63. In this study, we used the Korean version of BAI.11
Analysis
The Statistical Package for Social Science (SPSS) version 18.0 was used for all statistical analyses, and statistical significance was defined at the 0.05 level (two-tailed tests). Chi-square tests were conducted to examine group differences in nominal and categorical variables. A Kruskal-Wallis test was used as the data were not normally distributed and Mann-Whitney U test with Bonferroni correction was used for post-hoc analyses. Finally, ROC analyses were conducted to obtain the cutoff point of the PSWQ for screening GAD when considering sensitivity and specificity.
RESULTS
General findings
We found no significant differences in gender, age, education level and socioeconomic and marital status among the clinical samples and control subjects (Table 1). Table 2 shows the anxiety levels of patients with GAD and anxiety disorder NOS, and those of control subjects. GAD patients showed significantly higher scores on the HAM-A (p=0.024) and the PSWQ (p<0.001) than did those with anxiety disorder NOS, whereas there was no difference in the mean BAI score between the two groups. Control subjects showed significantly lower scores on the BAI (p<0.001) and the PSWQ (p<0.001) than the patients with GAD and anxiety disorder NOS.
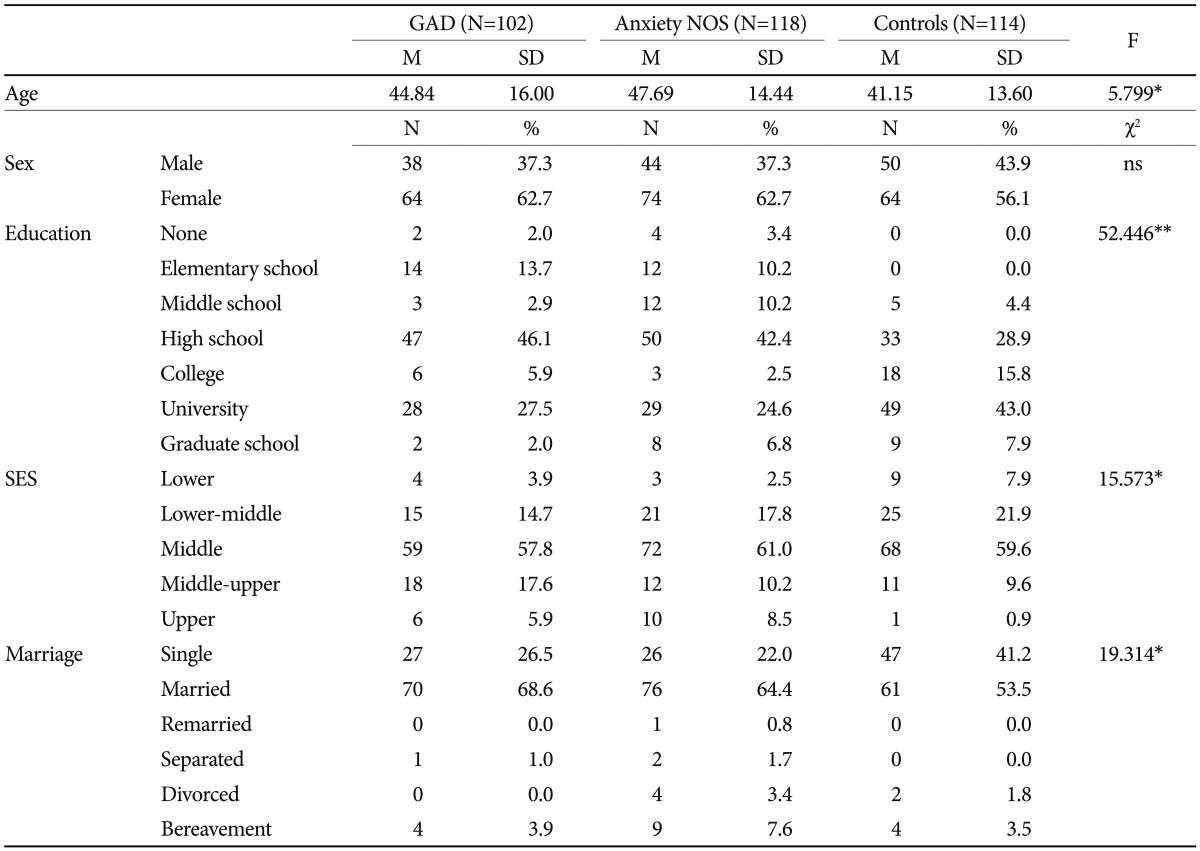
Demographic characteristics of subjects

Mean scores of HAM-A and PSWQ Anxiety in 3 groups
ROC analysis between GAD patients and control subjects
The first set of ROC analyses for the PSWQ score was conducted to differentiate GAD patients from control subjects. As shown in Figure 1, the presence of a good ROC curve supported the usefulness of the PSWQ in differentiating GAD patients from control subjects (AUC=0.904, p<0.001). Table 3 also gives support for the sensitivity and specificity of the PSWQ and thus supported its usefulness as a screening instrument for GAD. When optimizing sensitivity, specificity, and both sensitivity and specificity, the cut off scores of the PSWQ should be 41, 64, and 53, respectively.
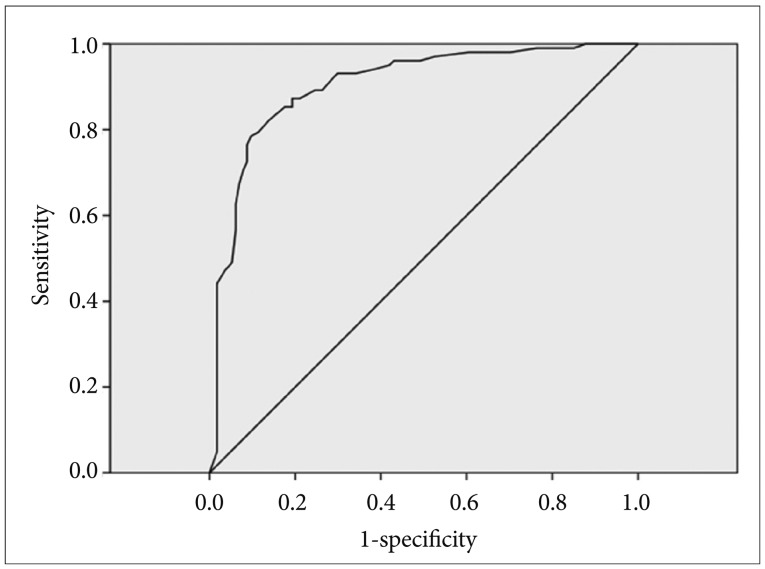
Receiver operating characteristic curve for the utility of the Penn State Worry Questionnaire in differentiating Generalized Anxiety Disorder patients from control subjects.
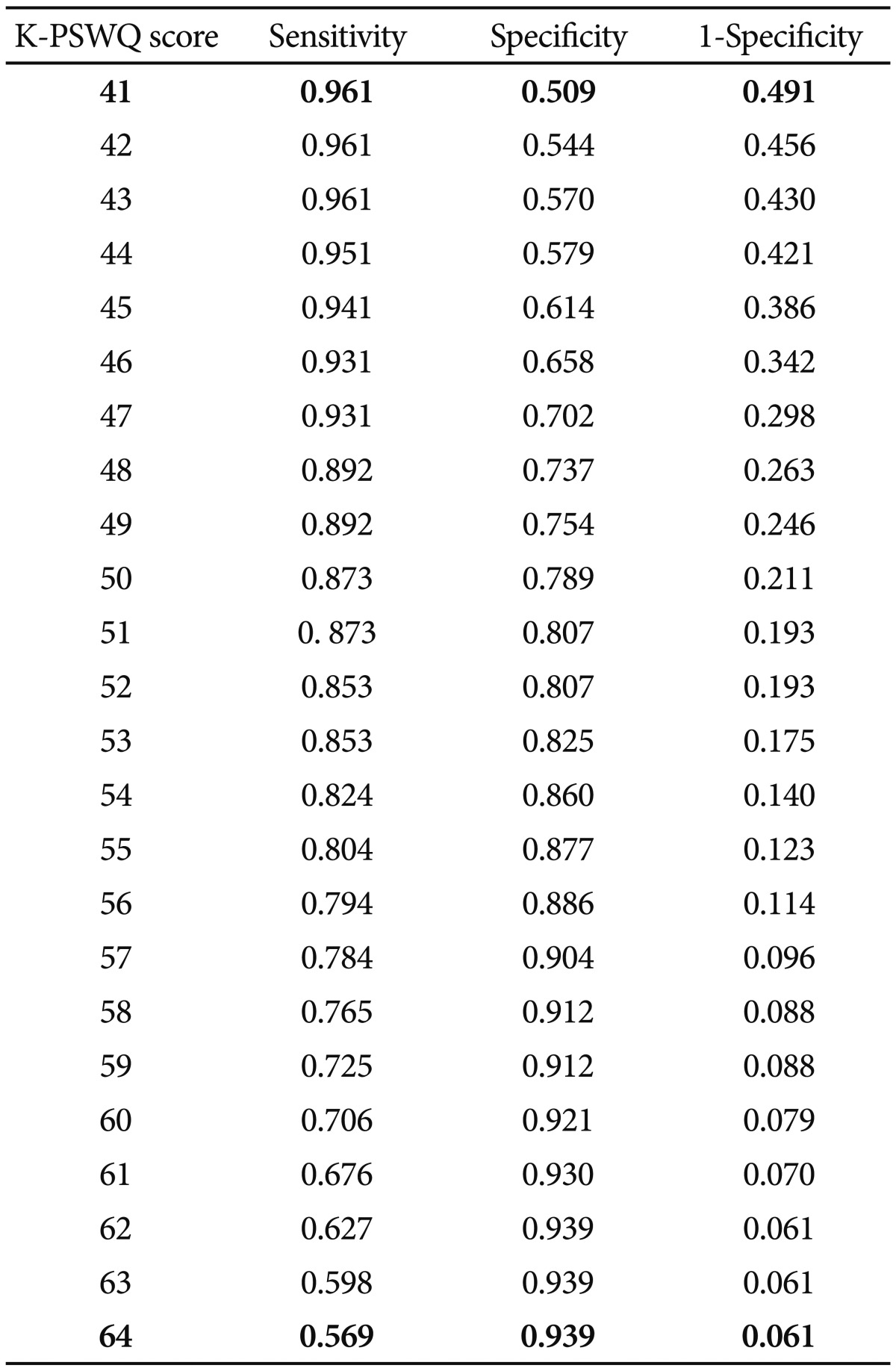
Sensitivity and specificity of the PSWQ in GAD patients and control subjects
ROC analysis between GAD patients and patients with anxiety disorder NOS
The second set of ROC analyses for the PSWQ score was conducted to differentiate GAD patients from patients with anxiety disorder NOS. In Figure 2, the good ROC curve supported the usefulness of the PSWQ in differentiating GAD patients from patients with anxiety disorder NOS (AUC=0.71, p<0.001). Table 4 also provides support for the sensitivity and specificity of the PSWQ and further supports its usefulness as a screening instrument for GAD. When optimizing sensitivity, specificity, and both sensitivity and specificity, the cut off scores of the PSWQ should be 57, 64, and 61, respectively.
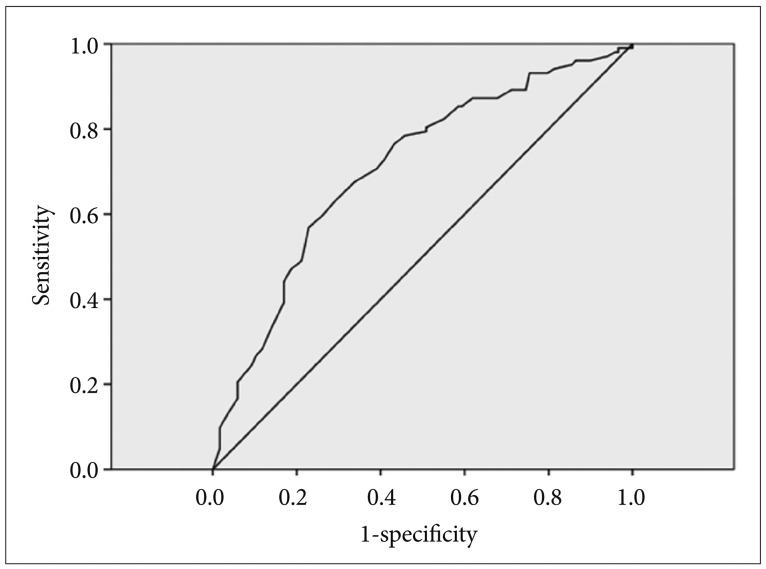
Receiver operating characteristic curve for the usefulness of PSWQ in differentiating GAD patients from patients with anxiety disorder NOS. PSWQ: Penn State Worry Questionnaire, GAD: Generalized Anxiety Disorder, NOS: not otherwise specified.
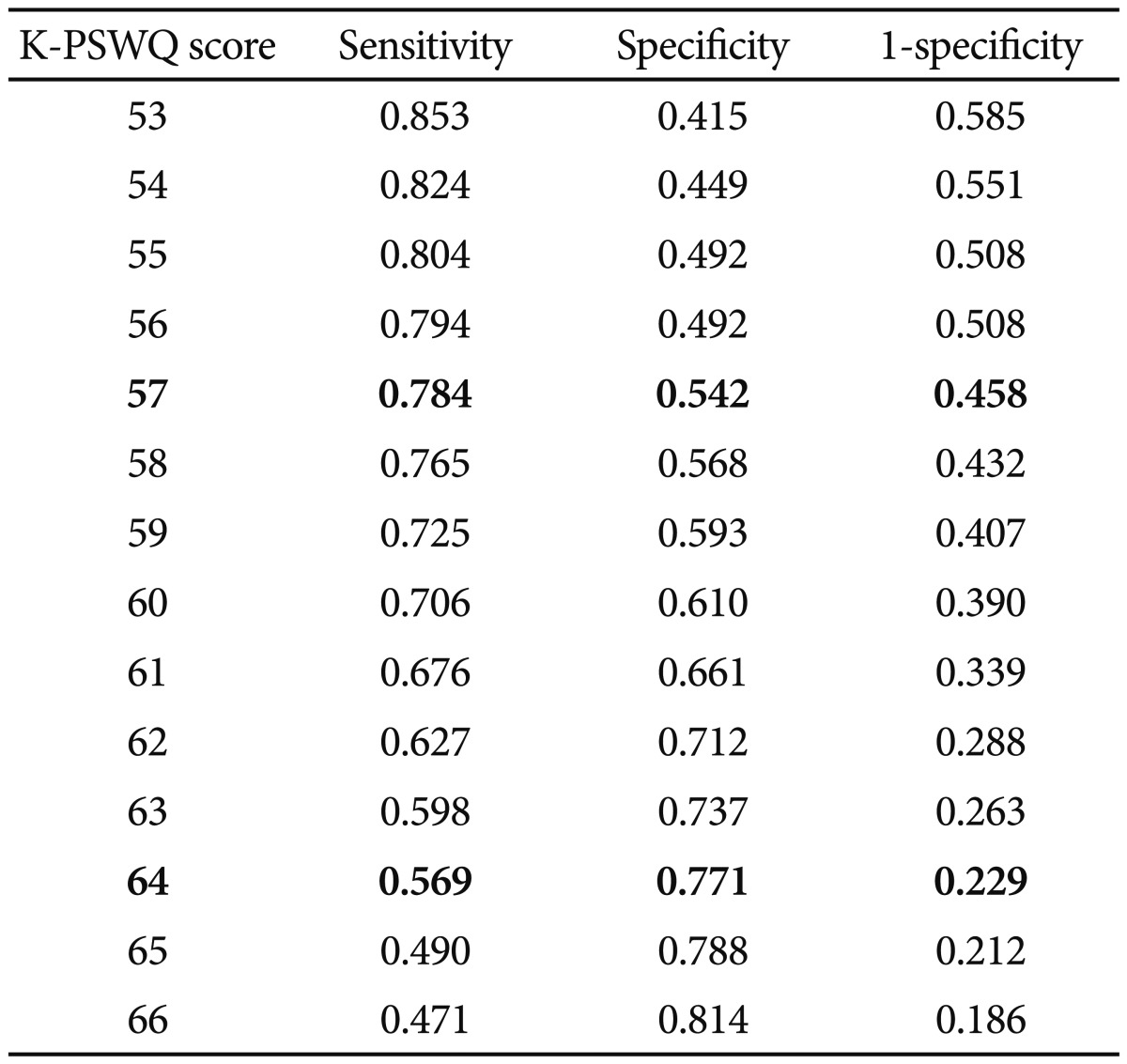
Sensitivity and specificity of the PSWQ in GAD and anxiety disorder NOS patients
DISCUSSION
The Korean subjects in the present study showed different clinical characteristics from those of previous studies that included Caucasian subjects.12,13 Recently, the applicability of the PSWQ as a screening method for GAD has been examined by Behar et al.14 which is the first examination of the PSWQ using a ROC analysis. They obtained PSWQ scores from treatment-seeking GAD patients as well as non-GAD patients and non-anxious control subjects, and suggested a PSWQ cutoff score of 45 for differentiating GAD patients from non-anxious control subjects and 65 for differentiating GAD patients from patients with other anxiety disorders. Their non-anxious control subjects had no past or current diagnosable conditions as well as no history of psychotherapy or pharmacological treatment. The proposed cut off score of 53 in our study seems to be higher than that of the previous study including Caucasian subjects. The relatively higher cutoff score in our study may result from different control subjects compared with those in the previous study. As we recruited control subjects who had no history of medical or psychiatric conditions just by thorough history taking, some of them might have hidden anxiety disorders. Thus, the mean PSWQ score of control subjects in our study was higher than that of the previous study, which might lead to the higher PSWQ cutoff score for differentiating Korean GAD patients from control subjects.
Regarding the PSWQ cutoff score of 61 for differentiating GAD from other anxiety disorders, our result was relatively lower than that of previous studies which proposed a PSWQ cutoff score of 65.13,14 In previous studies, Asian GAD patients had higher levels of somatic symptoms and lower levels of psychological symptoms than American GAD patients, and tended to complain of more somatic symptoms such as dizziness and indigestion rather than psychological or cognitive symptoms such as worry or nervousness.15,16 As the PSWQ centers on assessing pathological worry symptoms, the Korean GAD patients in this study might under-report worry symptoms compared with Caucasian GAD patients. These findings support that there may be both ethnic and cultural difference in the symptomatology of GAD, which might lead to the difference in the PSWQ cutoff scores for GAD.
We also found that GAD patients had higher PSWQ scores than patients with anxiety disorder NOS even though there was no difference in BAI scores between the two groups. This finding suggests that the PSWQ is a useful method for differentiating GAD from other anxiety disorders. In other words, pathological worry, among other general anxiety symptoms, should be a core symptom for screening GAD.
Our study has some limitations. Firstly, it included a retrospective study design and a selection bias might affect interpretation of the data. To avoid this bias, we included all patients who were diagnosed as GAD and anxiety disorder NOS in the Samsung Medical Center from 2008 to 2011 in our study. Secondly, we did not use any objective measures to identify psychiatric illnesses in normal control subjects, although their anxiety levels measured with the BAI and PSWQ were relatively very low. As the prevalence rate of anxiety disorders is relatively high in a general population, the recruitment method might lead to some selection bias for making control group. Thirdly, as we included only patients with anxiety disorder NOS in this study, we could not compare the PSWQ scores between GAD patients and patients with other anxiety disorders such as panic disorder, social phobia, specific phobia, or posttraumatic stress disorder. As some symptoms of these anxiety disorders also overlap with GAD symptoms, this limitation might have hindered this study from obtaining an optimal cutoff score for GAD. Finally, although GAD and anxiety disorder NOS are usually known to be highly comorbid with other mood and anxiety disorders, the comorbidity issue might affect the result of this study.
In spite of these limitations, this is the first study to examine the cut off score of PSWQ for Asian GAD patients, compared with patients with anxiety disorder NOS and normal control subjects. We can finally conclude that the PSWQ is a useful method for screening Asian GAD patients, and PSWQ cutoff score for GAD needs to be changed according to the ethnic or cultural background of GAD patients.
Acknowledgments
This study was supported by the Samsung Medical Center Grant CRO 112122. The Samsung Medical Center was not involved in the creation of the study protocol, data analysis, or in writing the manuscript.