Relationship between Problematic Internet Use and Post-Traumatic Stress Disorder Symptoms among Students Following the Sewol Ferry Disaster in South Korea
Article information
Abstract
We investigated the association between problematic internet use (PIU) and post-traumatic stress disorder (PTSD) symptoms in children and adolescents in South Korea. A cross-sectional survey was administered to community students who attended primary, secondary, and high schools in the Jindo area 1–2.5 months after the Sewol ferry disaster. Of the 1,744 respondents, 392 students who were exposed to the disaster, witnessing the rescue work directly, were evaluated. PTSD symptoms were measured using the University of California Los Angeles Post-traumatic Stress Disorder Reaction Index (UCLA PTSD-RI). The severity of impairment caused by excessive internet use was evaluated using Young's Internet Addiction Test. The Center for Epidemiological Studies Depression Scale (CES-D) and State Anxiety Inventory for Children (SAIC) were also used. Logistic regression analysis revealed that PIU was significantly and independently associated with a high level of PTSD symptoms. Our findings suggest that children and adolescents with PIU require intensive follow-up and special care to prevent the development of PTSD symptoms following a disaster.
INTRODUCTION
The Sewol ferry sank off the coast of Jindo Island on the way from Incheon to the southern resort island of Jeju, South Korea, on April 16, 2014. The ferry capsized while carrying 476 people, primarily second-year students from Danwon High School. Among the passengers, 295 people, including 250 high school students, died and nine passengers are still missing. Family members of victims waited for their return at Paengmok Harbor, Jindo Island, which became the base camp for the rescue until the South Korean government ended efforts on November 11, 2014. Jindo residents could witness the rescue work and bereaved family members of the disaster victims at the harbor during the period.
Witnessing a traumatic event can be sufficient for the development of post-traumatic stress disorder (PTSD) symptoms in children and adolescents.12 The type of disaster, pre-disaster functioning, family characteristics, and individual coping strategies have been identified as predictors of PTSD symptoms in children and adolescents.34 However, there is still relatively little information about risk factors and underlying mechanisms in the development of PTSD symptoms. Determining variables that reliably predict PTSD symptoms is important to support the identification of high-risk individuals.
Previous studies have shown that individuals may be more vulnerable to PTSD symptoms if they suffer from addictive problems.56 A study in adults found that individuals with addictive characteristics, such as alcohol abuse, were at higher risk for PTSD.7 A recent study also suggested the importance of routine assessments for substance use disorder among children and adolescents following a disaster, so that the development of disaster-related psychiatric problems, including PTSD, could be prevented.8 Problematic internet use (PIU), conceptualized as “internet addiction,” shares common neurobiological adaptive mechanisms and psychological vulnerability factors with substance addictions.910 That is, in this light of
addiction, PIU may have pathological aspects associated with the development of PTSD symptoms. Thus, we investigated any association between PIU and PTSD symptoms in a sample of children and adolescents who had witnessed rescue efforts associated with a disaster during the acute phase, 1–2.5 months after the event.
METHODS
Study design and participants
This was a cross-sectional survey. It was administered to 1,744 students (813 boys, 931 girls) aged 7–18 years in grades 1–12 from 20 of the 21 schools on Jindo island. Of the 1,744 respondents, 392 (22.4%) who had witnessed rescue work following the Sewol ferry disaster were included in the analysis after the exclusion of incomplete or inappropriate responses on the University of California at Los Angeles Post-traumatic Stress Disorder Reaction Index (UCLA PTSD-RI)11 and Young's Internet Addiction Test (IAT).12 The study was conducted between May 25 and June 3, 2014, 1–2.5 months after the Sewol ferry accident.
The survey was approved by the Ministry of Education, the principal of each school, and the Chonnam National University Hospital Institutional Review Board (CNUH-2014-271). The students and classroom teachers received a written explanation of the procedure and purpose of the study. Informed consent was obtained from all students and parents.
Post-traumatic stress disorder symptoms
We used the nine-item version of the UCLA-PTSD-RI, a self-reported test that provides a quick screen for PTSD symptoms. A previous study found that the mean scores of the nine items were highly correlated with those of the full scale in a sample of trauma-exposed children and adolescents and showed good internal consistency.13 The UCLA-PTSD-RI, a widely used instrument for the assessment of traumatized children and adolescents, evaluates the frequency of PTSD symptoms during the past month. The UCLA-PTSD-RI is scored on a four point scale (0=none of the time, 4=most of the time). We used a Korean version of UCLA-PTSD-RI, translated at the School of Mental Health Resources and Research Center of Korea; it has been used widely in screening South Korean students for PTSD symptoms. In the present study, Cronbach's α was 0.89, indicating excellent internal consistency. According to the UCLA scores, we selected two groups of students: low (the lower quartile with score ≤1) and high PTSD (the upper quartile with score ≥11) symptom groups.
Internet use
The Korean version of Young's IAT was administered to assess PIU among the study participants. The 20-item questionnaire, scored on a five-point Likert scale (ranging from 1, not at all, to 5, always), was used to evaluate the respondents' level of internet use. Subjects with moderate (40–69) to severe (70–100) user scores were defined as having PIU, and the remaining subjects were classified as ‘normal’ internet users. The Korean version of the IAT has been shown to be reliable and valid.14 The students were asked to assess their internet usage before the Sewol ferry disaster on the IAT. The students were also asked to estimate how many minutes a day they used the internet before and after the Sewol ferry disaster. In addition, the students were asked to estimate how many hours a day they used the internet for play before the Sewol ferry disaster. The time of internet use for play was categorized into three groups: <1, 1–2, and >2 h/day.
Sociodemographic and clinical characteristics
Various sociodemographic characteristics were obtained from the students, including their gender, school level, academic achievement, and religion. Self-rated academic achievement was categorized into three levels: good, average, and poor. Depression was measured using the Center for Epidemiological Studies Depression Scale (CES-D).15 The CES-D is a 20-item assessment of depressive symptoms experienced during the past week using a four-point Likert scale ranging from 0 (rarely or none, <1 day) to 3 (most or all, 5–7 days), with higher CES-D scores indicating increasing levels of depression. The reliability and validity of the Korean version of the CES-D have been established.16 The Korean version of the Spielberger State Anxiety Inventory for Children (SAIC) was used to measure anxiety.17 The SAIC is scored on three-point Likert scale (ranging from 0, almost never, to 3, almost always), with total scores ranging from 20 to 60; higher scores indicate greater anxiety.
Statistical analyses
Between-group comparisons of the sociodemographic and clinical characteristics were made according to the level of PTSD symptoms using the χ2 test for categorical variables and the Mann-Whitney U-test for continuous variables that were not normally distributed. The variables determined to be statistically significant by univariate analysis were entered into a logistic regression analysis to investigate independent associations with PTSD symptoms as the dependent variable. The SPSS software (ver. 21.0 for Windows; IBM Corp., Armonk, NY, USA) was used to conduct statistical tests. All statistical tests were two-tailed. p-values <0.05 were considered to indicate statistical significance.
RESULTS
The students' sociodemographic and clinical characteristics according to the level of PTSD symptoms are shown in Table 1. The mean age of the students was 13.4±2.2 years. Among the total 234 students, there were 107 boys (45.7%) and 127 girls. There were 81 primary school students (34.6%), 94 middle school students (40.2%), and 59 high school students. The time spent on the internet before and after the ferry disaster did not differ in the low (t=-0.396, p=0.692) or high PTSD symptom group (t=0.778, p=0.439) (data not shown). We found significant differences in gender, school level, PIU, and levels of depression and anxiety between the low and high PTSD symptom groups. The CES-D and SAIC scores were significantly higher in the high PTSD symptom group. Logistic regression analysis showed that high school, PIU, and depression were strongly and independently associated with PTSD symptoms (Table 2).

Comparison of sociodemographic and clinical characteristics according to the level of PTSD symptoms
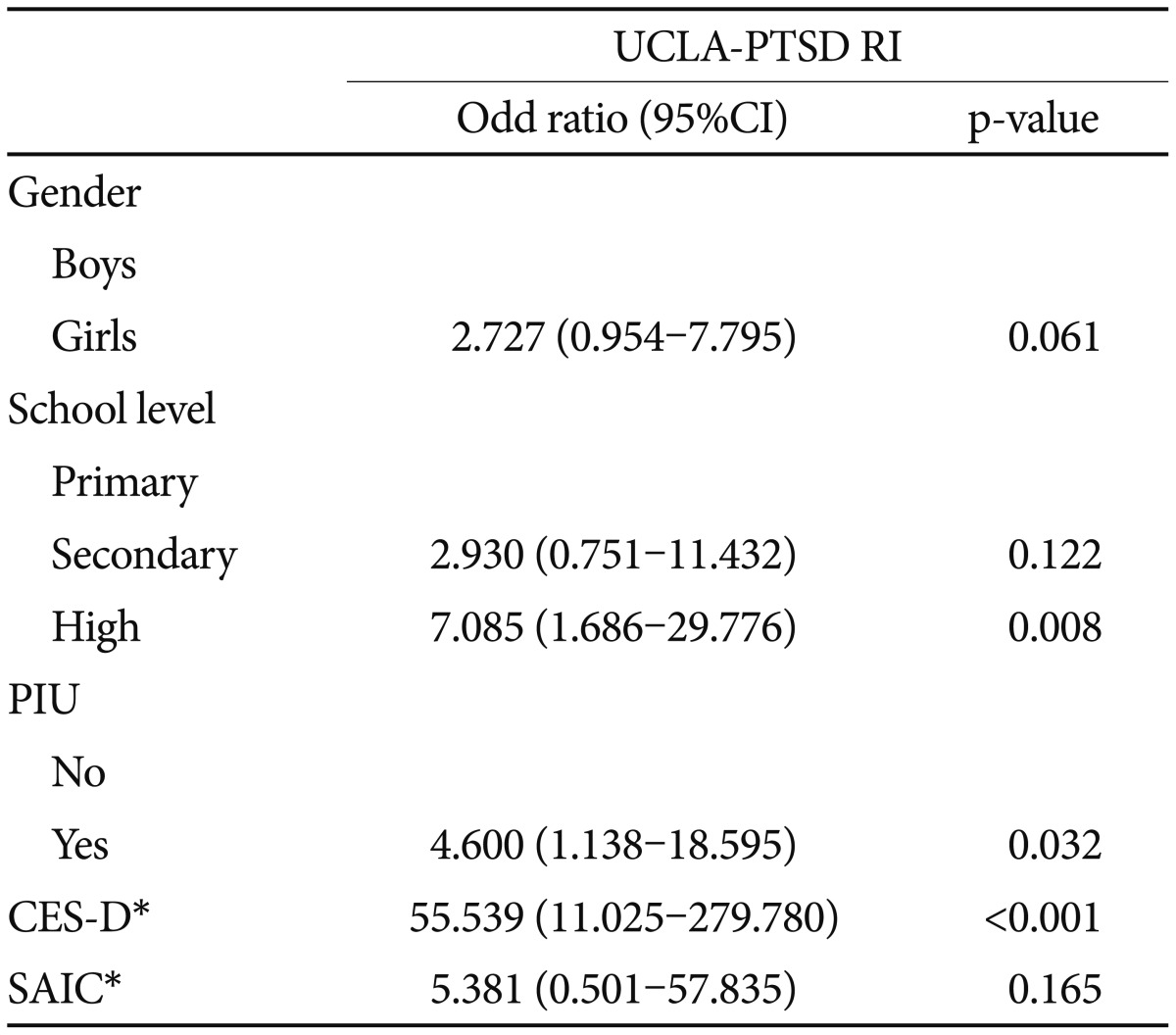
Logistic regression analysis predicting high level of PTSD symptoms
DISCUSSION
To our knowledge, this is the first reported study to identify the relationship between PIU and PTSD symptoms. In this study, individuals who witnessed traumatic events directly, not through media exposure after the disaster, meeting the traumatic event criteria of DSM-5 were investigated.
After adjusting for independent variables, logistic regression analysis revealed that PIU was significantly associated with PTSD symptoms. Internet use among children and adolescents is currently on the rise. Moreover, South Korea has one of the highest rates of high-speed internet penetration worldwide.18 The prevalence of potential PIU among children and adolescents is high, at 10–30%, and increasing annually.19 In this study, our findings showed that PIU, rather than overuse or internet use for play, was associated with PTSD symptoms. This result supports a pathological mechanism in which PIU is associated with PTSD symptoms that goes beyond the amount and specific content of internet use. Several studies have highlighted the potential harmful effects of secondary exposure to disasters via post-disaster media coverage, mainly focused on television. However, any association between the amount of media coverage of disasters and PTSD symptoms remains controversial. Furthermore, the measurement of television as a reflection of media exposure to disasters has limitations in South Korea, where the television screen has been transformed into a multimedia center that includes internet access. From an addiction standpoint, behavioral addiction, such as PIU, is also associated with maladaptive strategies for the process of coping with stressful events.2021 PIU has been associated significantly with one's rumination about threats and avoiding managing stress with passive coping, leading to inefficiency in controlling emotions.2223 In a study of adolescents, samples with PIU reported a greater use of avoidant coping versus normal internet users.24 Individual coping strategies also moderate the influence of the development of PTSD symptoms in trauma-exposed subjects.25 For example, passive coping, such as avoidant coping, can influence peritraumatic dissociation and PTSD symptoms in those exposed to traumatic events negatively.26 Several recent studies have proposed that adaptive strategies for coping with disasters are linked consistently to lower PTSD symptoms in trauma-exposed subjects.27 In particular, during the acute phase of responding to traumatic events, which is similar to the period of our study, coping strategies and emotional reactions interact dynamically.28 Our study showed that depression as well as PIU was positively associated with PTSD symptoms. Previous studies indicated children and adolescents with elevated levels of depressive symptoms are more likely to offer avoidant coping responses in response to stressful situa-tions.2930 Based on prior research, we suggest that the development of PTSD symptoms could be influenced by dysfunctional coping strategies related with the severity of depression.
Thus, the process of the development of PTSD symptoms and the maintenance of PIU may share dysfunctional mechanisms of coping with a stressful event. These underlying character traits in PIU could be essential in the development of PTSD and may have robust associations in trauma-exposed samples. Although the actual mechanism of any moderating effect of maladaptive coping on the association between PIU and PTSD symptoms is not clear, our findings may reflect the potential role of the coping process in contributing to PIU and PTSD and it may be that those with an addictive trait are more likely to present PTSD symptoms, indicating the need for further research in this area.
Additionally, in this study, high school age, the same school level as most of the victims of the Sewol ferry disaster, was independently associated with high PTSD symptoms. This supports the importance of psychological proximity to a disaster in children.3132
In conclusion, our exploratory results suggest that children and adolescents at risk of PIU who are exposed to trauma may need careful intervention to prevent the development of PTSD symptoms following a disaster.
Acknowledgments
This research data collection was supported by Jeollanamdo Jindo office of education.