Sensory Processing Problems in Children with ADHD, a Systematic Review
Article information
Abstract
One of the most common psychiatric disorders in children is attention deficit hyperactivity disorder (ADHD). Its course and outcome are heterogeneous. Sensory processing problems impact the nature of response to daily events. ADHD and sensory problems may occur together and interact. No published review article about sensory processing problems in children with ADHD were found. A systematic search, conducted on Pub-Med (up to January 2010), and Google Scholar, yielded 255 abstracts on sensory processing problems in children including 11 studies about sensory problems in children with ADHD. Sensory processing problems in children with ADHD is not a well studied area. Sensory processing problems in children with ADHD are more common than in typically developing children. Findings do not support that ADHD subtypes are distinct disorders with regard to sensory processing problems. However, co-morbidity with oppositional defiant disorder and anxiety are predictors of more severe sensory processing problems in children with ADHD.
INTRODUCTION
Attention deficit hyperactivity disorder
The symptoms of attention deficit hyperactivity disorder (ADHD) are relatively common in the community sample of children. The rates for boys and girls are 13.6% and 6.5%, respectively.1 This disorder is usually co-morbid with other disorders. More than two thirds of the clinical samples of children with ADHD have at least one co-morbid psychiatric disorder which are more likely to be oppositional defiant and anxiety disorders. This high rate of psychiatric disorders is not just confined to the children but their families also report a high rate of psychiatric disorders.2,3 The rate of psychiatric disorder co-morbidities does not differentiate between ADHD subtypes.4
Sensory processing problems
Sensory processing disorders are impairments in responding to sensory stimuli such as impairments in detection, modulation, or interpretation of stimuli.5 Sensory processing problems impact the responses of children to sensory events in daily life.6 5.3% of the kindergarten children meet screening criteria for sensory processing disorders according to their parental reports.7 One type of sensory processing problem is sensory over-responsivity or sensory hypersensitivity. That is, individuals respond to sensory stimuli in the way that is faster, longer, or more intense than what is expected.8 This response can be towards any types of sensory stimuli. Sensory over-responsivity can be considered as an independent diagnosis.9 For example, a child with tactile sensitivity or defensiveness might be defensive for hair-brushing and/or haircuts because she/he cannot tolerate it easily.
Another form of sensory processing problems is under-responsivity. Individuals with under-responsivity are unaware or they are slow to respond to sensory input. The third type is sensory-seeking, where individuals crave or display interest in sensory experiences.10 Sensory discrimination problems are another type of sensory processing problem characterized by difficulty interpreting the specific characteristics of sensory stimuli.11 There are multiple sensory modalities but they are not separate and interact with each other. For example, sound alters vision or vision alters sound location.12 An example is that when we watch television or movies, we perceive that the voices originate from the actors on the screen while there is a large spatial discrepancy between the origine of sound and the actors.12
The etiology of sensory processing is unknown. Genetic and familial factors have been suggested.11 Others suggest other risk factors such as pre-, peri- and post-natal birth factors such as maternal stress during pregnancy, jaundice, and allergies.13
It is clear that there is an alteration in the neural networks and a possible central role of dopamine for sensory problems that cannot be linked to specific cerebral lesions in children with ADHD.14 One of the prominent neuroanatomical markers for children and adolescents with ADHD is widespread cortical thickness reductions.15 Activities in resting state in sensory and sensory-related cortices in ADHD is significantly more than those of the control group.16 Moreover, there is a connection between perception and action that is impaired in ADHD.17 There are growing published studies about sensory processing problems in children with ADHD. However, the underlying structure and pathophysiology is not well studied and the assessment of sensory profiles of children with behavioral problems in clinical practice is recommended.18
The reason for conducting this systematic review is that there are some studies about sensory processing problems in children with ADHD but there appears to be no current reviews on sensory processing problems in ADHD.
METHODS
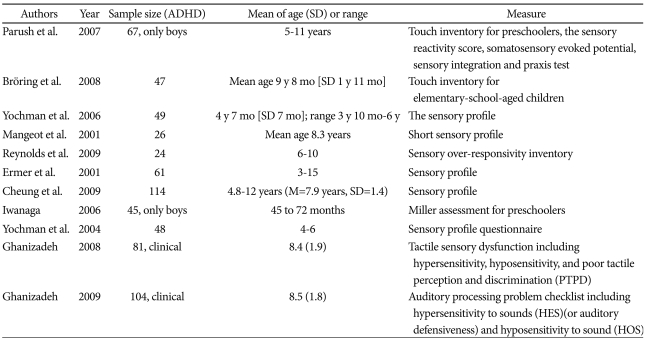
The MEDLINE database was systemically searched for articles published up to January 2010 reporting sensory processing problems in children with ADHD. The keywords used were ADHD, attention deficit hyperactivity disorder, sensory processing problem, sensory processing modalities, sensory processing integration, sensory, reactivity, auditory, tactile, vestibular, olfactory, visual, and profile. The reference section of the identified articles was reviewed. Google scholar database was searched for possible related articles. All of the articles were in English. There was not found any review article about sensory processing problems in children with ADHD. Two hundreds fity five abstracts were retrieved and studied. Eleven articles about sensory problems in children with ADHD were found (Table 1).
Characteristics of studies
RESULTS
Most of the studies were published in recent years. They usually included small samples of children with ADHD (for example,19,20 All of the studies used questionnaire or parent-reported measures. More details about the year of publication, sample size, the age of sample, and the measures used for assessment are displayed I Table 1.
The sensory-motor abilities of ADHD children are less than those of control group.21 Sensory processing problems in children with ADHD are more common than children without ADHD22 and the patterns of sensory modulation in the ADHD are significantly different from typical children.23
The sensory profile of children can discriminate children with autism or pervasive developmental disorder (PDD), children with ADHD, and children without disabilities.22,24
The sensory processing problem in ADHD is reported in both of the physiological and parent-reported measures.19 The sensory processing problem is not gender related but it is associated with age.22
Specific sensory symptoms are correlated with particular behavioral problems such as aggression and delinquency in ADHD. The higher level of sensory problems in ADHD predicts the higher levels of aggression and delinquency.19 The impairment of receiving and processing of sensory information in children with ADHD may cause inappropriate responses at different settings such as school, home and in the community.25
In addition, sensory functioning has a strong correlation with academic achievement and cognitive processing in ADHD.26 Earlier detection and management of sensory processing problems can play an important role for the performance improvement in children with ADHD. The early assessment of sensory-motor skills is suggested to be used for the prediction of academic performance deficits.26
DISCUSSION
Tactile sensory
Children with ADHD have more difficulties in tactile processing.27 The level of tactile defensiveness in females with ADHD is higher than that of males with ADHD. Tactile defensiveness is not part of a familial risk for ADHD because it is specific to children with ADHD and not to their sibling without ADHD.28 Tactile defensiveness is not due to tactile perception impairment but the impairment of central processing of somatosensory information.29
Sensory over-responsivity in ADHD is associated with anxiety. These children have a higher level of anxiety than those ADHD children without sensory overresponsivity and non-ADHD children.20 The hypothalamic pituitary adrenal axis is influenced by tactile sensory overresponsivity in children with ADHD.30 The symptoms of oppositional defiant disorder are predictors in hypersensitivity scores of tactile sensory function in ADHD. This impairment is not related to ADHD subtypes or gender.31 Another study reported that tactile defensiveness in girls with ADHD is more than boys with ADHD and the level of tactile defensiveness in boys was not different from the control boys.28 Two samples of tactile defensiveness are "doesn't like to brush his/her hair or is easily annoyed by it" and "react excessively to small cuts, or bites". "Might not be aware that his/her face or hands are dirty or even his/her runny nose" and "may not be aware that he/she has been touched, except that when he/she has been touched forcefully" are two examples for hyposensitivity to touch.
Balance control and vestibular systems
There are very few reports about balance problems in ADHD.32 Balance performance33 and ability for equilibrium and postural control21 in children with ADHD combined type are more impaired in comparison to typically developing children. More than one third of children with ADHD have poor balance and coordination.34 This balance problem in ADHD is associated with the sensory inputs, the sensory integration, and/or the inhibition of excessive movements.35 Children with combined-type ADHD without learning disorder do not usually benefit from vestibular stimulation.36 More studies considering covariant factors are required to reach a firm conclusion.37
Auditory sensory
Individuals with auditory processing disorders have normal peripheral hearing but they may be unsure about what they hear.38 Difficulty in auditory discrimination or localization and distractibility are other forms of auditory processing disorders.39 Hyposensitivity to sounds or under-registering of sounds can motivate parents seek professional help for their inattentive children. It may seem like a learning disability. Two examples of hypersensitivity to sounds are: "Often pleased by asking people to keep quiet" and "Very sensitive towards sounds which are unheard by others such as humming of refrigerator, clocks ticking, or fans". Two examples of hyposensitivity to sounds are "often irresponsive to oral points or calls" and "seems puzzled about where origin of a sound is". Auditory processing problem in children with ADHD is an ignored research area.40 The auditory processing of children without any disability is better than that in children with ADHD.22 Of course, this difficulty is not specific to ADHD and it cannot differentiate children with ADHD and those with autism.22
The subtypes of ADHD are not different regarding auditory processing problems. However, the co-morbidity of ODD in children with ADHD is a risk factor for auditory processing problems.40 These children are more under-responsive to sounds. Background noise in their classroom should be minimized. Co-morbidity with anxiety predicts hypersensitivity to the sound. Impairment of auditory processing is not gender-related in children with ADHD.40 Considering the co-occurrence of ODD and auditory processing problem, the question is that they are distinct disorders or they are part of a broader problem.
Visual and olfactory function
Stimulants may induce visual oversensitivity or photophobia in children with ADHD.41 Stimulants impact the visual fields in children with ADHD.42 There are only three studies concerning association of olfactory function in children with ADHD. Odor threshold is lower in ADHD than in healthy control subjects and stimulants improve it. However, odor discrimination or identification is not different in ADHD in comparison to the control group.43 Another study reported that the olfactory identification ability of children with ADHD is not as good as healthy controls.44 Prefrontal compromise is suggested as a reason for this inability and ADHD symptoms.44 Stimulants improve the odor sensitivity in ADHD while odor discrimination and identification are not different between ADHD children and control group.43
Sensory processing problems may differentiate ADHD from normally developing children. However, it does not mean that it is specific to ADHD. The sensory profiles of children with ADHD may be similar to other disabilities such as autism.22 Thus, how do we differentiate the different disorders in terms of sensory processing problems? Other assessment characteristics would be required to show up the differences in clinical features between the two groups.
Sensory problems are usually assessed using parents or caregivers reported questionnaires. The Sensory Profile is a widely used parent reported standardized questionnaire. Children's responses to different sensory events in daily life are rated by their parents. It has been used in different samples such as children with ADHD.25 Auditory processing, visual processing, taste/smell processing, body position, movement, touch processing, activity level, and social/emotional responses are the dimensions assessed by this questionnaire.
The parent reported auditory processing problem checklist which is used for assessment of auditory processing problems indicates child's reaction to sounds. Its psychometric properties were reported before.40 The two aspects of auditory dysfunction are hypersensitivity to sounds (or auditory defensiveness) and hyposensitivity to sound (under-registers)40
Tactile sensory dysfunction checklist is an instrument used for measuring tactile dysfunction. It comprises three types of tactile dysfunction including hypersensitivity to touch (tactile defensiveness), hyposensitivity to touch (under-responsive), and poor tactile perception and discrimination.31
ADHD children with sensory oversensitivity usually suffer from other problems such as anxiety.20 Treatment plans for children with ADHD and sensory oversensitivity should include management of other co-morbid psychiatric problems. As parents of children are educated about ADHD symptoms,45 considering the co-morbidity of ADHD and sensory processing problems, they should also be educated about the symptoms and behavioral management of sensory processing problems.46 In a promising report, it is indicated that occupational therapy improves sensory processing problems.5 Moreover, there are some reports showing that sensory processing problems can guide clinicians for pharmacological management of children with ADHD47 or other disorders.48 Although, there are some speculation that some medications may improve sensory problems,49 it is not clear how much can pharmacotherapy improve sensory problems in ADHD. An area that needs to be researched is effectiveness of interventions.
Future studies
Further studies may be conducted with objective measures such as Somatosensory Evoked Potential,29 P300 auditory evoked potentials,50 digital optical motion capture instruments,32 electrodermal reactivity, and Pennsylvania Smell Identification Test.44 Providing more objective measures and laboratory findings improves differentiating sensory processing problems from other disorders or problems. Moreover, there are some reports about the role of genetics on the sensory gating of mid-latency auditory evoked responses.51 So, future studies should investigate the possible role of genetics factors on the sensory processing problems in children with ADHD.
Overall, considering the fact that sensory problems in children with ADHD can impact the behavior and education of these children, it needs to be focused in future studies because it is not widely studied. More developed, valid, and reliable measurements are required. Many of the published studies have only focused on one or few sensory processing types. Future studies should include investigation of different sensory modalities. Since ADHD is not a homogenous disorder and previous studies have usually included just one type of ADHD, it is recommended that further studies include different types of ADHD and also consider psychiatric co-morbidities in children. Probably, ADHD children tend to have more than one type of sensory processing problems. It can guide clinicians for a better classification of ADHD according to the types of problem, severity, and duration. Our knowledge about association of sensory problems and age, gender, socioeconomic status of family, co-occurrence with medical and psychological conditions, parent-child interaction, mental age, severity of ADHD, and environmental factors such as environmental noise needs to be increased. Studies including measurement of possible biomarkers such as brain neurotransmitters, structural and functional aspects of sensory processing problems should be investigated.
Most of the published articles regarding sensory problems relay on parent reports, considering that parents of these children usually suffer from psychiatric disorders such as depression and anxiety. It is not studied if parental psychiatric problems may impact on their report for children's sensory processing problem. Further studies may investigate if the sensory processing problems are behavioral biomarkers for ADHD. In other words, both basic and clinical sciences about it need more studies. Research in this field may help to re-organize our understanding from ADHD and its diagnosis. Possible children and maternal risk factors for sensory problems need to be studied.
CONCLUSION
Sensory processing problems in children with ADHD is not a well studied area. There are many reported limitations for the published studies. So, it is difficult to reach a firm conclusion due to the limitations. However, it is reported that the sensory processing problems are more common in children with ADHD than in typically developing children. This article emphasizes that sensory processing problem in ADHD need to be further studied. Treatment protocols for management of this problem should be provided and researched.