Decreased Serum Brain-Derived Neurotrophic Factor Levels in Elderly Korean with Dementia
Article information
Abstract
Objective
The primary purpose of this study was to investigate the differences in the serum brain-derived neurotrophic factor (BDNF) level between elderly Korean people over 65 years with and without dementia.
Methods
171 individuals over 65 years were enrolled in this study. Screening for cognitive impairments was carried out using the Mini-Mental Status Examination-Korean version (MMSE-KC). One hundred thirty-two subjects scored below 1.5 standard deviations (SD) of the mean MMSE-KC score, and these were evaluated using the Consortium to Establish a Registry for Alzheimer's Disease, Korean version (CERAD-K) and the Geriatric Depression Scale (GDS). The Clinical Dementia Rating Scale (CDRS) and the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) diagnostic criteria were used for further evaluation. Subjects with a CDRS score of 1 or higher were classified as having Alzheimer's disease (AD), and subjects with a CDRS score of 0.5 were classified as having a mild cognitive impairment (MCI). Subjects with a CDRS score of 0 were classified as having aging-associated cognitive decline (AACD). Serum BDNF levels were analyzed using the enzyme-linked immunosorbent assay (ELISA) method.
Results
The serum BDNF levels were significantly lower in the subjects with MCI and AD compared with the healthy controls (p<0.01). A significant correlation was found between the total MMSE-KC score and serum BDNF level (r=0.295; p<0.01). However, no significant correlation was observed between the severity of MMSE-KC and the total GDS score. A significant difference was found in the total score of GDS between the AACD group and subjects with AD (p<0.05).
Conclusion
This study suggested that BDNF might be involved in the pathophysiology of cognitive decline in elderly people.
Introduction
Dementia refers to a disease that causes the deterioration of general memory, speech, executive function, visuospatial function, and other cognitive functions. Patients with dementia also manifest behavioral disturbances, personality change, and emotional disturbances, and these symptoms often cause social, professional, or occupational impairment.1 Due to the rapid increase in the elderly population, the number of patients with dementia is also rising sharply, and the consequent problems affect not only the patients themselves but also their families, creating wider social problems.2 It has been reported that Alzheimer's disease (AD) accounts for approximately 50% of all dementia.3 The characteristics of AD are the formation of neuritic plaques due to the deposition of beta-amyloid protein and the formation of neurofibrillary tangles in the br ain. Blasko and Grubeck-Loebenstein4 reported that 10-20 years prior to the development of AD, impairment of brain metabolism was already developing. It is thought that risk factors of AD include age, sex, education level, family history, head trauma, a history of depression, and smoking.5
However, according to recent studies, neurotrophins such as brainderived neurotrophic factor (BDNF) might also be associated with the pathogenesis of AD.6-9 Hashimoto et al.11 reported that the BDNF signaling pathway and MetBDNF may affect memory and hippocampal function in humans.
BDNF polymorphism could be a risk factor for rapid disease progression in preclinical AD.10,11 In postmortem brain analyses of patients with AD, the level of BDNF messenger RNA (mRNA) in the hippocampus and the cortex was decreased.12,13 The reduction of the BDNF level in the hippocampus and the cortex is thought to induce neurodegenerative changes in the brain.14 Yasutake et al.15 reported that serum BDNF concentrations were significantly lower in subjects with severe AD than in either healthy controls or subjects with vascular dementia. Gunstad et al.16 reported that higher serum BDNF levels were associated with better neuropsychological function in healthy older adults.
Yu et al.17 reported that reduced BDNF levels may play a role in the pathophysiology of amnestic mild cognitive impairemnt. In clinical studies, increased BDNF serum concentrations have been observed following treatment with lithium and donepezil.18,19
BDNF is a nerve growth factor that is expressed widely in the adult mammalian brain, and it has been shown to play an important role in the development and survival of neurons. BDNF is a subject of interest in the study on the pathogenesis of neurodevelopmental or neurodegenerative disorders.20,21
The incidence of depression in individuals with AD has been reported to be 23-51%.22 A correlation is known to exist between cognitive function and depression.22-24 Depression, therefore, might be associated with a deterioration of cognitive function.25-27 So depression may have a negative effect on cognitive function and on the ability to perform the functions required for daily life in patients with AD.2 Laske et al.28 observed inverse correlations between serum BDNF concentrations and depressive symptoms. In this study, therefore, we investigated whether serum BDNF concentrations differed between a normal group, an aging associated cognitive decline (AACD) group, an mild cognitive impairment (MCI) group, and an AD group.
We also evaluated the correlation between depression and serum BDNF concentration and the differences in serum BDNF concentration according to the severity of depression.
Methods
Subjects
Six hundred twenty-eight subjects aged 65 years or older participated in this study. The subjects were patients who were able to participate in the project voluntarily during the research period, and a written consent was obtained. The study protocol was approved by the Institutional Review Board (IRB) of Busan Paik Hospital, Busan. A dementia screening test was performed using the Korean version of the Mini-Mental State Examination (MMSE-KC), and for the final diagnosis of AD, the diagnostic standard of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) and that of the National Institute of Neurologic and Communicative Disorders and Stroke and Alzheimer's Disease and Related Disorder Association (NINDS-ADRDA) were used.29,30 A total of 371 subjects agreed to blood sampling to evaluate serum BDNF levels. A 5-cc sample of venous blood was collected from subjects between 11 : 00 and 24 : 00 h each day. Subjects with or psychotic features or history of depressive episodes according to DSM-IV criteria were excluded from the study. In addition, subjects who had clinically significant physical abnormalities based on both physical and laboratory examination or who had a history of organic brain abnormality or psychotropic drug misuse were excluded from the study.
Methods
A screening test for dementia was performed on all subjects using the MMSE-KC. One hundred subjects whose MMSE-KC scores were within 1.5 standard deviation (SD) of the mean were classified as "normal", and no further tests for dementia were performed on these subjects. Thirty-nine subjects with MMSE-KC scores above 25 were selected as the normal control group. One hundred thirtytwo subjects had MMSE-KC scores more than 1.5 SD above the mean and underwent further, more comprehensive examinations. These comprehensive tests were performed using two testing steps. The first was the Korean version of the Consortium to Establish a Registry for Alzheimer's Disease (CERAD-K) neurocognitive battery, and the second was the full version of CERAD-K, which was administered by psychiatrists.31 Subjects were classified according to their score on the Clinical Dementia Rating Scale (CDRS), which was a part of the second test. Forty-four subjects were classified as the 0-point group, 41 subjects were classified as the 0.5-point group, and 47 subjects formed the group higher than 1 point.
Finally, members of the group with CDRS higher than 1 point were evaluated by psychiatrists using the diagnostic standards of DSM-IV and NINDS-ADRDA, and all members of the group were diagnosed with AD. Previous studies have reported that some individuals with a CDRS score of higher than 0.5 may be in the initial stages of AD; however, in our study, they were all classified as having MCI.32
The diagnosis of MCI was performed using the diagnostic criteria proposed by Petersen et al.33 These diagnostic criteria were as follows. 1) Subjects should have memory-impairment problems identified by informants, 2) in comparison with their peers, subjects should have memory impairment, 3) relatively speaking, general cognition should be conserved, 4) the ability to perform daily living activities should be conserved, and 5) they should not be diagnosed as having dementia. Among the subjects, those with MMSE-KC scores less than 1.5 SD from the mean were classified as "normal", and therefore, comprehensive tests were not performed on them. However, these subjects may have had MCI. The subjects with CDRS scores of 0 were not diagnosable as having MCI. However, the MMSE-KC scores adjusted for age and schooling were higher in these subjects than in others, by 1.5 SD; thus, they were considered to belong in the AACD group.
The CDRS uses six detailed categories to evaluate cognitive function and all areas of social function in subjects with dementia. The categories are memory, orientation, determination and ability to solve problems, social activity, home life and hobbies, and hygiene and grooming.32 CDRS scores can be represented according to two different methods using scores in the above six categories. The first method is to calculate the "Sum of Boxes (CDR-SB)" by adding the scores of all six categories. The second method is to determine the global CDRS score based on memory. According to this method, a CDR score of 0 indicates no dementia (none), and a CDR score of 0.5 indicates questionable dementia. A CDR score of 1 represents mild dementia, 2 indicates moderate dementia, 3 indicates severe dementia, 4 suggests profound dementia, and a CDR score of 5 implies terminal dementia. While evaluating CDRS, raters must be careful to evaluate only that functional deterioration caused by cognitive impairment. Functional deterioration caused by physical conditions such as stroke or social and emotional problems should not be considered.34
For the evaluation of depression, the Geriatric Depression Scale (GDS) was used. This scale consists of 30 questions and has previously been applied very usefully as a screening test for geriatric depression.35 In this study, the Korean version of the Geriatric Depression Scale (GDS-K) was used.36 The GDS-K was adopted during the second step of testing, and subjects with total GDS-K scores higher than 20 were considered to have depression.36
Measurement of serum brain-derived neurotrophic factor concentration
Venous blood samples (5 mL) from the upper arm of each subject were collected in anticoagulant-free tubes between 08 : 00 h and 12 : 00 h. The samples were incubated at room temperature for 1 h followed by 1 h at 4℃ before the serum was isolated. Samples were then centrifuged at 2,000× g at 4℃ for 10 min. The supernatants were transferred to an Eppendorff tube, and the amount of BDNF was measured using enzyme-linked immunosorbent assay (ELISA) kits (Promega, Madison, WI, USA). Monoclonal anti-mouse-BDNF antibody was added to 96-well plates and they were incubated at 4℃ for 12 h. The next day, the plates were washed with a wash buffer (20 mM Tris-HCl pH 7.6, 150 mM NaCl, 0.05% Tween 20), blocked for nonspecific binding, and incubated at room temperature for 1 h After washing, BDNF standards and samples were added to the wells, and plates were incubated for 2 h at room temperature. The anti-human BDNF antibody was then added and incubated for 2 h at room temperature. After washing, the anti-IgY antibody conjugated to horseradish peroxidase was added and incubated for 1 h at room temperature. Any unbound conjugate was removed by washing. The solution was incubated with a chromogenic substrate, and the reaction was stopped using 1 N hydrochloric acid. BDNF concentration was measured at 450 nm using a microplate reader (SLT Spectra; SLT Instruments, Salzburg, Austria).
Statistical analysis
Chi-square tests and/or analysis of variance's (ANOVA's) were conducted to assess the demographic data. An ANOVA was used to analyze differences in serum BDNF concentration between the normal, AACD, MCI, and AD groups. We also used an ANOVA to assess differences in serum BDNF concentration according to the severity of the depression. Pearson's correlation test was used (p<0.05) to assess correlations among MMSE-KC scores, severity of depression, and serum BDNF concentration. The Scheffe method was used for post-hoc analysis.
Results
Demographic data
Educational level was significantly lower in the AD group than in any of the other groups (p<0.01). The mean MMSE-KC score of the AD group was significantly lower than that for any other group (p<0.01)(Table 1).

Demographic and clinical data of subjects
Cognitive impairment and serum brain-derived neurotrophic factor concentration
The average concentration of serum BDNF in the normal group was 27.9±6.9 ng/mL. In the AACD group, average concentration of serum BDNF was 24.2±7.4 ng/mL; in the MCI group, it was 22.8±6.3 ng/mL; and in the AD group, it was 22.9±5.0 ng/mL. In the MCI and AD groups, average serum BDNF concentration was significantly lower than that in the normal group (p<0.01)(Figure 1).
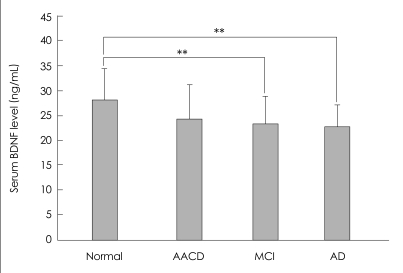
Serum BDNF levels of subjects. **p<0.01. BDNF: brain-derived neurotrophic factor, AACD: age-associated cognitive decline, MCI: mild cognitive impairment, AD: Alzheimer's disease.
Cognitive impairment and depression
The average GDS score of the AACD group was 19.5±7.2, the average score of the MCI group was 22.4±6.0, and the average score of the AD group was 23.3±4.9. The average GDS score of the AD group was significantly higher than that for the AACD group (p<0.05) (Figure 2). The GDS score of the normal elderly group with MMSE-KC scores higher than 1.5 SD from the mean was not evaluated.
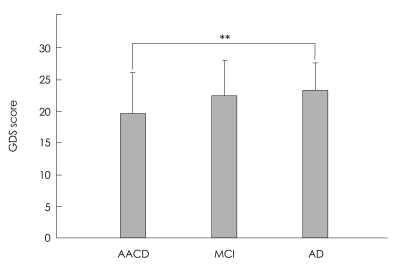
Mean GDS scores of subjects with MMSE-KC score 1.5 SD below. **p<0.01. GDS: geriatric depression scale, MMSE-KC: Mini Mental State Examination of Korean version, SD: standard deviation, AACD: age-associated cognitive decline, MCI: mild cognitive impairment, AD: Alzheimer's disease.
Depression and serum brain-derived neurotrophic factor concentration
In the 34 subjects with depression, the average concentration of serum BDNF was 23.3±6.1 ng/mL, whereas the average BDNF concentration among the 98 cases in the group without depression was 22.4±6.8 ng/mL; no significant statistical difference between the two groups was found (Figure 3).

Serum BDNF levels in the two groups with (GDS≥20) or without severe depression (GDS<20). BDNF: brain-derived neurotrophic factor, GDS: geriatric depression scale.
Korean version of the Mini-Mental State Examination score and serum brain-derived neurotrophic factor concentration
A correlation was observed between MMSE-KC score and serum BDNF concentration (r=0.295; p<0.01)(Figure 4).
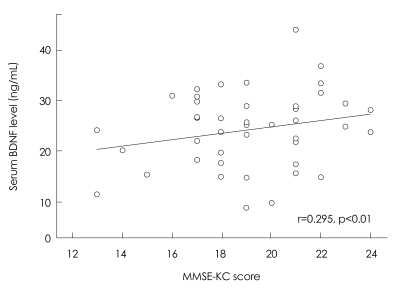
Correlation between serum BDNF levels and total scores of MMSE-KC in all subjects. BDNF: brain-derived neurotrophic factor, MMSE-KC: Mini Mental State Examination of Korean version
Korean version of the Mini-Mental State Examination score and depression
In subjects with MMSE-KC scores of 1.5 SD below the mean, an analysis of the relationship between MMSE-KC scores and GDS scores showed no significant correlation.
Discussion
It has been reported previously that BDNF can cross the blood-brain barrier (BBB), and in animal studies, a positive correlation between the concentration of BDNF in the serum and in the cerebral cortex has been shown.37-39 Therefore, it could be inferred that a change in BDNF in the central nervous system may be associated with a corresponding change in serum BDNF.12
In this study, the correlation between cognitive impairment and changes in serum BDNF concentration was evaluated. We also investigated the possibility of a correlation between cognitive impairment and depression. We found that the more severe the cognitive impairment was, the greater the reduction of serum BDNF concentration tended to be. This finding is similar to previous reports.12 According to recent studies, neurotrophic factors such as BDNF are associated with the pathophysiology of AD.40 In postmortem analyses of the brains of patients with AD, BDNF concentrations in the temporal cortex and the hippocampus have been found to be decreased, as have BDNF concentrations in the frontal cortex.41,42 In addition, it has been reported that the deposition of beta-amyloid protein is involved in the synthesis of BDNF and signal transduction, resulting in a blockage of, synaptic function and accelerated neuronal degeneration.40 Such results support the hypothesis that a reduction of BDNF concentration is involved in the etiology of AD.
Numerous studies have reported that after an ischemic brain injury, BDNF concentrations in the cranial cortex and the number of neurons in the hippocampus were increased.43-45 Such results strongly suggest that BDNF plays a neuroprotective role in ischemic brain injury. In a postmortem analysis of an AD brain, BDNF concentration was also found to be increased. This study also hypothesized that the BDNF concentration was increased by a compensation mechanism.46 Laske et al.14 showed that in patients with mild Alzheimer-type dementia, serum BDNF concentration was higher than in a healthy control group.12 They assumed that BDNF concentration was elevated temporarily as a compensatory mechanism at the initiation of degenerative changes, and thus, serum BDNF concentration was higher in the mild AD group than in the normal group. In our study, most patients with AD were mild cases, and compared with the normal group, their serum BDNF concentration was lower. The result of our study contradicts the above result and thus does not support the compensation mechanism theory described above. However, our study did detect a positive correlation between MMSE-KC score and serum BDNF concentration, which supports previous findings.12 Therefore, the result of our study supports the hypothesis that a reduction of BDNF concentration is associated with a deterioration of cognitive function.40
We found that the average GDS score in the AD group was significantly higher than that in the AACD group. It is widely accepted that depression can be severe in individuals with AD.22,47 It has also been reported that depression may be a risk factor for the development of AD.48 However, in the present study, no significant difference in average GDS score was found between the MCI and AD groups.
Generally, it could be predicted that depression would be more severe among individuals in the MCI group than among those in the AACD group, and it has been reported that in subjects with MCI and accompanying depressive symptoms, the prevalence of AD is increased.49 Depressive symptoms have a negative effect on cognitive function and are therefore sometimes referred to as pseudodementia.50-52 On the other hand, it has been also reported that neuronal degeneration progresses more rapidly in the brains of subjects with AD.53
In the present study, no correlation was found between MMSE-KC and GDS scores. This finding contradicts previous studies showing that depressive symptoms are associated with a deterioration of cognitive function.22-24,54 A reason for this discrepancy could be that in this study, GDS was not evaluated for subjects with MMSE-KC scores of more than 1.5 SD from the mean, so correlations between the two groups could not be examined. In addition, the tests used in this study to assess cognitive function and depressive symptoms are used widely for screening tests, and thus in future research, correlations should be examined by applying more accurate and objective evaluation tools. Because of these limitations, any correlation between deterioration of cognitive function and depression could not be elucidated in our study.
A comparison of serum BDNF concentration according to severity of depressive symptoms revealed no significant differences in this study. This contradicts the finding of a previous study, that in a group with depression, serum BDNF concentration was lower than in the healthy control group.55 We found no correlation between depressive symptoms and serum BDNF concentration; nonetheless, the deterioration of cognitive function correlated with serum BDNF concentration. Thus, regardless of the presence or absence of depression in subjects with AD, BDNF concentration was decreased. This supports the hypothesis that a reduction of BDNF influences the deterioration of cognitive function. In this study, it has been suggested that a reduction of serum BDNF concentration may be viewed as a biomarker of the deterioration of cognitive function.12
The limitations of this study are as follows. In the group with MMSE-KC scores lower than 1.5 SD below the mean, CDRS was not evaluated, and thus, some MCI patients were excluded from the study. Because GDS was not measured in this group, the correlation between depression and cognitive impairment could not be assessed accurately. In addition, classification of cognitive impairment is generally applied to cases lower than 1.0 SD from the mean, but in the present study, the AACD group was classified as those with a score lower than 1.5 SD from the mean.55 In addition, as mentioned above, some initial-stage AD patients are thought to have been included in the group with a CDRS score lower than 0.5; yet, in our study, all these subjects were classified as the MCI group.
The results of our study support the hypothesis that BDNF concentration is involved in the pathophysiology of AD. Serum BDNF concentration among individuals varies greatly; nevertheless, a reduction of BDNF concentration in an individual may be applied as a biomarker of AD. In our study, a trend toward severe depression was detected in subjects with AD but not in MCI patients.
However, the correlation between the severity of depressive symptoms and BDNF concentration could not be elucidated. Further research is required to reexamine this issue using supplementary research methods and more accurate evaluation tools.