INTRODUCTION
Parkinson's disease (PD) has long been well known for its association with progressive cognitive decline, with one third of them eventually diagnosed with dementia.1 Mortality rates of PD patients with dementia are significantly higher than those without dementia, with 3 years shorter life expectancy when compared with those without dementia.2 Therefore, early detection of cognitive decline with timely intervention has become of great importance for patients and clinicians.
Extant studies have adopted various modalities to find predictors of Parkinson's disease dementia (PDD). Two large-scale cohort studies have indicated that akinetic type of PD, hallucinations, increasing age, deficits in semantic fluency and failure to draw intersected pentagons have significant association with the risk of future PDD development.34 Motor symptom severity and apathy have also been reported to be able to predict cognitive decline in PD patients.45 In neuroimaging studies, a close association between Alzheimer's disease (AD) pathology demonstrated by magnetic resonance imaging (MRI) and deficits in cognitive performances of PD has been delineated.6 Moreover, cortical amyloid burden has been purported to be able to predict the rate of evolving into dementia in PD patients.7 Genetic studies have indicated the possibility of increased risk of dementia in Apolipoprotein ╬Ą2 allele carriers and microtubule-associated protein tau (MAPT) genotype carriers.48
Relatively scarce studies have been performed to demonstrate marked amyloid deposition in PDD patients utilizing in vivo amyloid imaging. Here, we present a case of PD patient with visual hallucinations and significant amyloid burden evidenced by beta-amyloid imaging, with pronounced cognitive impairment demonstrated by neuropsychological tests. There is a paucity of evidence on the clinical application of beta-amyloid imaging in PD patients, and the present case report will add another dimension to imaging diagnosis of cognitive decline in PD. In addition, a retrospective review of clinical course and diagnostic processes in this patient will raise questions on possible predictors of cognitive decline in PD. As with treatment approaches, several recent suggestions on the management of visual hallucinations in PD patients will be discussed.
CASE
A 75-year-old female patient visited our clinic with complaints of recurrent visual hallucinations of animals and human figures. She had been diagnosed with PD for 5 years with bradykinesia and both hand tremors as incipient symptoms in a neurosurgical clinic. Other medical diagnoses in her past history included hypertension, hyperlipidemia and osteoporosis. She had been taking medications including levodopa/carbidopa/ entacapone 150/37.5/200 mg twice a day, and 2 mg of ropinirole daily to control parkinsonian symptoms. She started to complain recurrent visual hallucination 4 years after the diagnosis of PD. Those visual hallucinations were vivid while disturbing, evoking anxiety and often sleep disturbance in the patient. 12.5 mg of quetiapine at night was prescribed to ameliorate the hallucinations but to no avail. Considering the degree of anxiety and the potential behavioral consequences of visual hallucinations she was experiencing, she was admitted to a psychiatric ward for more proper diagnosis and management.
Upon her psychiatric admission, neurological examination revealed masked face without tremors, moderate rigidity, bradykinesia, stooped posture, decreased arm swings and narrowbased gait with short steps. A neuropsychological test battery was used to test the patient's cognitive status. She scored 16 in Mini-mental status examination, 1 in Clinical dementia rating scale (CDR), and 3.5 in Clinical Dementia Rating-Sum of Box score (CDR-SB).910 In addition, she scored 25 in Neuropsychiatric Inventory (NPI),11 with major scores centered on symptoms of hallucination, depression, anxiety and apathy. Results from the Seoul-Instrumental activity of daily living (S-IADL) indicated score of 8,12 which indicated that the patient had been experiencing mild impairments in instrumental activity of daily living. A Korean version of the Consortium to Establish a Registry for Alzheimer's Disease Assessment Packet (CERAD-K) was used to assess the patient's cognitive function.1314 Results revealed marked impairments in Korean Boston naming test, word recognition and recall tests as well as constructional recall test, all falling below 5thpercentile scores13 (Table 1).
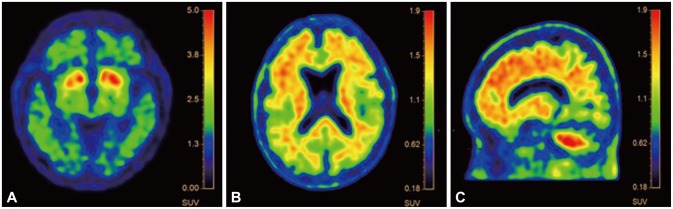
Brain MRI revealed marked medial temporal lobe atrophy (grade 2 by medial temporal lobe atrophy visual rating scale) with global cerebral atrophy (grade 1 by cortical atrophy scale) and periventricular, deep white matter hyperintensities (grade 2 by Fazeka scale)151617 (Figure 1). A fluorodopa F18 positron emission tomography (PET) was implemented to confirm the diagnosis of PD in the midbrain after discontinuing dopaminergic agents for three days. Decreased activity of both posterior portions of putamina was noted, and mild decrements in both caudate activities were found (Figure 2), concordant with the PD pathology. Patterns of the patient's cognitive decline fulfilled the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association Alzheimer's (NINCDS-ADRDA) criteria18 for possible Alzheimer's disease while mixed etiologies, making the patient a good candidate for amyloid PET imaging. 19 Amyloid imaging with 18F-florbetaben was performed to acquire images of cortical diffusion in the patient (Figure 2). Brain beta-amyloid plaque load (BAPL) was found to have a score of 3, indicating pronounced amyloid load.20
To control her visual hallucinations, increased doses up to 100 mg of quetiapine was applied, and antiparkinsonian drugs (levodopa/carbidopa/entacapone 150/37.5/200 mg and 2 mg of ropinirole) were discontinued to exclude the effect of dopaminergic agents on visual hallucination. However, there was no improvement in her symptoms. Significant distress due to oversedation as side effect of quetiapine was found. Her parkinsonian symptoms started to emerge after discontinuing those drugs, including persistent rigidity and bradykinesia resulting in mobility limitations. Alternative prescription was considered for her medication regimen. Her previous antiparkinsonian medications were discontinued, and instead, 100 mg of levodopa and 25 mg of carbidopa were prescribed. The patient was required to take 1.5 tablets 3 times a day. In addition, 6 mg of paliperidone was used, which was soon discontinued due to marked aggravation in rigidity and postural instability. To target her progressive memory decline, 9 mg of rivastigmine patch was prescribed, and the patient experienced reduction in frequency of visual hallucinations. As a result, her anxiety subsided, and the dose of rivastigmine was increased up to 18 mg upon her discharge after one month of psychiatric admission.
DISCUSSION
Previous literatures have repeatedly reported the clinical and pathological overlaps between AD and PD pathologies. Some studies have demonstrated that the two neurodegenerative diseases share etiological basis. Linkage between presenillin 1 and alpha-synuclein has been elucidated in one study,21 whereas genetic polymorphisms and disruptions in iron homeostasis have been suggested as possible culprits.22 Oxidative damage amplified by mitochondrial derangement has been purported to be possible cause of amyloidogenesis and neuronal damage in both AD and PD.22 In addition, neuronal losses in locus coeruleus and disabled modulatory role of nicotinic receptors could also explain the shared clinical pictures of AD and PD.22 Although the aforementioned overlaps complicated the diagnostic process, pondering over the etiological basis for the cognitive decline evident in the patient, we focused on the disparities in the cognitive impairment patterns of AD and PDD. Patients with PDD and dementia with Lewy bodies (DLB) tend to display more severe impairments in visual perception, recognition, constructional recall as well as in attention and fronto-executive function when compared with AD patients.23 Meanwhile, AD, PDD and DLB patients can equally show disabilities in semantic memory.23 The cognitive profile of our patient demonstrated marked impairments in semantic memory, word recognition, and constructional recall test, which were concordant with the cognitive characteristics of PDD and DLB. The patient had been suffering from Parkinsonian symptoms long before the emergence of cognitive decline, which made our conclusion geared towards the diagnosis of PDD.
As with substantial AD pattern of cortical atrophy and high cortical amyloid burden evident in the patient, they offer some important and valuable clinical implications. A previous study has suggested that cortical atrophy resembling AD could be a valuable predictor of cognitive decline in cognitively normal PD patients.6 Significant cortical and hippocampal atrophy in the patient might represent risks of PDD that the patient had harbored before conversion to dementia. Mixed reports exist on the understanding of the role of cortical amyloid deposition. While infrequent amyloid deposition was noted in PDD patients when compared with DLB patients in one study,24 several literatures have consistently reported associations between cognitive decline and cerebral amyloid retention in PD without dementia.252627 The marked cognitive impairment in this present case might have been foretold long before the manifestation of actual symptoms.
Meanwhile, visual hallucinations in PDD patients have been interpreted from multidimensional aspects. Presence of hallucinations can expedite the rate of cognitive deterioration in PD patients.28 An approximately 20% of PD patients have been reported to have visual hallucinations, with marked cognitive impairment and longer duration of illness as predictors.29 Hallucinations not only could predict the rates of cognitive decline, but also could predict the severity of cognitive impairment.30 Along with the bidirectional relationship between visual hallucination and cognitive decline in PD patient, a causal relationship between the two clinical entities has been delineated. Disruptions in networks involved in attentional control,31 along with perceptual disturbances originating from faulty processing of visual information are thought to be important causative factors of visual hallucinations in PD.23 Impairments in detailed recollection of events have also been purported to be contributors to the emergence of visual hallucinations.32 Attempts have been made to integrate various suggested causes of visual hallucination into theoretical models with regard to anatomical correlates.33
Visual hallucinations from dopaminergic agents in PD have been effectively controlled by quetiapine in several studies, but our patient was not responsive to quetiapine.343536 Some mixed results have been reported on the antipsychotics treatment of visual hallucination in PD patients.37 As with antidepressants, two recent case reports mirtazapine improving visual or auditory hallucinations have been notable, without side effects of aggravation in patients' motor symptoms.3839 Non-pharmacological interventions yielded varying results. Case series enlisting application of electroconvulsive therapy (ECT) in PD patients with treatment-resistant psychotic symptoms have been delineated, and use of ECT in this group of patient could be worthy of attempt.40 With reports of low frequency transcranial magnetic stimulation (TMS) suppressing the activity of occipital cortex,4142 application of TMS sounds feasible, but more evidences are needed.
Regarding the treatment approaches of visual hallucinations in this case, rivastigmine has been shown to be effective in controlling both cognitive symptoms and visual hallucinations in dementia associated with Parkinson's disease.4344 The patient in this case also demonstrated amelioration of symptoms with the titration of rivastigmine. Previous studies4546 have demonstrated the efficacy of anticholinesterase inhibitors as a whole in abating visual hallucinations and other neuropsychiatric symptoms associated with dementia. They have suggested that the effect of acetylcholinesterase inhibitors on visual hallucination of PDD patients might be due to increases in cholinergic neurotransmission resulting in improvements in attention and visual information processing, in accordance with the aforementioned discussion on the etiopathogenesis of visual hallucinations in PD patients.4546
Further studies will be needed to find predictors of cognitive decline and their association with PD pathology. More clinical trials are required to establish a more standardized treatment approach for visual hallucinations and cognitive dysfunction frequently present in PDD patients.