INTRODUCTION
Obsessions are recurrent and persistent thoughts, impulses, or images that are experienced as intrusive and inappropriate, causing marked anxiety or distress.1 Obsessions are one of the major symptoms of obsessive-compulsive disorder (OCD), and it has been suggested that obsession-like thoughts can be observed in nonclinical populations as well.2 Mental intrusions or intrusive thoughts are the terms that have been used for nonclinical obsession-like thoughts. These thoughts are similar in form and content to clinical obsessions, but the latter are more frequent, anxiety-provoking, and uncontrollable than mental intrusions of nonclinical individuals.3 It has been suggested that a nonclinical mental intrusion escalates to a clinical obsession when individuals appraise the mental intrusion as having important meaning to them (e.g., potential threats) and try to reduce the anxiety induced by the negative appraisals with specific neutralizing responses.4 The more individuals appraise certain intrusive thoughts as meaningful to themselves and try to control those thoughts, the more they experience the mental intrusions.5 The frequency of mental intrusions is an important index of the possibility that a nonclinical mental intrusion escalates to a clinical obsession,5 and therefore, properly measuring the frequency of mental intrusions in nonclinical individuals is crucial for preventing manifestations of OCD.
Another important factor that should be considered is the content of mental intrusions. Mental intrusions have various contents (e.g., aggressive thoughts, sexual thoughts, contamination related thoughts, and accident-related thoughts), which are related to cognitive appraisals and neutralization strategies.6 However, there are few models that have considered the contents of mental intrusions. A taxonomic model proposed by Lee and Kwon6 is unique in that it classifies mental intrusions/obsessions based on the differences in their contents, cognitive appraisals, neutralization strategies, trigger stimuli, and the perceived rationality of the thought contents. The model classifies mental intrusions into two subtypes: autogenous obsessions (AOs) and reactive obsessions (ROs). AOs are highly aversive and unrealistic mental intrusions that usually take the form of thoughts, images, or impulses. The themes of AOs are centered primarily on unacceptable aggression, sexual behavior, and blasphemy. Further, AOs tend to occur without clearly perceived antecedents. ROs, in contrast, are relatively realistic mental intrusions that usually take the form of thoughts, doubts, or concerns about contamination, mistakes, accidents, asymmetry, or disarray. Relative to AOs, ROs are more prone to be triggered by external cues, which correspond to specific core threats. Since the AO-RO model was proposed, research has demonstrated meaningful differences between the two subtypes of mental intrusions in several important domains relevant to OCD: 1) subsequent cognitive appraisals, inferences, and neutralization strategies;67 2) associated personality features;89 3) responsiveness to cognitive therapy;10 4) distinct neural abnormality.11
This evidence suggests that contents of mental intrusions, or at least the subtype of mental intrusions (i.e., AOs vs. ROs), should be considered when measuring mental intrusions. The Revised Obsessive Intrusion Inventory (ROII)2 is a well-developed measure that assesses an individual's mental intrusions in terms of content and frequency and has been used in many studies related to mental intrusions and obsessions. The ROII consists of two sections.2 In section I, respondents rate how frequently they experience each of 52 intrusive thoughts on a seven-point Likert scale. 52 items of the ROII assess mental intrusions with various contents (e.g., aggressive thoughts/images/impulses, sexual thoughts, contamination related thoughts, thoughts about accidents and mistakes, thoughts about dirt and cleaning). Section II consists of several items inquiring about mental-intrusion-related cognitive appraisals, emotions, and neutralization strategies. Lee and Kwon6 conducted factor analysis on a Korean version of the ROII section I and found that the two-factor structure (AOs and ROs) was appropriate for the scale. This two-factor structure was supported in another study as well.12
Although the ROII is a reliable and valid measure for assessing mental intrusions in terms of content and frequency, it still has several limitations. First, the ROII is composed of 52 items, which is relatively time-consuming to complete and could hinder its use both in research and clinical contexts. Second, it addresses various thought contents but certain contents are assessed in much greater proportion than others: 41 items assess AOs and 11 items assess ROs.2 Even among items tapping AOs, there is an imbalance of thought contents (i.e., only 10 items for sexual thoughts and 31 items for aggressive thoughts).2
Considering these limitations of the ROII, the aim of the current study was to develop a short version of the ROII assessing mental intrusions with a balanced proportion of thought contents. To this end, we examined the psychometric properties (factor structure, internal consistency, test-retest reliability, and external validity) of the short, 20-item Korean version of the ROII (ROII-20).
METHODS
Participants
The sample comprised 1125 undergraduate students (50.1% female) from two universities in Seoul. The students participated in this study in partial fulfillment of their research participation credit. Only native Korean speakers were retained for the study. The age of the participants ranged from 17 to 35 years (mean=21.86 years, SD=2.47).
Procedure
Groups of 50 to 100 individuals completed the ROII-20 and other measures in their university classes. The questionnaires were completed anonymously, and all participants provided informed consent. One subgroup of participants (n= 431) completed the ROII-20 for Exploratory Factor Analyses (EFA). Some participants in this subgroup (n=52) completed the ROII-20 twice (with an interval of four weeks) to establish test-retest reliability. A personal code instead of an identity was used to monitor these participants across sessions. A second subgroup of participants (n=464) completed the scale for Confirmatory Factor Analyses (CFA). A third subgroup of participants (n=230) completed the ROII-20 and other self-report measures to determine external validity of the ROII-20.
Instruments
The Revised Obsessive Intrusion Inventory-20
The ROII-20 is a 20-item scale that evaluates two different subtypes of mental intrusions labeled as AOs and ROs. All items are scored on a Likert scale from 0 ("never") to 6 ("frequently during the day"). The items of the ROII-20 were taken from the 52-item Korean version of the ROII.6 Lee and Kwon6 translated the original version of the ROII into Korean and conducted factor analysis on the Korean version of the ROII. To create the ROII-20, we considered two aspects of the Korean version of the ROII: the factor loading and the content. First, we adapted all items with contents related to mistakes and accidents of the scale (items 22, 23, and 24). Second, we adapted all items with contents related to dirt, ordering, and cleaning of the scale (items 50, 51, and 52). Third, we selected four items with contents related to fatal contamination of the scale (items 46, 47, 48, and 49). An item with this content category (item 45 'catching sexual transmitted disease') was removed from further analysis because it had an item-redundancy problem with item 48 ('fatal disease, stranger') and had the lowest factor loading (0.51). Fourth, we selected five items with aggressive contents of the scale that loaded most strongly on the AOs factor (items 12, 16, 21, 27, and 31). We expected that five items would constitute a minimum scale length that would still exhibit acceptable levels of internal consistency.13 Fifth, we also selected five items with sexual contents of the scale that loaded most strongly on the AOs factor (items 35, 36, 41, 42, and 43).
The Obsessive-Compulsive Inventory-Revised
The Obsessive-Compulsive Inventory-Revised (OCI-R) is a well-established 18-item questionnaire assessing the severity of OCD symptoms with good psychometric properties: internal consistency, test-retest reliability, and convergent validity.14 A Korean version of the OCI-R was administered, which has demonstrated good psychometric properties.15
Statistical analyses
To examine the factor structure of the ROII-20, we conducted EFA with maximum likelihood extraction and direct quartimin rotation. We also performed CFA with R (version 3.0.1, lavaan package)22 to cross-validate the results obtained from EFA. Goodness of fit was tested with Žć2, and two other indices were computed: the root mean square error of approximation (RMSEA) and the standardized root mean square residual (SRMR).23 An RMSEA of between 0 and 0.05 indicates a good fit, and a value between 0.05 and 0.08 indicates an acceptable fit. An SRMR of between 0 and 0.05 indicates a good fit, and a value between 0.05 and 0.10 indicates an acceptable fit.24 We also reported the comparative fit index (CFI).25 A CFI greater than 0.90 indicates an acceptable fit. The internal reliability of the ROII-20 was examined with the Cronbach ╬▒ coefficient. Two-tailed Pearson correlations were used to examine relations between the ROII-20 and the other self-report measures included in this study. Pearson correlations were also used to examine the test-retest reliability of the ROII-20. Pairwise treatment of missing data was used.
RESULTS
Factor structure and reliability of the ROII-20
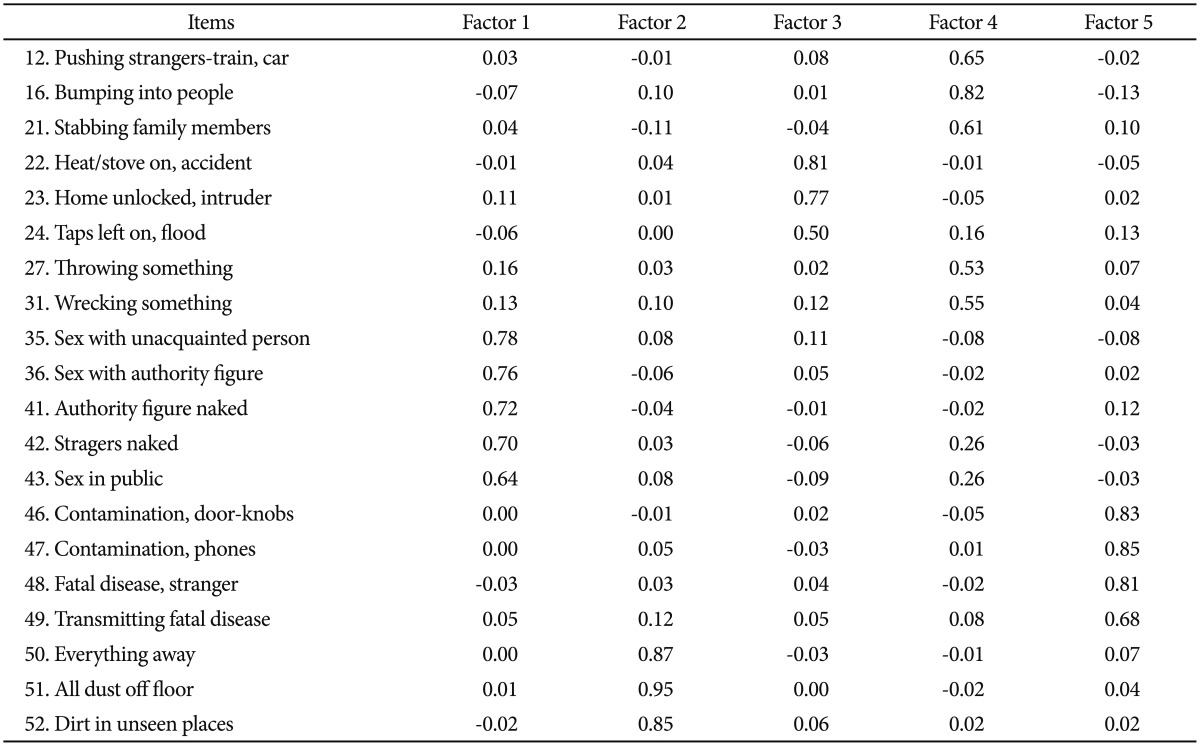
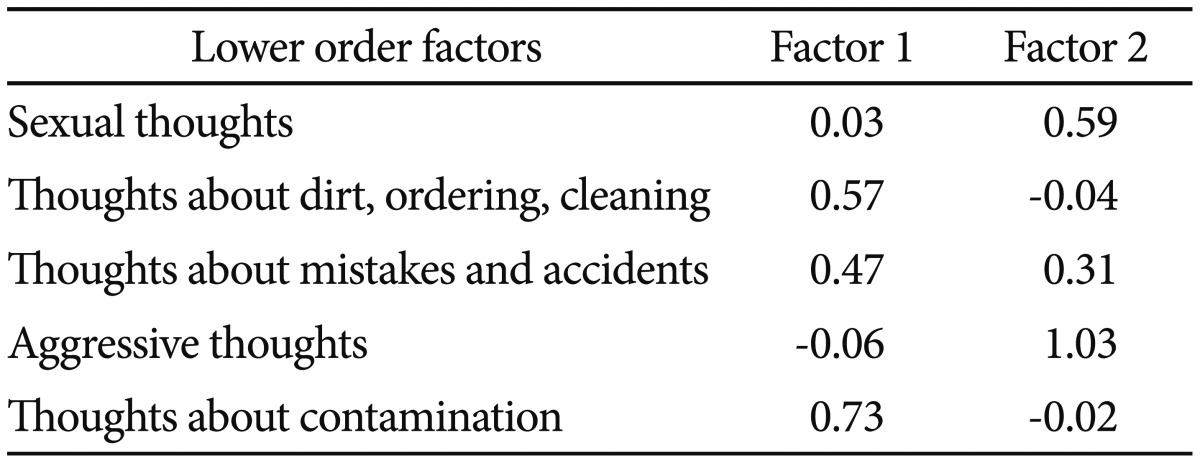
Of the 1125 participants, 51 had one item or more missing after completion of the questionnaires and were removed from the analyses. EFA was conducted with 410 participants. These participants were divided into two subgroups. The lower-order EFA was conducted with a subgroup (n=305) to examine the lower-order factor structure of the ROII-20. Eigenvalues of the correlation matrix suggested a five-factor structure (five eigenvalues >1.0). The five-factor model showed an acceptable fit (RMSEA=0.07) and explained 71.5% of the total variance. The detailed factor loadings are reported in Table 1. The five factors were consistent with the major thought contents that we aimed to assess using the scale: aggressive thoughts, sexual thoughts, thoughts about contamination, thoughts about mistakes/accidents, and thoughts about dirt/ordering/cleaning. We then conducted the higher-order EFA with another subgroup (n=105). In this step of analysis, we used factor scores of the five-factor model from the lower-order EFA to extract higher-order latent variables. Eigenvalues of the correlation matrix suggested a two-factor structure (2 eigenvalues >1.0). The two-factor model showed a good fit (RMSEA <0.01) and explained 69.4% of the total variance. Detailed factor loadings are reported in Table 2. The two factors were consistent with the two major subtypes of mental intrusions: AOs and ROs.
We conducted CFA with 434 participants to confirm the factor structure of the ROII-20. The hierarchical model that we obtained from the EFA was tested by maximum likelihood estimation. The results showed that the hierarchical model had an acceptable fit [Žć2 (164)=488.43, p<0.001; RMSEA=0.07; SRMR=0.05; CFI=0.93]. This model is depicted in Figure 1.
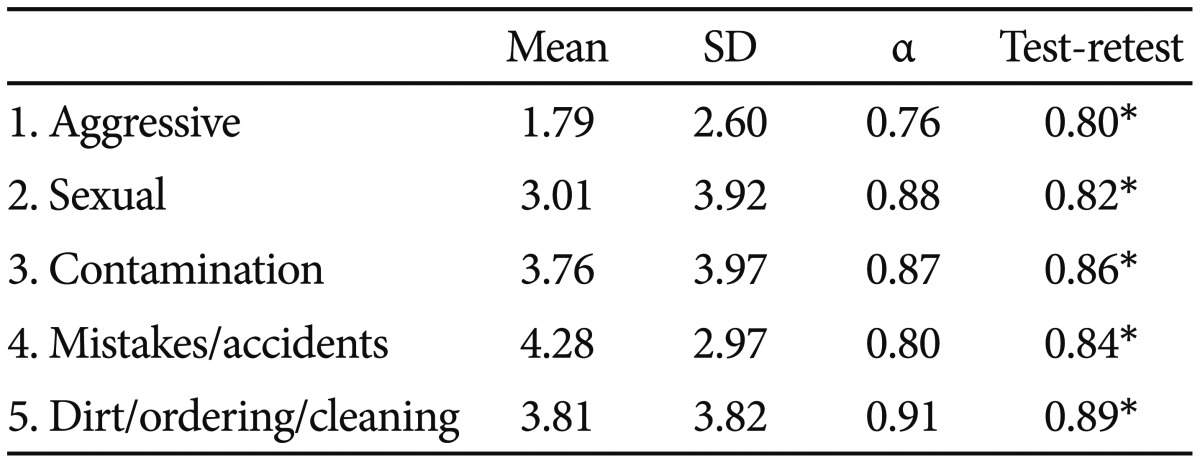
Mean, SDs, internal consistency coefficient (Cronbach ╬▒), and test-retest reliability indices for the components of the ROII-20 are reported in Table 3. The Cronbach ╬▒ ranged from 0.76 to 0.91, suggesting good internal consistency for the subscales. The Cronbach ╬▒ of the higher-order subscales (0.88 for the AOs subscale and 0.80 for the ROs subscale) also suggested good internal consistency. Finally, among participants who completed the ROII-20 twice, correlations between the two administrations ranged from 0.80 to 0.89, which suggested good test-retest reliability.
Correlations between the ROII-20 and other measures
Table 4 reports the correlations between the components of the ROII-20 with the other questionnaires measuring OCD symptoms, anxiety, and depression. First, the OCI-R total score was positively associated with the scores of all five lower-order subscales and two-higher order subscales (AOs and ROs) of the ROII-20. However, the ROs score was more strongly associated with the OCI-R total score than the AOs score was (Z=4.49, p<0.01). Three subscales of the ROs scale were also strongly associated with most of the subscales of the OCI-R. However, the relationships between the two subscales of the AOs scale (i.e., aggressive thoughts and sexual thoughts) and the subscales of the OCI-R were mostly weak or not significant. Second, the PIWUSR-obsessional impulses subscale was strongly associated with the AOs scale and its two subscales, whereas the relationships between the PIWSUR-obsessional impulses scale and the three subscales of the ROs scale were very weak or not significant. Third, both of the AOs and ROs scales were moderately associated with the BAI. However, the correlation between the AOs scale and the PIWSUR-obsessional impulses subscale was greater than the correlation between the AOs scale and the BAI (Z=4.68, p<0.01), and the relationship between the ROs scale and the OCI-R was stronger than the relationship between the ROs scale and the BAI (Z=4.47, p<0.01). Finally, the relationships between the AOs/ROs scales and the CES-D were significant but weak. The AOs scale was more strongly associated with the PIWSUR-obsessional impulses subscale than with the CES-D (Z=5.47, p<0.01) and the ROs scale's correlation with the OCI-R was significantly higher than its correlation with the CES-D (Z= 6.28, p<0.01).
DISCUSSION
The present study examined the psychometric properties of a short version of the Korean adaptation of the ROII developed by Purdon and Clark.2 EFAs revealed that a hierarchical model fit the data. The hierarchical model consisted of five lower-order factors (i.e., aggressive thoughts, sexual thoughts, thoughts about contamination, thoughts about mistakes/accidents, and thoughts about dirt/ordering/cleaning) and two higher-order factors (i.e., AOs and ROs). CFA also confirmed that this hierarchical model is appropriate for application to the data obtained. Internal consistency and test-retest reliability of the scale ranged from good to very good. Specific links to psychiatric symptoms were identified. More precisely, the two subtypes of mental intrusions (autogenous and reactive) were related to the OCI-R. However, the associations between ROs and the OCI-R were stronger than the associations between AOs and the OCI-R. One possible explanation for these differential relationships is that the OCI-R primarily consists of overt OCD symptoms such as washing, ordering, checking, or hoarding. These overt OCD symptoms have been considered to be more closely related to ROs than AOs.6 The PIWSUR-obsessional impulses subscale was related to AOs exclusively. This result indicates that the AOs subscale of the ROII-20 exhibits good convergent validity because the PIWSUR-obsessional impulses subscale primarily concerns obsessions about harming oneself or others and obsessions related to sexual behaviors.16 Finally, moderate relationships between AOs/ROs and anxiety and relatively weak relationships between AOs/ROs and depression were found, as demonstrated in previous studies.8 However, the AOs subscale of the ROII-20 was more strongly associated with the PIWSUR-obsessional impulses subscale than with the BAI and the CES-D. The relationship between the ROs subscale and the OCI-R was stronger than the relationship between the ROs subscale and the measures assessing depression and anxiety. Overall, the current study demonstrated that the ROII-20 possesses good psychometric properties.
The completion time of the original 52-item scale is approximately 13 min (15 seconds per item), whereas the ROII-20 takes only 5 min to complete. This significant time saving is only justified if the psychometric properties of the short-form measure remain largely comparable to those of the original measure.26 We found the ROII-20 to have a theoretically based factorial structure.6 Moreover, the internal consistency coefficients of the ROII-20 are similar to those obtained with the original scale devised by Lee and Kwon6 (the Cronbach ╬▒ of the AOs and ROs were 0.95 and 0.89 for the original scale and 0.88 and 0.85 for the short-form scale, respectively). Taken together, these results support the use of the ROII-20 for meaningful time saving.
We developed the ROII-20 by retaining the 10 items that loaded most strongly on each of the two factors (AOs and ROs). Although this technique has been frequently used to develop short-form measures, it has the limitation that selected items reflect narrower constructs.26 This potential problem is herein discussed with respect to one of the components of the ROII-20: aggressive thoughts. The original ROII contains 31 items tapping various types of aggressive thoughts: aggressive thoughts while driving, thoughts about hurting others, thoughts about hurting family, thoughts about causing a public scene, and thoughts about impulsive damage.2 We selected five of these items, which could diminish the breadth of the original measure and omit certain aspects of the construct (i.e., aggressive thoughts). The ROII-20 items with aggressive contents, however, represent all of the major aggressive contents of the original ROII (i.e., two items from 'hurting others', one item from 'hurting family', one item from 'causing a public scene', and one item from 'impulsive damage'), except for only one category (aggressive thoughts while driving).
In the present study, we examined the external validity of the ROII-20 using several measures tapping OCD symptoms and general distress (i.e., depression and anxiety), and we were able to determine the scale's convergent validity and criterion validity. Moreover, we examined the differential relationships between the AOs/ROs subscales and two measures tapping OCD symptoms to determine the subscales' discriminant validity. The discriminant validity of the whole scale, however, has yet to be established. Because mental intrusions are similar to other unwanted cognitions (e.g., worry)27 and still different from those cognitions, it would be valuable to examine the discriminant validity of the ROII-20 using well-validated measures assessing such cognitions.