The Core Symptoms of Adolescents Online and Offline Gambling in South Korea Using Network Analysis
Article information

Abstract
Objective
Adolescent gambling is rapidly increasing recently. However, little is known about the core feature of adolescent gambling that should be the treatment target for adolescents. Thus, the objective of this study was to determine the core symptom of adolescent gambling using network analysis with large-scale data targeting community indwelling adolescents.
Methods
We used dataset of the 2018 national survey on youth gambling problems collected by the Korea Center on Gambling Problems to explore symptom networks of gambling in adolescents. Of 17,520 respondents in the dataset of the 2018 national survey on youth gambling problems collected by the Korea Center on Gambling Problems, 5,619 adolescents with experience of gambling were included in the analysis. We computed an association network, a graphical least absolute shrinkage and selection operator, and a directed acyclic graph to model symptom interactions.
Results
In each network of online, offline, and all gambling, stealing money or other valuable things in order to gamble or pay off gambling debts was the most centrally situated and skipping practice followed by dropping out of activities. Especially strong connections emerged between stealing money or other valuable things in order to gamble or pay off gambling debts and academic performance degradation due to gambling. Feeling bad due to gamble and skipping hanging out with friends who do not gamble emerged as a highly central node that might be distinctive to adolescents with online gambling.
Conclusion
These findings demonstrate central features of adolescent gambling. Different associations among specific network nodes suggest the existence of distinctive psychopathological constructs between online and offline gambling.
INTRODUCTION
Gambling has traditionally been regarded only as an adult activity. However, recent studies have provided evidence that substantial numbers of adolescents also participate in gambling [1,2]. Adolescent gambling is gradually emerging as a serious health problem that requires more rigorous research attention [3,4]. In addition, there are recent reports showing that gambling involvement is increasing as spatial distancing continues under the influence of the coronavirus disease-2019 pandemic [5,6].
Recently gambling environments have changed dramatically [7]. Accessibility of online gambling has increased due to the development of technology and the universalization of digital mobile personal devices [8]. Easy accessibility, rapid feedback, and easy repetitive betting have raised concerns about excessive gambling [9]. The increased accessibility allowed frequent and repeated bets without limits of time and place, which caused concern about excessive gambling [10]. Previous studies reported features distinct between online gambling and land-based gambling, such as higher gambling problem severity, higher addiction potential, younger age, and severe psychological distress, but some studies demonstrated contradictory results [10-12]. Therefore, additional research is needed to resolve this controversy.
Determining treatment targets for adolescent problematic gambling is important to establish appropriate early therapeutic intervention strategy and prevent chronification in adulthood. However, adolescents gamblers are a heterogeneous group that cannot be explained by a single etiology and their symptom presentations are also diverse [13]. In addition, gambling is a hidden addiction, and since gambling adolescents do not seek treatment until overt behavioral problems (e.g., stealing, skipping school) appear [14]. Although there are several previous studies on adolescent gambling, such studies have been conducted mainly on patient populations who seek psychiatric treatment, which might cause a bias to understand true core features of adolescent gambling [15-17]. Thus, a large community-based study is needed to understand psychological characteristics of adolescent gambling and to establish for adolescent gambling.
Network approaches are useful for clarifying the therapeutic target of psychiatric problems that include heterogeneous conditions. Network approaches are analytical methods that can identify nodes (symptoms) and edges (connections or associations between nodes). They are newly attracting attention in psychiatry and various social science studies [18,19]. In particular, network analysis in psychiatry can reveal core symptoms and the most related symptoms among the diagnostic criteria of Diagnostic and Statistical Manual of Mental Disorders, 5th edition so that the latent structure of a disease and the interconnection between symptoms can be identified [20].
Therefore, the objective of this study was to determine core symptoms of adolescent gambling using network analysis with large-scale data targeting community indwelling adolescents.
METHODS
Study population
Data of the 2018 national survey on youth gambling problem collected by the Korea Center on Gambling Problems were used. This survey was conducted on in-school youth and out-of-school youth. As of August 2018, in-school youth included students from the first grade of middle school to the second grade of high school. Based on the April 2017 Educational Statistic Service, 1,381,334 middle school students and 1,101,624 high school students were set as the population, and the total target sample size of in-school youth was 14,000 subjects (7,800 middle school students, 6,200 high school students) considering the population ratio. For youth in schools, the sample size by region was determined using the proportional distribution method. Post-stratification and weighting were applied to adjust the gender distribution. For in-school youth, 133 middle schools nationwide and 126 high schools nationwide were selected to obtain target samples. After consent was obtained through prior contact with the school selected as the sample, trained interviewers visited the school and conducted survey. All students participated in the survey voluntarily, and written informed consent was obtained from the participants. A total of 17,520 in-school youths were recruited.
Out-of-school youths were collected by non-probability sampling because there was no population data and sampling frame. Out-of-school youths were defined as those who used out-of-school youth support centers and youth shelters or belonged to non-accredited alternative schools during the survey period. In the case of out-of-school youths, data were collected from a total of 1,240 subjects.
Among the collected data, 5,619 adolescents with experience of gambling were included in the analysis. A total of 5,619 gambling adolescents were asked to choose only one money betting game they played most frequently over the past three months. According to their responses, they were assigned into an online gambling group or an offline gambling group. The protocol of this study was approved by the Institutional Review Board (IRB) of National Center for Mental Health (IRB no.116271-2021-33).
Gambling Problem Severity Scale
To evaluate the degree of gambling of adolescents, Gambling Problem Severity Scale (GPSS), a subscale of the Canadian Adolescent Gambling Inventory [21], was used. The GPSS consists of nine items: G1, skipping practice or dropping out of activities; G2, skipping hanging out with friends who do not gamble; G3, planning gambling/betting activities; G4, feeling bad; G5, going back another day to try to win; G6, hiding gambling/bets from others; G7, feeling that gambling/betting is a problem; G8, taking money from lunch/clothing allowance, and so on; and G9, stealing money in order to gamble/bet. Each item of GPSS is rated with a 4-point Likert scale (0, no; 1, sometimes; 2, often; and 3, almost always), yielding a total score ranging from 0 to 27. Scores of gambling severity were classified into three categories: 1) 0–1, no problem gambling; 2) 2–5, low to moderate severity; and 3) 6 or more, high severity. Cronbach’s α for the GPSS of sampled participants was 0.768, which was considered reliable.
Statistical analyses
Network structures of a total of 10 items (9 items of GPSS and the presence of academic performance degradation due to gamble) in adolescents with gambling experience were estimated using R-package qgraph [22]. Networks consisted of both nodes (symptoms) and edges (associations among symptoms). Edges connecting each node represent regularized partial correlation coefficient between nodes after controlling for all other variables in the network. Consequently, if partial correlation was exactly zero, then no edge was drawn between two nodes, indicating that two variables were independent after controlling for all other variables in the network [23]. To avoid false-positive edges, least absolute shrinkage and selection operator was used to shrink small edges to exactly zero and create a more parsimonious network [24]. Minimizing the extended bayesian information criteria was used to avoid false-positive edges and retrieve true network structures accurately [25]. All gambling related factors were ordered-categorical variables. Network analyses were based on polychoric correlations.
The central stability (CS) coefficient was estimated to examine robustness using the R-package bootnet. The CS coefficient for the centrality measures should not be below 0.25. It is preferably above 0.5 [23]. To investigate whether nodes were clustered together, the modularity-based community-detecting algorithm was implemented. The spin-glass algorithm was used to test for communities in the network whereby the number and weighted strength of edges within a cluster exceeded the number and weighted strength of edges between nodes in another cluster. The spin-glass community function of the R-package, igrah, was applied over the glasso network (weights=null, vertex=null, parupdate=false, gamma=0.5, start temperature=1, stop temperature=0.01, cooling factor=0.99, spins=17) [26].
Each symptom’s centrality was estimated. Node strength centrality indicated the sum of all correlations of each edge linked to the node. Closeness centrality indicated the inverse of the sum of all shortest paths between a given node and all other nodes in the estimated network. The betweenness centrality was based on the number of times the node lied on the shortest path between two other nodes. It could be interpreted as how central the node was connecting other nodes. Thus, as node strength centrality was substantially correlated with closeness or betweenness centrality, most central symptoms within the network structures of gambling related factors were estimated according to node strength, closeness centrality, and betweenness centralities.
After estimating the network, the centrality outcome “strength” was plotted for every variable in the network. To graphically visualize the network structure, the Fruchterman–Reingold algorithm was used. It placed nodes with stronger connections closer together, whereas nodes with weaker connections were placed more peripherally in the network [22,27].
RESULTS
Participants characteristics
A total of 5,619 adolescents with experience of gambling completed the questionnaire. The mean age of these participants was 15.44 (standard deviation [SD]=1.56) years. More than half of participants were males (n=858, 61.0%). Table 1 presents the mean symptom severity score for each GPSS item. The total GPSS score of the online gambling group was 3.88 (SD=4.31), whereas that of the offline group was 1.05 (SD=2.18), showing a significant difference between the two groups (p<0.001).

Mean symptoms severity scores of problematic gambling adolescents
Network analysis of all adolescents with gambling experience
As shown in Figure 1, psychological network consisting of 10 gambling related factors were constructed for 5,619 adolescents with gambling experience. Of a total of 45 possible edges, 32 were estimated to be above zero. Node strength and betweenness centralities demonstrated an interpretable level of stability (i.e., CS-coefficient=0.517; CS-coefficient=0.361), although closeness centrality demonstrated low levels of stability (i.e., CS-coefficient=0.206).
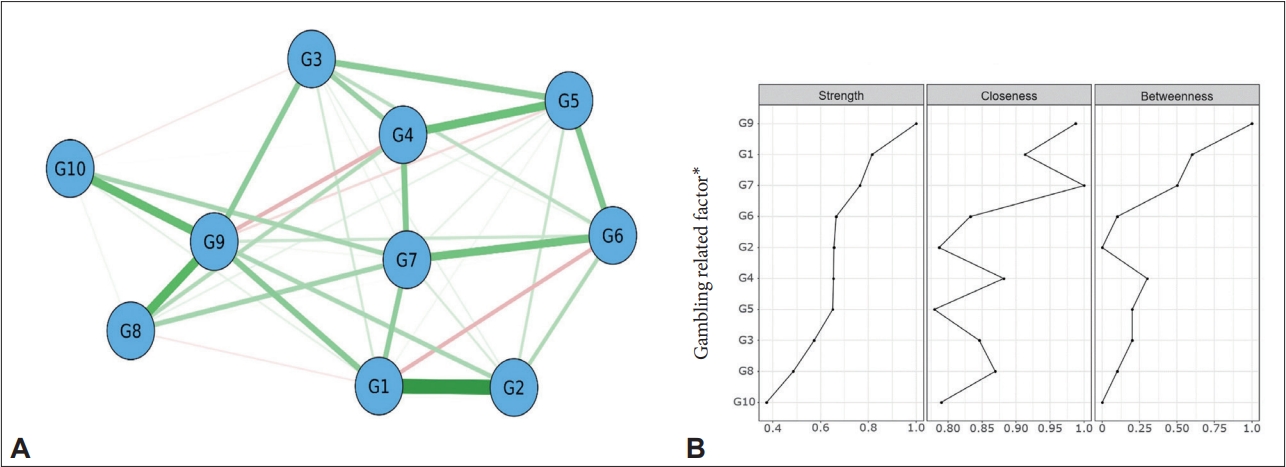
Network analysis of all adolescents with gambling experience. A: Network containing the 10 gambling related factor. Green lines represent positive associations, red lines negative ones, and the thickness and brightness of an edge indicate the association strength. B: Node strength, closeness, and betweenness centrality estimates for the 10 gambling related factors. *gambling related factor: G1, skipping practice or dropping out of activities; G2, skipping hanging out with friends who do not gamble; G3, planning gambling/betting activities; G4, feeling bad; G5, going back another day to try to win; G6, hiding gambling/bets from others; G7, feeling that gambling/betting is a problem; G8, taking money from lunch/clothing allowance, and so on; G9, stealing money in order to gamble/bet; G10, academic performance degradation.
In the network, G1 and G2 appeared to have the strongest connection, followed by the connection between G8 and G9, and the connection between G9 and academic performance degradation due to gambling (G10).
A community-detection analysis estimated that the 10 gambling related factors could be organized into three clinically meaningful clusters. Cluster A (limited other activities due to gambling) included G1 and G2. Cluster B (non-specified gambling symptoms) included G3, G4, G5, G6, and G7. Cluster C (problematic behavior due to gambling) included G8, G9, and G10.
G9 showed the strongest centrality (betweenness=1; closeness=0.99; strength=1), followed by G1 (betweenness=0.6; closeness=0.91; strength=0.82), G7 (betweenness=0.5; closeness=1; strength=0.77), and G6 (closeness=0.83; strength=0.67). These symptoms were situated in the central to the symptom network of gambling adolescents (Figure 1). G10 due to gambling was the most poorly interconnected one in the network (closeness=0.79; strength=0.37).
Network analysis of adolescents with online gambling experience
We additionally conducted analyses for those with online and offline gambling experience separately. As shown in Figure 2, psychological network consisting of the 10 gambling related factors were constructed for 524 adolescents with online gambling experience. Of a total of 45 possible edges, 34 were estimated to be above zero. Node strength centrality demonstrated an interpretable level of stability (i.e., CS-coefficient=0.315), although betweenness and closeness centralities demonstrated low levels of stability (i.e., CS-coefficient=0.183; CS-coefficient=0.116).
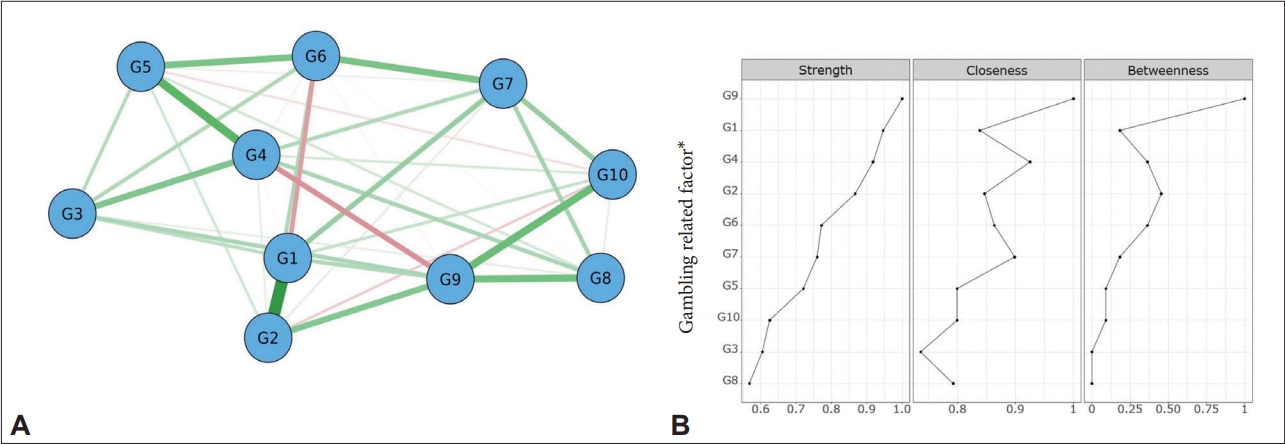
Network analysis of adolescents with online gambling experience. A: Network containing the 10 gambling related factor. Green lines represent positive associations, red lines negative ones, and the thickness and brightness of an edge indicate the association strength. B: Node strength, closeness, and betweenness centrality estimates for the 10 gambling related factors. *gambling related factor: G1, skipping practice or dropping out of activities; G2, skipping hanging out with friends who do not gamble; G3, planning gambling/betting activities; G4, feeling bad; G5, going back another day to try to win; G6, hiding gambling/bets from others; G7, feeling that gambling/betting is a problem; G8, taking money from lunch/clothing allowance, and so on; G9, stealing money in order to gamble/bet; G10, academic performance degradation.
Regarding centrality index, G9 showed the strongest centrality (betweenness=1; closeness=1; strength=1), followed by G1 (betweenness=0.18; closeness=0.84; strength=0.95), showing the same result as any gambling model (Figure 2). G4 (betweenness=0.36; closeness=0.93; strength=0.93) and G2 (closeness=0.85; strength=0.87) also showed strong centrality. Their results were differentiated from any gambling model. G8 was the most poorly interconnected one in the network (closeness=0.79; strength= 0.57).
The connection between G1 and G2 was the strongest in the network. The second strongest connection was between G4 and G5, which was a distinguishing feature that only appeared in the online gambling model. The connection between G9 and G10 showed the third strongest connection, consistent with adolescents’ all gambling model.
A community-detection analysis revealed that the 10 gambling related factors could be organized into two clinically meaningful clusters. Cluster A (problematic behavior due to gambling) included G1, G2, G7, G8, G9, and G10. Cluster B (non-specified gambling symptoms) included G3, G4, G5, and G6.
Network analysis of adolescent with offline gambling experience
As shown in Figure 3, a psychological network consisting of the 10 gambling related factors was constructed for 5,095 adolescents with offline gambling experience. Of a total of 45 possible edges, 27 were estimated to be above zero. Node strength, closeness, and betweeness centralities demonstrated an interpretable level of stability (i.e., CS-coefficient=0.314; CS-coefficient=0.314; CS-coefficient=0.38).
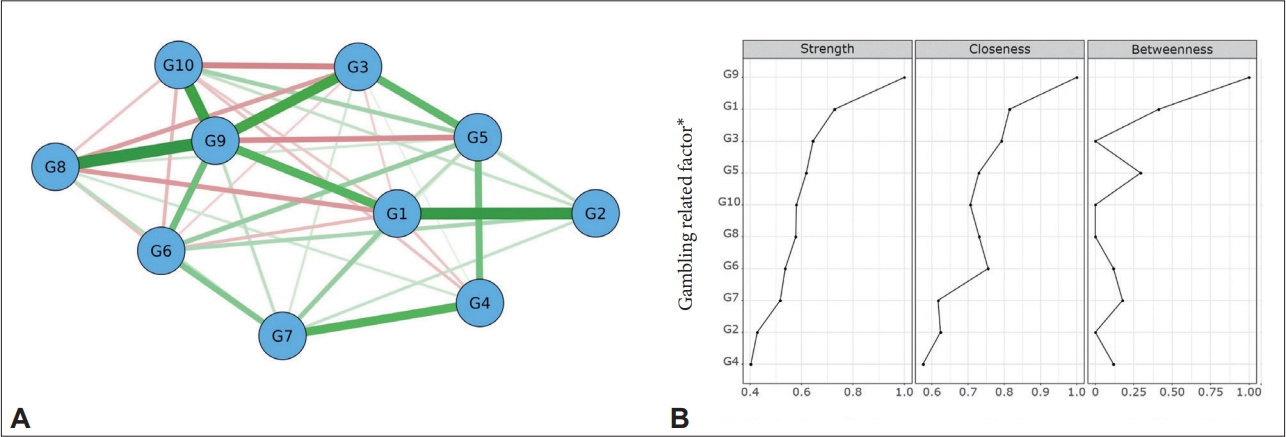
Network analysis of adolescents with offline gambling experience. A: Network containing the 10 gambling related factor. Green lines represent positive associations, red lines negative ones, and the thickness and brightness of an edge indicate the association strength. B: Node strength, closeness, and betweenness centrality estimates for the 10 gambling related factors. *gambling related factor: G1, skipping practice or dropping out of activities; G2, skipping hanging out with friends who do not gamble; G3, planning gambling/betting activities; G4, feeling bad; G5, going back another day to try to win; G6, hiding gambling/bets from others; G7, feeling that gambling/betting is a problem; G8, taking money from lunch/clothing allowance, and so on; G9, stealing money in order to gamble/bet; G10, academic performance degradation.
G9 showed the strongest centrality (betweenness=1; closeness=1; strength=1), followed by G1 (betweenness=0.41; closeness=0.82; strength=0.73), consistent with the previous two models. G3 (betweenness=0; closeness 0.79; strength=0.64) and G5 (closeness=0.73; strength=0.62) showed the third and fourth strongest centrality, respectively. These were characteristic features that could distinguish them from the other two previous models (Figure 3). G4 was the most poorly interconnected one in the network (closeness=0.58; strength=0.40).
In the network, G8 and G9, which showed the second strongest connection in the any gambling model, had the strongest connection. G1 and G2, which appeared as the strongest connection in previous two models, also showed the second strongest connection. G9 and G10 showed the third strongest connection, consistent with results of the previous two models.
A community-detection analysis revealed that the 10 gambling related factors could be organized into three clinically meaningful clusters. Cluster A (limited other activities due to gambling) included G1 and G2. Cluster B (non-specified gambling symptoms) included G3, G4, G5, G6, and G7. Cluster C (problematic behavior due to gambling) included G8, G9, and G10, consistent with results of the any gambling model.
DISCUSSION
To the best of our knowledge, this is the first study to identify the latent structure among psychological variables using a network analysis in large community adolescents with gambling experience. Previous researches to date were focused on the association of gambling behavior with psychosocial variables [4,28]. To date, previous studies using network analysis have mostly been used to figure out the complex features of each symptom in depression, schizophrenia, eating disorder, and posttraumatic stress disorder [29-32].
The present study found that stealing money or other valuable things in order to gamble played a key role in all three models, suggesting that stealing was a core feature of the problematic gambling. Stealing money was an item with the most delinquent behavior among GPSS items. It was clearly distinguished from other gambling related harmful problems (guilty feeling, skipping activities, etc.). Previous studies have reported high risks of violent delinquent behaviors (such as fighting and carrying a weapon) and non-violent behaviors (such as theft and selling drugs) of adolescent gamblers [33,34]. Findings of previous studies have revealed that impulsivity, low parental supervision, and deviant friends are predictors of gambling and delinquent behavior, respectively [35,36]. Our finding of this study indicates that stealing behavior in online and offline gambling is the most closely and strongly related factor with other gambling related symptoms in adolescents, and this result suggests the clinical importance of examining gambling related stealing behavior when screening and evaluating pathological gambling. Further assessment of impulsivity and other types of delinquent behavior in pathological gambling adolescents would be needed in the future.
In all three models, there was a strong interconnection between stealing money or other valuable things in order to gamble and academic performance degradation due to gamble. Although it was not a central symptom in the network, it was found to be the most relevant factor to the most central factor, stealing money or other valuable things in order to gamble. Gambling participation and preoccupation can lead to academic underachievement [37]. Our findings reconfirm that underlying impulsivity causes early school dropout in gambling adolescents, while newly suggesting that the decline in academic performance due to gambling needs to be considered in the impulsivity dimension such as stealing behavior [37-39].
Differences in social involvement were observed in associations with problematic gambling across adolescent online and offline gamblers. Skipping practice or dropping out of activities showed the second strongest centrality, and a strong connection with skipping hanging out with friends who do not gamble in all three models. Unlike the all, offline gambling model, the only online model showed that skipping hanging out with friends was centrally situated. Online gambling is typically a solitary play that leads to social withdrawal, whereas offline gamblers often start or continue gambling for social reasons due to peer pressure [33,40]. On the other hand, social isolation and peer victimization as predictors of online gambling have been consistently reported [41]. Considering results of a previous study showing negative consequences of gambling on social functioning [42], it is difficult to conclude that online gambling will lead to a particularly more severe deterioration in social functioning than offline gambling. Therefore, a further longitudinal study to confirm the causal relationship between gambling and social function is needed.
One of centrally situated symptoms of the online gambling network model was feeling bad due to gambling. However, in the offline gambling model, it was the most peripherally situated. These differences could be interpreted in two ways. First, in general, online gambling is more addictive than offline gambling because of its less cost, convenience, speed, anonymity, various contents, and attractive marketing [43-45]. In line with previous studies showing that online gamblers have greater gambling severity and associated risky behavior than offline gamblers [46,47], this study also showed that the severity of the online gambler group was higher than that of the offline group. Therefore, in the offline gambler group, dependence symptoms for gambling such as “feeling bad due to gamble” would have appeared less than in the online gambler group. Second, in previous studies of online game addiction similar to online gambling, depression is the most common comorbid disorder [48-50]. In online gambling adolescent accompanied by depression, guilty feelings about gambling and awareness of loosening control gambling may appear as significant gambling related negative emotions. To confirm the comorbidity of adolescent gambling, further study is needed.
Some limitations of the current study must be acknowledged. First, our study had a cross sectional design. Thus, could not confirm the causal relationship between factors. Second, although subjects of this study were divided into online gamblers and offline gamblers, it was difficult to generalize easily and apply to gambling adolescents because there were various cases of mixed gamblers or offline gamblers in the past but now online gamblers in actual situations. Third, since this study was based on self-report, the accuracy of responses of participants might not be ensured. Adolescents are often late in help seeking due to the lack of awareness of gambling related problems [51]. Thus, the gambling severity in this study might have been underestimated. Fourth, in this study, analysis results according to gambling problem severity were not presented. In network analysis according to gambling severity, the CS coefficient was evaluated at an unacceptable level, and the model was not accepted. Finally, in our analysis method, demographic variables (age, gender, residential area) that can affect gambling were not considered, so sample heterogeneity may have affected the analysis result.
In conclusion, the most central symptom in gambling was stealing money, suggesting the importance of accompanying delinquent behavior for evaluation and therapeutic intervention of a gambling adolescent. In addition, the distinct nature of connectivity between online and offline gambling models provides important information for understanding the psychopathology of complex adolescent gambling.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Yunhye Oh, Ji Hyun Baek. Data curation: Yunhye Oh. Formal analysis: Yunhye Oh. Funding acquisition: Ji Hyun Baek. Investigation: Yunhye Oh, Ji Hyun Baek. Methodology: Yunhye Oh, Ji Hyun Baek. Project administration: Ji Hyun Baek. Supervision: Yoo-Sook Joung, Ji Hyun Baek. Writing—original draft: Yunhye Oh. Writing—review & editing: Yoo-Sook Joung, Ji Hyun Baek.
Funding Statement
This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project Number NTIS 9991006915, KMDF_PR_20200901_0250).