Does Drinking Culture Induce Problematic Alcohol Use? Evidence From a Military Representative Survey in Korea
Article information

Abstract
Objective
To examine the relationship between problematic alcohol use and contributing factors among Korean professional soldiers.
Methods
Cross-sectional data of 2,646 participants collected by 2014 military-wide representative health survey was analyzed. Multivariate logistic models were used to identify contributing factors for problematic alcohol use. Problematic alcohol use was defined by the Alcohol Use Disorders Identification Test (AUDIT) questionnaire as hazardous (8≤ AUDIT <16) or harmful (AUDIT ≥16). Tolerant drinking culture was measured by the Drinking Culture Questionnaire.
Results
Hazardous alcohol use was found in 56.9% of men and 46.8% of women and harmful use in a further 16.2% of men and 5.4% of women. In univariate analyses, perceived health status, subjective sleep quality, depression, and drinking culture were related to the outcome variable. In multivariate models controlling covariates, the likelihood of problematic alcohol use was significantly increased by man gender, being single, current/past smoking, and tolerant/permissive drinking culture. In those with harmful alcohol consumption, tolerant drinking culture was a particularly powerful influence.
Conclusion
A substantial proportion of Korean professional soldiers demonstrated problematic alcohol use. Tolerant drinking culture was shown to have a significant influence on problematic alcohol use in the military. Our findings underscore the need for public health policies that address this drinking culture to mitigate negative health consequences and preserve the forces’ combat readiness.
INTRODUCTION
Alcohol is one of three leading contributing factors to the global burden of disease, which negatively affects not only physical and mental health but also a nation’s economy [1-4]. Harmful alcohol use was estimated to have caused 5.3% of all deaths and 7.2% of all premature deaths worldwide in 2016 [5]. In numerous studies, military populations have been found to have higher alcohol misuse, binge drinking, and other alcohol-related problems [6-11]. A study from the United Kingdom (UK) revealed that the most common mental disorder in the military was alcohol abuse, with a prevalence of 18.0% [12]. A large representative and cross-sectional survey conducted with United States (US) active military personnel demonstrated that 21.9% of active-duty male soldiers are heavy alcohol users [9]. Prior research identified that deployment, exposure to combat, and post-traumatic stress disorder (PTSD) increase the likelihood of harmful alcohol use [8].
Alcohol use problems in the military seem to be highly related to the occupation, despite the ‘healthy soldier effect’ that implies better health status of soldiers than the general population [13,14]. Moreover, alcohol use problems affect individuals’ mental and physical health even after retirement. Multiple studies have demonstrated that veterans significantly suffer from substance addiction, including alcohol abuse [11,15-17]. Given the significance of roles of military personnel in society, the increased risk of alcohol use problems should not be neglected. In addition, safety concerns arise as military personnel are authorized to access weapons. Previous studies have demonstrated that alcohol problems increase the risk of violent crimes and misconduct in the military [18,19].
The prevalence of alcohol use disorder (AUD) in the military population is higher than that of the general population [20]. However, no single study has ever assessed alcohol use problems in the Korean military [21], and the underlying mechanisms that contribute to problematic alcohol use in this population have not been explored. Korea’s alcohol consumption per capita in 2019 was 8.7 liters, comparable to the average of 8.9 liters in the Organisation for Economic Co-operation and Development [22]. This study aimed to investigate whether the Korean military servicemen are also at greater risk of AUD than the general population, which was repeatedly demonstrated in the Western countries.
Uniformed services are more homogenous than the civil sector by the nature of their duty and structure. In addition to manliness or toughness, obedience and taking unilateral action are often emphasized as virtues in the military. Thus, there is a need to understand how these cultural components and the culture of drinking contribute to problematic alcohol use in the military population.
We therefore proposed three hypotheses: 1) Korean professional soldiers have a high rate of problematic alcohol use, 2) individual factors such as man gender and single status and work and life stress contribute to problematic alcohol use, and 3) a tolerant drinking culture contributes to problematic alcohol use in this population. In order to test these hypotheses, we analyzed military representative survey data from 2014 with multivariate logistic regression models.
METHODS
Data source
This study used data from the Military Health Survey (MHS), carried out by the Armed Forces Medical School (AFMS), to demonstrate representative health data of the Korean Armed Forces (KAF) for evidence-based health policy development and implementation. A pilot study was conducted in 2013 and the first wave was carried out in 2014. The overall process of the survey is described as follows: Before the survey was carried out, the AFMS provided training to interviewers to assist interviewees. The survey was carried out in 40 randomly-selected military units across all branches (Army, Navy, Marine, and Air Force) in consideration of the location, unit type (front or rear), and unit population. Although the study included enlisted and professional soldiers as study participants, the Alcohol Use Disorders Identification Test (AUDIT) was applied only to professional soldiers, as enlisted soldiers are not allowed access to alcohol during their service period. A total of 3,546 professional soldiers participated in the survey with informed consent. After excluding 900 subjects with incomplete information, 2,646 subjects remained for analysis (Figure 1).
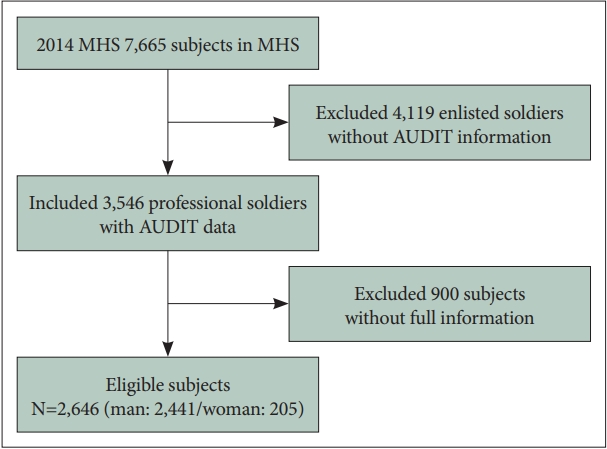
Flowchart describing the study population. MHS, Military Health Survey; AUDIT, Alcohol Use Disorders Identification Test.
Measures
In identifying the relationship between problematic alcohol use and factors of interest, we included the following variables to control for confounding effects: 1) gender (man/woman), 2) age (18–25/26–30/31–40/41–50/65 years or less), 3) marital status (single/married/divorced/separated), 4) educational level (secondary school or less/university or more/graduate school), 5) military rank (commissioned/non-commissioned officer), 6) service years (0–2.9/3–9.9/10–19.9/20 years or more), 7) location of unit (urban/rural/very remote area), 8) working hours (less than 40 hours per week/40–49.9/50–59.9/60 hours or more), 9) working condition (normal work/shift work or night work), 10) work-related stress (high/low), 11) life stress other than work (high/low), 12) subjective health status (good/bad), 13) average sleep duration per day (5–9 hours a day/less than 5 hours/more than 9 hours), 14) satisfaction with sleep quality (satisfied/not satisfied), 15) body mass index (BMI) (less than 18.5/18.5–25/25 kg/m2 or more), and 16) smoking history (non-smoker/current smoker/past smoker).
Center for Epidemiologic Studies Depression short form
The survey included Center for Epidemiologic Studies Depression short form CES-D 11 which is a shortened version of the full 20-item CES-D. The full-scale survey has been widely used as a screening instrument for depression in large scale studies since 1977 [23,24]. It asks about depressive symptoms in the past week and each item is rated on a 0–3 scale (0: rarely, 1: some or little, 2: occasionally, 3: most). We converted the scores from CES-D 11 to the full 20-item scores by multiplying 20/11 and used the previously suggested score of 16 points as the cutoff for depression [25].
Alcohol Use Disorders Identification Test
The survey measured the severity of alcohol use problems with AUDIT, a 10-item questionnaire developed by the World Health Organization (WHO) [26]. The scale of each item ranges from 0 to 4 points. AUDIT is a verified tool to screen problematic drinking, which is sub-classified into hazardous alcohol use (the risk of harm) or harmful alcohol use (actual harm) [27]. The optimal cutoff scores for hazardous drinking and harmful drinking are 8 and 16, respectively, as suggested by the WHO [28].
Drinking Culture Questionnaire
This questionnaire was developed by KAF to assess the socio-cultural influences of military unit, comrades, and superiors on the respondent. It consists of nine items with a four-point Likert scale and an extra response option for ‘don’t know/no idea.’ It asks about the general culture of military units in using alcohol for recreational or socializing purposes, permissiveness towards high-risk drinking, and peer pressure (Table 1). Each item is rated from 0 to 3 except ‘In mess or after work, individuals are free to choose non-alcoholic drinks,’ which is reversely scored. The total score therefore ranges from -3 to 27. For analytic purposes, we categorized by quartile distribution: 1st quartile, three points or less; 2nd quartile, four to seven points; 3rd quartile, eight to nine points; and 4th quartile, 10 to 27 points.

Drinking Culture Questionnaire
Statistical analysis
We analyzed data using chi square tests and multivariate logistic regression with the Statistical Analysis System (SAS) statistical software package version 9.3 (SAS institute, Cary, NC, USA). A descriptive analysis of relevant variables with categorized AUDIT scores was performed using the chi-square test. We used multivariate logistic regression analyses to identify the relationships between alcohol use, work-related factors, and health status, controlling the covariates taken into account in previous studies [8,10,29-31]. In order to determine adjusted odds ratios (aORs) of hazardous alcohol users against low-risk users (those who have responded the AUDIT score less than 8) and harmful alcohol users versus low-risk users, we employed three analytic models: model I was adjusted for demographics (gender, age, marital status, and educational level); model II included occupational factors such as military rank, location of unit, working condition, working hours, and work-related stress as well as the model I variables; model III added health-related factors to model II. Statistical significance was set at p<0.05 and a 95% confidence interval (CI) was reported as appropriate.
Ethics statement
The ethics of using data from soldiers was reviewed and approved by the Institutional Review Board of Uijeongbu St. Mary’s Hospital, The Catholic University of Korea (UC17EESI0093).
RESULTS
From 3,546 professional soldiers who participated in the survey, 2,646 subjects remained for analysis (Figure 1). Comparisons of demographics, work- and health-related factors between subjects with low-risk drinking, hazardous drinking, and harmful drinking are shown in Table 2. In the descriptive analysis, 56.9% of men (1,389/2,441) and 46.8% of women (96/205) were identified as hazardous alcohol users (AUDIT 8–15), and a further 16.2% of men and 5.4% of women were found to be harmful alcohol users (AUDIT ≥16). In the chisquare tests, gender, age, marital status, educational attainment, military rank, working condition, work-related stress, life stress other than work, subjective health status, sleep quality, BMI, smoking status, depression screening results, and drinking culture demonstrated significant relationships with hazardous and harmful alcohol use.

General characteristics of study subjects
Comparison of low-risk group versus problematic alcohol groups
In multivariable regression analyses of the low-risk group versus the problematic dinking group (AUDIT ≥8), various socio-demographic, occupational, and health-related variables were identified to exert a significant influence on problematic alcohol use (Table 3). The likelihood of being a problematic drinker increased with age. It remained significant in the final model after further adjustments with occupational and health-related factors. The aOR for 26–30, 31–40, and 41–65 age groups were 1.29 (95% CI, 1.01–1.64), 1.43 (95% CI, 1.02–1.98), and 2.37 (95% CI, 1.47–3.83), respectively. The final model also found that gender and marital status are linked with problematic alcohol use (woman: aOR, 0.61, 95% CI, 0.44–0.84; and never married: aOR,1.45, 95% CI, 1.09–1.93). It was determined that past or current smoking status increased the likelihood of problematic alcohol use (past smoker: aOR, 2.12, 95% CI, 1.53–2.93; and current smoker: aOR, 2.01, 95% CI, 1.64–2.45). Drinking culture significantly influenced the risk of problematic drinking in a dose-dependent manner (2nd quartile: aOR, 1.50, 95% CI, 1.19–1.89; 3rd quartile: aOR, 1.58, 95% CI, 1.26–1.99; 4th quartile: aOR, 1.94, 95% CI, 1.48–2.55).

Multiple logistic regression analyses of low risk vs. problematic alcohol use
Comparison of low-risk group versus harmful alcohol use group
In the analysis of the low-risk group versus the harmful dinking group (AUDIT ≥16), the identified risk factors were similar to those of the problematic drinking model but showed more profound effects (Table 4). As in the prior analysis for problematic drinking, woman gender was significantly associated with a reduced likelihood of harmful alcohol use (aOR, 0.45; 95% CI, 0.22–0.91). In addition, being single was also associated with harmful drinking (never married: aOR, 1.58; 95% CI, 1.02–2.46). The chance of being a harmful drinker increased significantly with age in a dose-dependent manner with aOR of 1.70 (95% CI, 1.14–2.52), 3.07 (95% CI, 1.86–5.07), and 4.01 (95% CI, 2.05–7.85) for the 26–30, 31–40, and 41–65 age groups, respectively.

Multiple logistic regression analyses of low risk vs. harmful alcohol use
Contrary to the analysis on problematic drinking, longer working hours remained significant even after adjustments. Military personnel with longer working hours were more likely to display harmful alcohol use (50≤ weekly working hours <60: aOR, 3.04, 95% CI, 1.08–8.56; and ≥60 weekly working hours: aOR, 2.89, 95% CI, 1.03–8.12). Compared with daytime working conditions, night or shift working was associated with lower risk of harmful drinking (aOR, 0.41; 95% CI, 0.22–0.78). Although not statistically significant, work-related stress, life stress other than work, poor sleeping quality, and higher BMI displayed tendencies for association with harmful alcohol use in the final model. Smoking status again demonstrated significant association with harmful drinking but more profoundly, with current smoker (aOR, 3.85; 95% CI, 2.74–5.41) and past smoker (aOR, 4.14; 95% CI, 2.60–6.59) both showing greater risk of being a harmful alcohol user.
Drinking culture was found to exert a more profound effect on harmful alcohol use compared with problematic drinking as a whole. As military personnel reported a higher degree of tolerant drinking culture in their unit, their likelihood of being a harmful drinker increased in a dose-dependent manner (aOR, 2.36, 95% CI, 1.60–3.47; aOR, 2.28, 95% CI, 1.55–3.36; and aOR 4.85, 95% CI, 3.20–7.35 for the 2nd; 3rd; and 4th quartile, respectively).
DISCUSSION
The 2016 nationwide mental health survey conducted by the ministry of health and welfare showed a one-year prevalence of 3.5% (5.0% in male and 2.1% in female) for AUD in general population [32]. This military representative study demonstrated that 16.2% male and 5.4% female professional soldiers showed harmful use of alcohol. The harmful drinking cutoff score of 16, as suggested by the WHO [28], is far conservative than the optimal cutoff score of 12 suggested for AUD in the previous Korean validation study [33]. Therefore, this study demonstrated that the one-year AUD prevalence is at least three times higher in men and two times higher in women than those in the general population.
Many factors were identified as contributing to problematic alcohol use in this military population but the most striking was the influence of a tolerant or permissive drinking culture, and particularly on harmful use. More broadly, these findings indicate for the first time a substantial prevalence of problematic alcohol use among Korean professional soldiers. Overall, 73.1% of man soldiers and 52.2% of woman soldiers were problematic alcohol users. Man soldiers were at increased risk for problematic use. The prevalence of problematic drinking in the Korean general population was 57.5% for males and 16.6% for females, according to nationally representative surveys from 2009 to 2011 [29]. This comparison implies that military personnel of both sexes are more susceptible to unhealthy drinking behavior than the general population.
The rate of problematic alcohol use by woman soldiers presented in this study is more than triple that of the woman general population; therefore, the burden of problematic drinking is relatively higher in woman soldiers than man soldiers when compared with the general population.
There are some reasons why the negative health consequences of alcohol may be greater in women than in men. Females are more vulnerable to harm of alcohol due to pharmacokinetics. Young females have a lower activity of gastric alcohol dehydrogenase, leading to decreased alcohol metabolism [34]. The lower water to fat ratio in the female body leads to smaller volume of distribution for alcohol, which contributes to higher blood alcohol concentration in comparison to males [35]. In terms of harmful consequences, alcohol consumption during pregnancy increases the risk of malformations and developmental disorders. Although under-recognized, fetal alcohol spectrum disorder remains one of the most common preventable causes of intellectual disability [36]. Our study demonstrated that most woman military personnel (85.7%) were of childbearing age, between 18 to 40 years. Since higher alcohol use prior to pregnancy can predict the overall consumption of alcohol during pregnancy [37,38], appropriate public health measures to improve understanding of the potential harm of drinking during pregnancy are required.
Single marital status and current or past smoking were found to be associated with problematic alcohol use in this study. A number of studies have determined the relationship between drinking and various factors such as sex, marital status, educational status, military rank, and deployment status [8,9,39-42]. A US study identified that male sex, young age, alcohol dependence history, co-existence of depression and PTSD, and current smoking are related to alcohol use problems [8]. Another US study showed that male gender, service in the Marine Corps and lower educational level were related to heavy alcohol use [9]. A UK study demonstrated that heavy drinking was associated with lower ranks, young age, being single, deployment, smoking, and being exposed to combat [39].
The fact that such a high rate of problematic drinking was identified in both current and past smokers provides another important implication for military health policy. Contrary to educational, marital, or deployment status, which may not be modifiable, tobacco smoking is a risk factor that is potentially modifiable by implementing public health policies. However, smoking cessation did not seem to be effective against problematic drinking in our study, as the risk of problematic drinking was also elevated among past smokers. Possibly, biological vulnerabilities in these individuals such as reward deficiency syndrome or a shared genetic risk factor may have contributed for addictive disorders. There is also the possibility that nicotine cravings stimulate alcohol use. Although not statistically significant, the risks of problematic and harmful drinking were both higher in past smokers compared with current smokers. If nicotine cravings lead to higher alcohol consumption as a substitute for tobacco, more clinical attention should be given to other potential substance misuse in those trying to quit smoking in order to mitigate the ‘balloon effect.’
Several studies have highlighted the role of alcohol intake in the military population to cope with symptoms related to PTSD and high psychological distress levels due to combat readiness [8-10]. In this study, we were not able to include variables representing PTSD-related symptoms and combat-related deployment due to the scope of the survey and KAF’s mission to deploy its personnel for peace-keeping purposes. Instead, we included other occupational factors such as location of the unit, work stress, and life stress other than work in the analytic model. Our findings demonstrate that longer working hours for military personnel are associated with significantly higher harmful alcohol use. Even though work-related stress did not remain significant in the final model, it was associated with greater likelihood of harmful alcohol use in model II.
The most salient and arguably most important findings in the study were the dose-dependent increasing risks of both problematic and harmful drinking according to the degree of tolerant and permissive drinking culture. This study identified that a tolerant and permissive drinking culture in the military is related to increased risk of both overall problematic alcohol use and harmful alcohol use, showing a dose-response relationship. No prior research has reported this linkage except one study that reported that heavy alcohol use may play an important role in building higher comradeship [40]. The tolerant drinking culture of the military may also partly explain the lower risk of harmful drinking observed in night or shift work, when military personnel are less likely to congregate.
The drinking culture may explain in particular the increased problematic drinking among woman military personnel when compared with the woman general population. Although awareness of gender equality and women’s rights has dramatically increased in Korean society, the ‘masculine’ culture may still predominate in the military due to the widespread ‘obey to command’ notion. In order to avoid exclusion from the group or prove that they are as strong as men, woman military members may be reluctant to turn down drinking offers and also fall under the strong drinking culture of the military.
To the best of our knowledge, this is the first study demonstrating the effect of a collective drinking culture in military units on individuals’ problematic alcohol use. While no previous studies exist for the military population, it has been demonstrated that neighborhood or racial norms may influence drinking behavior [43,44]. In a student population, Kypri et al. [45] found that the hall of residence (for example, fraternity) had a strong influence on individuals’ drinking.
Greater risks of problematic and harmful alcohol use were found with increasing age in our study. In a separate analysis, age showed a strong correlation with service years (r=0.84, p<0.001). Such dose-dependent relationship of age hints that military service per se may actually be an occupational hazard for drinking problems. The drinking culture may be a moderating factor for this occupational hazard. Further research is required to determine how longer service period (exposure) contributes to both problematic and harmful alcohol use. Nevertheless, our findings should urge policy makers and health professionals in the military to consider public health means to change drinking culture and reduce problematic alcohol use in the military. Public health policies for stronger regulations on alcohol drinking and more active health promotion campaigns are needed to promote safer use of alcohol.
In addition to such preventive efforts and education, military authorities should allocate more resources for earlier identification of at-risk drinkers to prevent alcohol-related diseases, accidents, injuries, crimes, and non-combat loss of life. To better implement such polices, further research is needed to reveal which factors–comrades, superiors, or the general atmosphere of the unit–contribute to military drinking culture. More effective policy making could then be achieved by enabling strategic priorities, better prevention, and treatment program development in the military.
In conclusion, this study demonstrates a prevalence rate of problematic alcohol use in a representative health survey of Korean professional soldiers of 73.1% in men and 52.2% in women, and identifies several risk factors for hazardous and harmful alcohol use, notably the drinking culture. We found that AUD prevalence is at least three times higher in the man and twice higher in the woman professional military population than those in the general population. The results of this study emphasize planning and implementation of public mental health policies to prevent alcohol-related diseases, injuries, and crimes in the Korean military by addressing its unique drinking culture.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are not publicly available due that the conduct of the survey and the management of the survey data have been done by the Armed Forces Medical Commend under the Ministry of National Defense but it may be available from the Armed Forces Medical Command on a formal reasonable request.
Conflicts of Interest
Seung-Yup Lee, a contributing editor of the Psychiatry Investigation, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Author Contributions
Conceptualization: all authors. Data curation: all authors. Methodology: Seung-Yup Lee, Hae Kook Lee, Chang-gyo Yoon. Writing—original draft: all authors. Writing—review & editing: Seung-Yup Lee, Hae Kook Lee, Chang-gyo Yoon.
Funding Statement
None