INTRODUCTION
Sound-based intervention encompasses dedicated therapy that utilised any form of sound for interventions. This is in line with the definition of sound that is characterised by the movement of air particles back and forth and audible in the human brain [1]. The terms music and sound have been used interchangeably when referring to music or sound therapy. Specifically, sound is a generic term that includes include all sound types while music is specific to a sound that is arranged and produced with features such as melody, rhythm, harmony, and so on. To simplify, music is a subcategory of a sound. Nevertheless, both are used for interventions by adjusting and modulating the pitch, frequency, tone, and intensity [2]. The term ‘sound-based intervention’ is used in this article for consistency and to avoid confusion.
Throughout history, sound has been regarded to possess healing properties and is used in a variety of ways globally. The first report of this intervention in rehabilitation was back in the 1940s when it was used to treat mental health issues among soldiers that had experienced psychological issues following World War II. Since then, it has evolved and adapted to fit specific functions and applications in different settings. Auditory integration training (AIT), the Tomatis method, and the Samonas method are all well-known forms of therapy. The similarity between these methods is that each involves the process of listening to electronically modified music through headphones for a specific period. Nevertheless, each method adapts its own music and sound, which is customised based on the patient’s condition and severity. Sound therapy is commonly used in treating tinnitus, sound hypersensitivities, mental health problems and disorders, such as attention deficit hyperactivity disorder (ADHD) [3,4] and autism spectrum disorder (ASD) [5]. Numerous individuals have asserted the benefits of the method as a well-established alternative treatment for a variety of diseases. The therapeutic effects of sound therapy were reported to enhance the development of emotion, imagination, perception, and stimulating conversation [6].
Sound therapy has been used as a part of intervention among the ASD population to alleviate their associated symptoms [6,7]. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), ASD is defined as difficulties with social interaction and behaviour, specifically the inability to initiate and sustain social discussion and interaction. Affected children may demonstrate restricted, repetitive patterns of behaviour, interests, or activities in response to objects, motor movement, daily routine, intensity, or sensory input [8]. The symptoms manifest during the child’s early years and might limit or prevent them from engaging in daily activities [8]. While ASD has no definitive cure, intervention or treatment has been found to diminish or alleviate its indicators or symptoms [9]. Resultantly, early intervention is critical for a favourable outcome. Patients with ASD exhibit unique traits and severity, necessitating the establishment of numerous versions of therapies [7]. Therefore, several intervention methods have been developed to address the symptoms with these goals in mind.
In the same vein, researchers have made a collaborative effort to demonstrate the efficacy of sound therapy in alleviating ASD symptoms. The majority of research demonstrates significant improvements in symptom reduction and improvement, demonstrating the efficacy of this method [9,10]. In contrast, a few studies reported no significant improvement following sound therapy intervention, thereby complicating the findings and casting doubt on the efficacy of sound therapy [11-13]. A few review articles have attempted to address this issue by either assessing the efficacy of sound-based interventions for ASD or synthesising the current body of knowledge regarding sound therapy intervention. Music- or sound-based intervention have been demonstrated to improve autistic behaviour, language, social and communication abilities, and auditory processing in a few systematic reviews [14-16]. Meanwhile, other review articles stated that there is a dearth of research to support the use of sound-based interventions [17-19]. A review by Villasenor et al. [20] reported a lack of evidence to support the improvement related to children with sensory processing in education participation after sound-based intervention due to limitations in methodology. Likewise, Weitlauf et al. [21] discovered that the evidence is small and warrants a thorough investigation. It is thus difficult to conclude the efficacy of sound therapy given the inconsistent findings in and between research articles.
Different methodological issues have been identified as the underpinning reasons for the lack of evidence to support the effectiveness of sound-based interventions. Some of the drawbacks in most studies include small sample size, lack or complete absence of a control group, short-duration intervention, maintenance of long-term effect, and study designs such as case studies or single-subject research designs without outcome measures. A few technical aspects of sound intervention such as training duration were also not mentioned in the previous systematic reviews. The rationale of the current scoping review is to provide an overview of the existing evidence for sound-based intervention therapies for ASD individuals. To date, no scoping review on the use of sound therapy intervention for individuals with ASD has been conducted. A scoping review was determined to be the most effective method for achieving the study objectives since it is exploratory and encompasses several research approaches, with an emphasis on breadth rather than depth.
This study summarises the present state of the literature on the use of sound therapy interventions in ASD and highlights the gaps that will guide future research in this area. The research questions of this scoping review are as follows: 1) what are the known sound-based intervention among ASD in the literature and 2) what other information has not been explored from previous literature.
METHODS
A scoping review research design was employed in this study to identify, collect, clarify, examine, and analyse all relevant studies, before mapping them into a single reference [22]. This review was conducted based on the Joanna Briggs Institute framework of PRISMA-ScR [22]. The five stages are outlined as follows: 1) identify the inclusion criteria, 2) search for relevant studies, 3) studies selection, 4) data extraction and charting, and 5) data analysis and presentation. This scoping review study was approved by International Islamic Univerity Malaysia Research Ethics Committee with the identification number (IREC 2020-063).
Stage 1: identify the inclusion criteria
This scoping review aimed to gather and map evidence from relevant studies regarding the use of sound therapy as an intervention for ASD. Specifically, this review sought to summarise the evidence from relevant studies regarding the use of sound therapy as an intervention for ASD, identify the test parameters utilised in sound therapy with ASD individuals, and identify the types of sounds employed and their associated outcomes concerning ASD symptoms. The selected articles were based on the following criteria: 1) the population focuses on individuals with ASD, 2) studies involved soundbased therapy as a type of intervention, and 3) articles published in English, Malay, and Indonesian languages. Studies on other population disabilities, different interventions, and articles published in forms other than peer-review original articles and the indicated languages were excluded from this review.
Stage 2: searching for relevant studies
Five online databases namely Google Scholar, PubMed, CINAHL, MEDLINE, and Scopus were used to identify the relevant literature via keywords combination. The keywords combination were 1) autism AND sound therapy OR auditory integration therapy OR Tomatis sound, 2) autism spectrum disorder AND sound therapy OR auditory integration therapy OR Tomatis sound, and 3) autistic disorder AND sound therapy OR auditory integration therapy OR Tomatis sound. The keywords were combined using the Boolean operator ‘AND’ and ‘OR’ to widen the search results and ensure the keywords are present in the articles. The earliest articles dated from the 1st January of 1997 were chosen to reflect the first introduction and publication for sound-based intervention for the ASD population until 31st December 2020.
Stage 3: selection of studies
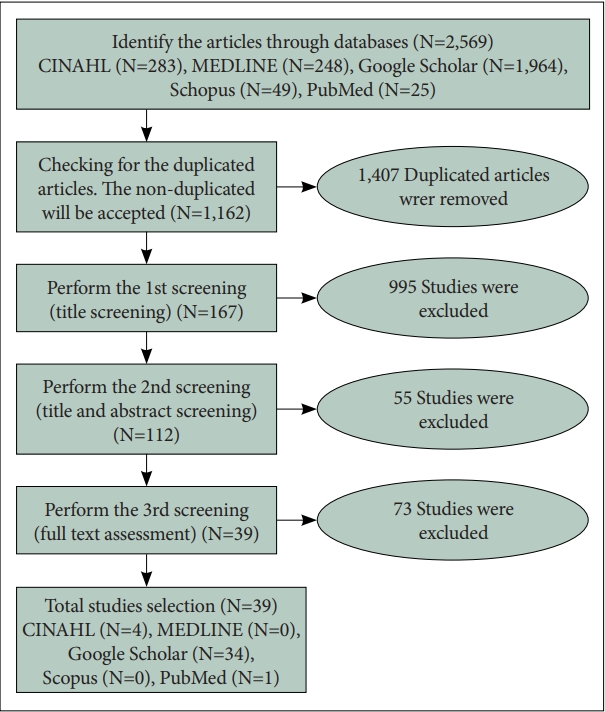
This step involves identifying, removing, and screening articles obtained from the five databases. The initial search yielded 2,569 records (Figure 1). A total of 1,407 duplicate articles were identified and removed, resulting in 1,162 remaining articles for the screening process. The screening process involved three steps; title screening, title and abstract screening, and full-text screening. Following the inclusion and exclusion criteria described above, 167 articles were screened based on their titles and 995 were removed. From the 167 articles, 55 were removed for not fulfilling the language and intervention criteria based on the title and abstract screening, resulting in 112 articles for further screening. Thirty-nine articles were finalised after reading the full-text articles. The remaining 73 articles were excluded as they did not correspond to the type of intervention, had missing pages, or could not be accessed. Forty-one review articles were removed after considering the possibility of redundancy between articles in the reviews and the present study. Thus, a total of 39 articles were selected for this study. Figure 2 shows the summary of the article selection process. Two independent reviewers were involved to minimise the risk of bias while maintaining consistency and accuracy. Any disagreements between reviewers were resolved before finalising the total number of articles.
Step 4: data extraction and charting
The data and information from the 39 articles were extracted and charted as listed: the author, year of publication, type of study, characteristics of the studied population, study aspects, duration of intervention, assessment tools, and key findings. All the relevant data and information were extracted and charted.
Step 5: data analysis and presentation
Thematic analysis was used to generate themes in response to discussion among reviewers regarding the data and study objectives. All articles were first familiarised by reading through the articles and determining the vital points, which were then highlighted and coded. Coding was determined by extracting important data from the articles before assigning a keyword (code) to represent the content of the articles. All the codes were collated by the reviewers to identify the patterns and generate themes. Meanwhile, the data with similar characteristics were grouped into a single overarching theme. The themes had a broad scope in order to encompass as many articles as possible while also representing the study objectives. Thereafter, the themes were reviewed and finalised with the agreement of all authors, as detailed in the results section. The data were analysed based on the themes associated with research articles and other types of publications using simple descriptive studies. All findings were presented per the research questions and objectives of the study. Finally, detailed information from each study was summarised, including the author, year, type of sound therapy, duration of intervention, methodology, and findings.
RESULTS
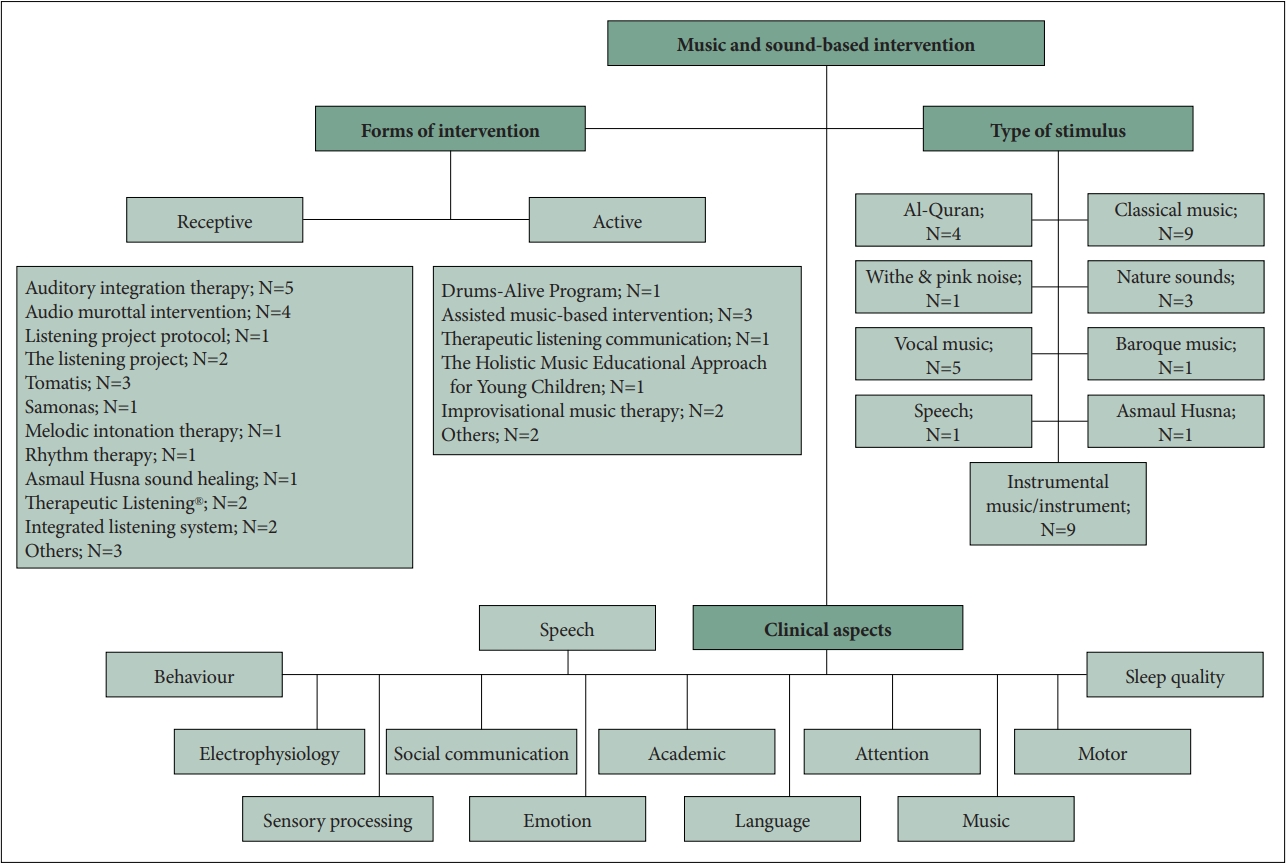
A total of 39 peer-reviewed original research articles were selected and analysed based on four themes derived from the primary results and objectives of each study. The four major themes were 1) forms of sound therapy, 2) duration of the intervention, 3) clinical characteristics of the intervention, and 4) evidence for the effectiveness of the intervention. Overall, this scoping review discovered 16 forms of sound-based intervention; nine types of stimuli; varied listening time, overall listening hours, and the total number of listening sessions; social communication and behaviour as the most researched clinical aspects; with more than half of the articles reporting positive findings. Figure 3 summarises the findings from the original research article based on the themes presented below.
Theme 1: sound-based intervention and stimulus (n=36)
A total of 36 research articles investigating sound-based interventions among ASD children were identified.
Forms of sound-based intervention
Receptive therapy was used in 26 of the studies while the remaining 10 utilised active therapy. Active music therapy is when the patient or client engages in the act of creating music such as playing a musical instrument, singing, songwriting, and conducting. Meanwhile, in receptive music therapy, the clients or patients go through the process of listening to live or recorded music. From 30 peer-review research articles, 16 distinct types of sound therapy were identified while the remaining six articles did not specify the type of sound therapy employed. AIT (five articles) and audio murottal intervention (AMI) (four articles) were regularly used in conjunction with other sound therapy methods identified in this study.
Types of stimuli
From the 36 studies, nine stimuli were found which included vocal music, instrumental music/instruments, Al-Quran, classical music, nature sounds, speech, Asmaul Husna, baroque music, and white/pink noise. However, nine studies did not specify the type of stimulus used. The stimuli that were mostly implemented by previous studies were instrumental music/instruments (nine studies), classical music (nine studies), and vocal music (five studies). Notably, a few articles implemented more than one stimulus but all studies except two (Asmaul Husna and melody from “Ah vous dirai-je, Maman” by Mozart) did not specify the title for the kinds of music or verses used. The sound-based interventions that were used to process or modify music/sounds were AIT, listening project protocol (LPP), Tomatis, Samonas, and Therapeutic Listening® (TL).
Theme 2: duration of intervention (n=35)
The duration of the intervention varied from four weeks to eight months in several trials employing sound therapy. Each study had different frequencies of intervention ranging from once to five times per week and once per month. Due to this variation, the information entailed the listening time of each session (in minutes), the overall listening hours, and the total number of listening sessions for each study were analysed instead of using hour, day, and week.
Based on Figure 4, the average listening time spent on each session was around 15 to 30 minutes. The shortest session documented was 11 minutes 19 seconds while the longest was around 6 to 8 hours. As for the listening session, about onethird of the research utilised a maximum of 10 sessions with a minimum of four sessions. The other one-third of the research had more than 30 sessions with the highest of 112 sessions. The differences in the overall listening session were partly contributed by the daily listening in which 21 studies had one listening session per day, seven studies had two sessions per day, and the other seven did not state the daily listening. The total listening hours were as follows: five hours and less (eight articles), 6 to 10 hours (nine articles), 16 to 20 hours (three articles), one article for 21 to 25 hours, eight articles for more than 30 hours, and the other six were not stated.
Theme 3: clinical aspects of interventions (n=39)
Clinical aspects refer to the observable presentation of symptoms related to the disorder. These studies examined various aspects of ASD and the research differed from one to another. The authors either focused on single or multiple targeted ASD abilities. In this context, multiple refers to more than one aspect of ASD. Of the 39 studies included in this section, 14 of them focused on a single clinical aspect while the remaining studies focused on more than one clinical aspect.
The most studied clinical aspect (including both single and multiple) was social communication (n=19). Overall, different skills of social communication have been studied, such as receptive communication, communicative behaviour, social awareness, social cognition, social interaction, social orienting, joint attention, and imitation. Subsequently, the behavioural aspect specifically looking at hyperkinetic movement, stereotypic-repetitive behaviour, self-stimulatory, and aberrant behaviour was studied in 15 articles, followed by the sensory processing aspect in nine articles; comprising sensory processing disorder and auditory hypersensitivities. As previously stated, ASD is characterised by difficulties with social communication and behaviour, which supports the reason for the majority of the research to specifically target the two clinical aspects.
Theme 4: evidence of the effectiveness (n=39)
The effectiveness of sound therapy was reviewed based on the findings of each study and they were classified as either positive, negative, or mixed. The outcome of the studies was deemed favourable or positive if it has a beneficial effect or provides improvements. Meanwhile, negative outcomes were labelled as such when they indicate a poor outcome or no change. Mixed findings referred to studies that produced both positive and negative outcomes. The effectiveness was categorised according to the type of sound therapy.
Positive findings
Positive results were produced from 27 of the 39 studies. This includes four studies of AMI, three studies of auditory integration therapy, two studies of TL, two studies of Tomatis sound, three studies of assisted-music based interventions, six studies on other forms of sound therapy, and one session each of LPP, the listening project (TLP), melodic intonation therapy, Samonas, Drums-Alive Program, The Holistic Music Educational Approach for Young Children, and improvisational music therapy (IMT). Positive findings in these studies were found in aspects such as social communication, speech, behaviours, sleep quality, electrophysiology, and education.
Negative findings
Negative outcomes were reported in five studies, including those conducted by AIT, Tomatis, Asmaul Husna sound, and other forms of sound therapy. Aspects such as sound processing, behaviour, language, social orienting, motor development, and music reflected negative findings in a way that suggest deterioration or no changes.
Mixed findings
Seven studies produced mixed findings; including TLP, rhythm therapy, integrated listening system, therapeutic listening communication, IMT, and other forms of sound therapy. The evidence on the effectiveness of sound treatment based on forms of sound-based intervention is summarised in Table 1.
In summary, it was difficult to determine which of the listed interventions and characteristics (duration, type of sound, and method) were the most effective due to a dearth of study in this section. Each intervention probably yielded different results in terms of the clinical aspects of ASD. Some interventions might also be beneficial in treating specific clinical aspects of ASD. Depending on which aspect is being addressed, each clinical aspect might need different parameters or/and types of sound therapy to achieve the best result from the intervention.
DISCUSSION
This scoping review aimed to elucidate the evidence for various methods of sound therapy intervention in ASD individuals and to provide a general overview of the use of sound therapy as an ASD intervention. Sound therapy may be an effective strategy for ASD, as growing evidence of its efficacy indicates a favourable outcome. Almost half of the articles reported positive findings in a variety of clinical areas spanning all forms of sound therapy, whereas the remaining articles found negative and mixed findings. The outcome of the scoping review was coherent with previous systematic reviews, demonstrating inconsistent findings across the original and review articles [2,17,19,23]. This scoping review also demonstrated that sound therapy has the potential to provide therapeutic effects in ASD intervention. Nevertheless, further systematic studies are required to verify the positive effects as it is still considered to be experimental in nature [15,17-19,23,24].
Inconsistent results were reported in the reviewed studies due to certain components, such as treatment duration and type of stimulus that were not clearly classified. Hence, the conclusion of the previous systematic reviews can be questioned without considering the factors that were mentioned earlier. A more comprehensive review that systematically normalised all those factors is needed to ensure that a firm conclusion could be drawn. In addition, current evidence for the efficacy of music therapies in children with ASDs emanates from a handful of studies lacking systematic study designs, assessments, and treatment protocols [25]. The majority of the studies were exploratory with a limited sample size, thereby resulting in poor generalisability of the outcome [18]. With no or lack of control/placebo group in pre-and post-test raises questions on the outcome reliability and validity; whether the changes observed or measures were truly the result from the treatment [18]. Thus, this result should be interpreted cautiously since there is no strong evidence demonstrating its efficacy in reducing symptoms and additional research is necessary to fill in the knowledge gaps identified in previous studies.
The findings of this study revealed that the various types of sound used in previous studies are beneficial for ASD individuals. The characteristics of the sound could act as cues and attraction, assisting affected individuals in social interaction, communication, and connection [26,27]. Individuals with ASD have a severe deficiency of time synchronisation between the areas of speech perception and production. Hence, sound therapy assists to organise synchronisation between those areas by providing neuronal connections, thereby improving the physiological function, in this case, language [26,27].
With the wide variety of stimuli ranging from music, voice, Quranic verse, and natural sounds, it is challenging to identify the types of sound that provide the best efficacy. Therefore, more research is needed to elucidate these events. Most studies presented one or two types of stimulus in the intervention while the majority of the sounds were modified electronically, either classical, vocal, or instrumental music as it is more engaging for the child. The majority of the studies arbitrarily choose sound for sound-therapy based intervention without any systematic investigation. The only study that employed a systematic and scientific basis for choosing of sound for intervention was conducted is by Cibrian et al. [28] in which melody from musical instruments was used based on its influence on child attention and emotions. Currently, there is a lack of understanding and appropriate model to explain the relationship between ASD and sound, therefore specific sound and interventions to suit any model have not yet been established. A proper model or framework may be needed as in the case of The Moderate Brain Arousal model in the ADHD population [29]. Introducing white noise to ADHD individuals triggers the phenomenon of stochastic resonance where a certain amount of noise may facilitate cognitive performance, thus potentially reducing ADHD symptoms.
The scoping review also suggests the need to establish objective and standard outcome measure methods that can determine the effectiveness of each sound (types, arrangements, pitch, and other factors) in sound-based therapy intervention in ASD children. Mindwave band is one of the techniques that can measure stimulus efficacy. Mindwave band is used to measure the changes in attention as seen in the study by Cibrian et al. [28]. Changes in attention are observed while listening to the presented sounds and the outcome determines the type of stimulus that affects attention the most. Although it is still in trial, the findings indicate that the method is useful in determining the preferred sound. Another possible technique to measure effectiveness is the suppression of otoacoustic emission (OAE), which was used previously [30,31]. This technique measures the sensory gating aspect when presented with different sounds to determine the sound with the highest suppression. A child with ASD has a lower suppression effect in comparison to a normal child due to the sensory gating deficits causing sensory processing difficulties [31]. It is hypothesised that by listening to sound with the highest suppression, the sensory gating process can be improved, thus explaining why this method was suggested to investigate the effectiveness of the stimulus [30]. Finally, the sounds obtained from these studies can be analysed for further understanding of its effect by using digital signal processing technique [14]. Gathering all the information on similarities of the sound that provide the therapeutical or beneficial effect on ASD is crucial for effective sound therapy. Furthermore, it will provide a better understanding of ASD sound preferences.
Additionally, this study determined the duration of the intervention and its clinical characteristics. The duration of sound therapy varied among the reviewed studies and key information was lacking within the actual duration of sound therapy. Therefore, it is difficult to identify the optimal duration for reducing or alleviating ASD symptoms. The key information in the sound-based intervention that needs to be factored in the statistical analysis includes the rest time between listening sessions, daily listening (once or twice per day), and other parameters. This information is currently lacking evidence across studies, thereby reducing the chances of making a solid and reliable conclusion. The relationship between duration and frequency of auditory training and the benefits achieved also remains unclear [32]. A previous study suggested that a minimum of four weeks of intervention (generally preliminary studies) is required to achieve the desired treatment outcome [33] while other studies suggested a minimum of two weeks of clinical sessions and eight weeks of home programs for the best result [34]. Notably, the suggestions were based on researchers’ observations and experience from conducting sound therapy studies, which explains the variation between studies. As different studies implemented different methodologies and parameters, the effective duration might differ and reduces the chances of generalising the results to others. In addition, the treatment duration has always been measured in periodical terms (day, week, and month), which creates confusion when determining the effectiveness of sound therapy. A suggestion for future studies is to measure the duration by the amount of exposure from treatment (total listening hours), which will make it more consistent and easier to analyse the effectiveness. A study dedicated to this matter is vital if sound therapy is to be implemented as part of ASD intervention. The researcher must ensure the methodology and parameters are consistent throughout the experiment while varying the duration to achieve valid and reliable results. This information will be useful to establish protocol and policy for sound therapy if it is to be implemented in clinical settings.
In terms of clinical aspects, social communication and behaviour are the most frequently studied in ASD populations. This is primarily due to the way ASD symptoms are typically presented. Features of social communication discussed in these studies include receptive communication, communicative behaviour, social awareness, social cognition, social interaction, social orienting, joint attention, and imitation. Similar to previous reviews, the present findings reflected positive trends in the social communication aspects after treatment [24,35,36]. For behavioural aspects, hyperkinetic movement, stereotypic-repetitive behaviour, self-stimulatory, and aberrant behaviour were among the features found in this study. The outcome for behaviour aspects produced positive trends [26,37-39], which is in agreement with prior reviews [35]. Meanwhile, other studies reported no changes in behaviour and even a deterioration after the sound therapy intervention [12,13,36]. Furthermore, the carry-over effect on the positive outcome (long-term result) is still inconclusive as only a few studies investigated this effect through follow-up testing; usually, after three or six months of intervention [12,27,34,37-40]. Nonetheless, additional aspects of ASD are being explored as new information about aetiology emerges from ongoing research, providing a better understanding of the disorder.
The potential of sound therapy demonstrates unequivocally that it can be developed into a more effective intervention for ASDs. This could be achieved by addressing the knowledge gaps identified in this study. To begin with, there is a dearth of research on specific types of sounds, which makes it difficult to synthesise data and choose the appropriate sound to incorporate into sound therapy interventions. Data extraction also revealed a large range of durations, complicating cross-record comparisons. There is also data paucity on the use of technology in sound therapy interventions (assistedbased sound therapy) and issues arising from using a small sample size. Assisted-based sound therapy implements the use of technology in the intervention to enhance its efficacy and to obtain more apparent results. Technologies such as robots, virtual reality and 3D applications have been widely commercialised and used but the ideas of implementing this technology in sound therapy are still novel and experimental. While the studies [40,41] reported positive trends after using this method, the evidence is weak as they were all preliminary studies. Hence, further investigation with random-controlled trials and a larger sample size is required. Furthermore, there is no information on the appropriate type of sound therapy to address specific clinical characteristics. This knowledge will be able to cater for those that exhibit symptoms that require attention. Finally, only a few articles discussed the interaction of interventional clinical characteristics.
As research in this area continues to gain more attention, the development of sound-based intervention allows for better intervention of ASDs. The study trend in sound intervention over the last three years has focused more on the incorporation of technology (virtual technological robots), which has demonstrated beneficial outcomes. These outcomes were reported in previous research where the combination of technology and music boosted the attractiveness, involvement, and emotion of ASD children during the intervention [40,41]. By addressing the limitations discussed earlier, the implementation of technology and sound-based intervention will provide effective intervention, thus generating beneficial effects for ASD individuals.
Future research should focus on addressing the knowledge gaps discussed previously in order to provide a comprehensive sound therapy intervention. It is important to investigate the various types of sound and their uses, as well as to determine the best methods to obtain optimal sound. Custombased sound therapy which entails the provision of a suitable sound to each autistic child based on their preferences or objective measure, such as OAE, can also be considered in future since ASD is a spectrum disorder. Additional research is needed to determine the best appropriate duration of intervention and its effectiveness. Similarly, new technology or additional tools for music therapy intervention, such as auditory training and memory training are necessary. Such tools can upgrade the potential of sound therapy to cater for different clinical characteristics of ASD in a single intervention. Future research should also focus on establishing effective methodologies and parameters of sound therapy to determine the generalisability of the study.
Conclusively, a total of 39 papers were examined and analysed, which revealed that 16 sound-based interventions and nine stimuli were used in the experiments. Differences in duration and clinical characteristics were also observed. The evidence of effectiveness was more favourable to positive impacts. Although evidence and reviews for effective therapy and study have been ongoing for a long period, there is data paucity to draw conclusions about the effectiveness of the intervention. Moreover, the evidence presented by most studies is weak due to the limited sample size, unverified methodology, absence or lack of a control/placebo group, and insufficient follow-up investigations. Thus, more research addressing these issues is required to further clarify the effectiveness of this intervention.