A 24-Month Effects of Methylphenidate Use on Growth in Children and Adolescents With Attention Deficit Hyperactivity Disorder
Article information

Abstract
Objective
The primary objective of this study was to investigate the effect of methylphenidate (MPH) on height, weight, and body mass index (BMI) in drug-naive children and adolescents with attention deficit hyperactivity disorder (ADHD) over 24 months. The secondary objective was to investigate whether the age of MPH initiation and sex act as risk factors for growth retardation.
Methods
A total of 82 patients with ADHD were included. Weight, height, and BMI were measured at baseline and every 6 months up to 24 months. Weight, height, and BMI data were converted to z-scores and analyzed using two-way repeated-measures ANOVA and multiple linear regression.
Results
The z-score of height, weight and BMI decreased from the baseline values. The z-scores of height were at baseline 0.002; 6 months -0.100; 12 months -0.159; 18 months -0.159; 24 months -0.186. The z-scores of weight were at baseline 0.104; 6 months -0.155; 12 months -0.256; 18 months -0.278; 24 months -0.301. Here were no age and sex differences of height, weight, and BMI.
Conclusion
The use of MPH was associated with attenuation of weight and height gain rates in children and adolescents with ADHD.
INTRODUCTION
Attention deficit hyperactivity disorder (ADHD) is one of the most common psychiatric disorders in children and adolescents. The prevalence of ADHD among children and adolescents has been reported to be in the range of 2%–17%, depending on the diagnostic criteria and sample population [1]. In a meta-analysis of 175 studies including 1,023,071 subjects over 36 years, the estimated prevalence of ADHD was found to be 7.2% [2].
ADHD is a neurodevelopmental syndrome characterized by deficits in attention, hyperactivity, and impulsivity that can cause persistent problems in learning, peer and family relationships, as well as in time and financial management. ADHD is often accompanied by other psychiatric disorders, such as learning disorders, oppositional defiant disorder, or anxiety and mood disorders. Proactive, long-term treatment for ADHD is advised because it can improve the functional outcomes of patients with ADHD and comorbid conditions [3]. In addition, ADHD is associated with an increased risk of early mortality, suicide, drug abuse, automobile accidents, and crime [4].
Methylphenidate (MPH) is the most commonly used drug for the treatment of ADHD. In the United Kingdom, 88.9% of patients on medication for ADHD between 1995 and 2015 were prescribed MPH, and the prescription rate has shown an annually increasing trend [5]. MPH is used to ameliorate ADHD symptoms, such as hyperactivity and impulsivity, as well as improve angry outbursts, cognitive function, social and intra-family function, and learning. It also has a positive effect on reducing absenteeism [6]. MPH has shown higher efficacy than non-stimulant drugs. However, there are some adverse effects associated with MPH use, including sleep disturbances and a reduction in appetite. In addition to symptom management in children and adolescents with ADHD, it is also important to pay attention to the patient’s age, drug sensitivity, and adverse effects [7].
Anthropometrically, growth is determined by complex interactions among numerous genetic, hormonal, nutritional, and psychosocial factors. Studies on the effects of MPH on growth have shown diverse results. When MPH was used for 18 months in 298 patients with ADHD, aged ≤18 years, a significant decline in body mass index (BMI) and height z-scores were observed, and the medication dosage was weakly correlated with the changes in BMI and height [8]. In contrast, Harstad et al. [9] performed a longitudinal study with 340 children and adolescents with ADHD and 680 controls, and reported that the use of psychostimulants was not associated with changes in peak height velocity or final adult height. A 10-year longitudinal study comparing 137 children with ADHD and healthy controls revealed that stimulants did not lead to growth retardation [10]. Furthermore, racial differences have been reported in relation to the efficacy and adverse effects of MPH [11].
The first objective of the present study was to investigate the changes in height, weight, and BMI when MPH was used for 24 months in children and adolescents with ADHD in South Korea. The second objective was to investigate whether any sex-specific differences are associated with the changes in height, weight, and BMI following MPH therapy and whether any changes were associated with the age at initiation of MPH.
METHODS
The subjects in this study were 6–15-year-old pediatric patients who visited the Psychiatry Department of Yeungnam University Hospital in Daegu, Korea between December 2007 and August 2019 and were diagnosed with ADHD based on the Diagnostic and Statistical Manual of Mental Disorder, 4th edition, text revision (DSM-IV-TR), or DSM 5th edition diagnostic criteria. The exclusion criteria were as follows: 1) patients with an organic brain lesion, such as cranial trauma or a tumor; 2) patients with systemic diseases affecting growth; 3) patients receiving hormonal therapy for precocious puberty; 4) patients with a z-score of >3 or <-3 for height or body weight before initiation of MPH; 5) patients who had taken stimulants for at least 1 year or non-stimulant drugs, such as atomoxetine, before participating in the study; and 6) patients with a percentage of the dose taken correctly (PDTc) of <80%.
The extent of ADHD symptoms was measured using the Korean version of the Swanson, Nolan, and Pelham Rating Scale, and accompanying diseases were assessed using the Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version-Korean version [12]. All subjects underwent baseline evaluation and were prescribed one MPH formulation (osmotic controlled-release, extended-release, or immediate-release) from day 14 to day 28 after baseline evaluation. The subjects visited the hospital as outpatients once per month. Symptom severity, MPH medication compliance, MPH effects, and adverse effects were examined. When patients complained of severe adverse effects, their drug treatment was suspended or the dose was reduced. At each monthly outpatient visit, the subjects’ height and weight were measured under the same conditions using the same anthropometric device. To measure body weight, the subjects removed their coats and shoes, and wore light clothing. Height was measured with the subjects in a standing posture, from the heel to the vertex.
We retrospectively collected data on height and weight, drug prescription records, and medical records in the course of clinical treatment, before initiating MPH, and also 24 months later. Height and weight measurements at baseline and at 6, 12, 18, and 24 months after commencing MPH were converted to height (cm), weight (kg), and BMI (kg/m2) z-scores using the lambda value for skew, mu for the median, and sigma for the generalized coefficient of variation (LMS) values given in the standard growth charts published in 2017 by the Korea Centers for Disease Control and Prevention [13]. The LMS method calculates the standardized growth percentiles by age using the L (Box-Cox Power), M (Median), and SV (Coefficient of Variation) values, and the z-scores calculated by this method were adjusted for age and sex [14,15]. In addition, the differences in growth were compared between male and female patients and across age groups (<9 years, 9–12 years, and ≥12 years) at the initiation of drug treatment. Because of the retrospective design of the study, we were exempted from obtaining patient consent. The study was approved by the Institutional Review Board (IRB) of the Yeungnam University Hospital (IRB No. YUMC 2019-05-032-002).
Demographic data were analyzed using descriptive and frequency analyses. Two-way repeated-measures analysis of variance was used to test whether there were significant changes in height, weight, or BMI in relation to the time after taking MPH, and to test whether the changes differed by sex or age at the time of initiation of MPH. Bonferroni’s method was used for post-hoc testing. Additionally, multiple linear regression was performed to assess the possible contribution of different factors as independent variables, considering height and weight z-scores at follow-up as the dependent variables. The regression was controlled by sex and age. In all statistical tests, a p-value of <0.05, was considered statistically significant. All statistical analyses were performed using IBM SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Demographic characteristics
A total of 240 patients were included in the study. 98 patients were excluded based on the exclusion criteria. Thus, 142 patients were included in the baseline evaluation. After the baseline evaluation, we excluded 60 inappropriate patients. Therefore, data from the remaining 82 patients were included in this study (Figure 1). The mean age of the patients was 8.17±1.93 years, and 64 patients (78.0%) were males. There were 57 patients aged <9 years (69.5%), 19 patients aged 9–12 years (23.2%), and 6 patients aged ≥12 years (7.3%). The mean z-scores for height and weight before the initiation of MPH were 0.02±1.06 and 0.10±0.94, respectively (Table 1).

Flow chart for 24 months of recruitment and attrition from the study. The figure reports the number of patients included in weight and height analysis. The reasons for which the patients were excluded from analysis were also explicated. ADHD, attention deficit/hyperactivity disorder; MPH, methylphenidate; ATX, atomoxetine; PDTc, percentage of dose taken correctly.

Baseline demographic and clinical characteristics of 82 ADHD patients (N=82)
Changes in height, weight, and body mass index every six months after MPH use
The changes in the mean z-scores for height, weight, and BMI were compared with the baseline values every 6 months for 24 months of MPH treatment. Overall, there was a change in height, weight, and BMI over the 24-month follow-up. The z-scores for height and BMI decreased after 24 months compared to the baseline values (p<0.05). Moreover, z-score for weight decreased significantly after 24 months (p<0.001) (Table 2). There were differences in the patterns of reduction in height, weight, and BMI. While the decline of z-scores in height and BMI was reduced at 18 months, the weight z-score showed a prominent reduction in the first 6- and 12-months after MPH use, and this pattern of decline was sustained (Figure 2).

Comparison of body height, weight, and BMI of 82 ADHD patients for 24 months (N=82)
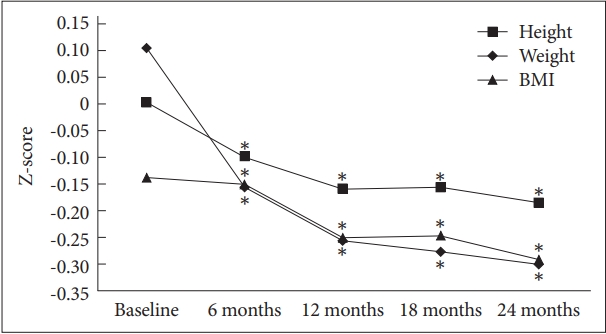
Height, weight, and BMI Z-score at baseline and after MPH treatment in 82 ADHD subjects. BMI, body mass index; ADHD, attention deficit hyperactivity disorder.
Comparison of the changes in height, weight, and body mass index by sex
The z-scores for height at baseline were 0.097±0.968 for males and -0.338±1.311 for females, indicating that female patients had a shorter mean height. The z-score for weight at baseline was 0.231±0.928 for males and -0.348±0.887 for females. When the changes in height following MPH use were compared, the difference in z-scores between male and female patients was not significant over the 24-month follow-up. However, there were sex differences in the z-scores for weight and BMI (p<0.05). The weight and BMI z-scores of males persistently decreased over time, but the weight and BMI z-scores of females decreased up to month 12, after which they recovered slightly. However, according to regression analysis, sex did not predict final height, weight, or BMI (p>0.05) (Table 3).

Comparisons of body weight, height, and BMI z-scores by sex
Comparison of changes in height, weight, and body mass index by age after initiation of methylphenidate
The patients were divided into three groups according to their age of MPH initiation (<9 years, 9–12 years, and ≥12 years), and the changes in height, weight, and BMI z-scores following MPH treatment were compared. There were no significant differences in height, weight, or BMI among the three groups. The <9 years group showed a continually decreasing trend in height z-score up to 24 months. In contrast, the 9–12 years and ≥12 years groups showed a reduction in height z-score up to 12 months, followed by a slight increase at 18 and 24 months. Moreover, according to the regression analysis, the age difference did not predict final height (p>0.05). The weight z-score decreased over time in the <9 years group. Conversely, in the 9–12 years group, the weight z-score increased after 12 months, and in the ≥12 years group, the weight z-score increased from 6 months to 12 months and 18 months to 24 months. The weight z-score in the ≥12 years group was 0.206±1.655 at 24 months, which was higher than the baseline value (-0.034±0.846) (Table 4).

Comparisons of body weight, height, and BMI z-scores in relation to age at which MPH was first used
DISCUSSION
The objective of this study was to investigate the effects of MPH on height and weight in children and adolescents diagnosed with ADHD. In this study, MPH treatment for 24 months, there was an effect on the height, weight, and BMI of children and adolescents with ADHD. First, in terms of the effects on height, after taking MPH, patients with ADHD showed a reduction in the height z-scores at all follow-ups after MPH was initiated. These results are consistent with those of previous studies which showed that extended MPH initially delays height gain. When MPH was used for 18 months in 298 patients with ADHD aged ≤18 years, a significant decline in height z-score was observed [8]. There are several hypotheses on how the height gain pattern changes after the initiation of MPH. First, the release of hepatic growth factors, such as insulin-like growth factor, may be inhibited by the dopaminergic and adrenergic effects of MPH [16]. In addition, MPH may affect bone and cartilage metabolism, thereby slowing the increase in bone and lean tissues [17]. In an in vitro study, MPH inhibited sulfate uptake into cartilage, promoted osteoclast differentiation, activity, and resorption, and reduced bone mineral density and bone mineral content at appendicular sites [18-20]. Finally, MPH may affect growth via negative effects on sleep, which is related to nocturnal growth hormone secretion [21,22]. Conversely, during the long-term use of MPH, it has been suggested that up- and down-regulation of dopamine and other neurotransmitters may ameliorate the growth inhibitory effects of MPH and lead to rebound [16,23-25]. There is a need for continuous studies on the long-term effects of MPH on height gain and the underlying mechanisms.
Second, in the present study, weight z-scores decreased significantly at all time points after the initiation of MPH treatment and did not recover at the final time point of 24 months. The decrease in weight z-scores was most prominent between 6 and 12 months after treatment initiation, after which the trend in reduction was maintained. There are conflicting results regarding the changes in weight caused by MPH. In a study involving central stimulant (CS) use in 410 children and adolescents with ADHD for 0.9–16.1 years, CS was found to cause a relative reduction in weight, and there was a lag of 72 months as compared to the relative baseline values [26]. Conversely, in a study in which 89 children and adolescents with ADHD were followed up for at least 3 years, psychostimulant use significantly changed the weight z-score for 2 years, but there was no significant change afterward [27]. In an analysis using electronic health record data from 3–18-year-old children, stimulants were found to reduce BMI in early- to middle-aged children and were associated with early BMI rebound and obesity [28]. MPH is known to be associated with the regulation of endogenous peptides involved in appetite control, such as ghrelin and leptin. It also delays gastric emptying time, resulting in appetite loss and an anorexic effect [29,30]. However, long-term systematic studies are needed to verify how this anorexic effect influences long-term weight gain.
Third, there were sex differences in the z-scores for weight and BMI at 24 months, while there were no differences between boys and girls in the effect of MPH on growth. This may be due to sex differences in z-scores at the baseline. This finding is similar to that of previous studies [31,32]. In contrast, in a study of 157 ADHD subjects, the weight reduction was greater in girls, and this was thought to be caused by sex-specific differences, such as hormonal differences and behaviors in influencing a reduced food intake [33].
Finally, there were no differences in height gain according to the age of MPH initiation. While the height z-scores continually decreased in the <9 years group, the other age groups showed a rebound in the z-scores after a certain time, although the differences in these changes were not statistically significant. This finding differs from those of previous studies that have reported a greater magnitude of growth inhibition in groups that started taking stimulants at a younger age [34,35]. Further research in this area is required.
This study has some limitations. Since this was a retrospective study that collected data through the subjects’ medical records, there was no double-blinding or any control group. Furthermore, because drug compliance was based on medical interviews or treatment records, there may be some differences in patients’ actual drug usage.
Despite the above limitations, we believe this study is clinically significant because we periodically monitored and analyzed the changes in height and weight gain rates longitudinally over 24 months in children and adolescents with ADHD in South Korea who had not previously taken MPH. Further studies are warranted to determine the extent and mechanisms of the effects of MPH on height and weight development in children and adolescent patients with ADHD. Furthermore, studies on treatment strategies that can minimize MPH’s negative effects on growth are also needed.
In conclusion, the objective of this study is to investigate the effects of 24 months of MPH maintenance on growth in children and adolescents with ADHD (64 males and 18 females; age 6–15 years). We compared height, weight, and BMI z-scores before and after treatment at 6, 12, 18, and 24 months. The height z-scores decreased after initiation of MPH treatment compared with the baseline values, and that decline was slightly decreased at 18 months. The weight z-scores showed a significant reduction at each time point. The changes in height and weight z-scores after MPH treatment showed no differences according to sex or the age of MPH initiation.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Wan Seok Seo. Data curation: Yoojeong Lee, Nayeong Kong, San Koo. Formal analysis: Dai Seg Bai, Hyeonseok Jeong. Funding acquisition: Wan Seok Seo, Hee jin Kim. Investigation: Hee jin Kim. Methodology: Wan Seok Seo, Nayeong Kong. Project administration: Wan Seok Seo. Resources: Hee jin Kim. Software: Wan Seok Seo, Yoojeong Lee. Supervision: Wan Seok Seo. Validation: Wan Seok Seo, Yoojeong Lee. Visualization: Wan Seok Seo, Yoojeong Lee. Writing—original draft: Yoojeong Lee, Nayeong Kong, San Koo. Writing—review & editing: Wan Seok Seo.
Funding Statement
This study was supported by a Yeungnam University Research Grant in 2018.