Increased Risk of Recurrence of Non-Muscle Invasive Bladder Cancer Associated With Psychological Distress: A Prospective Cohort Study
Article information

Abstract
Objective
The primary aim was to evaluate the influence of depressive and anxiety symptoms on the 1-year recurrence rate of non-muscle invasive bladder cancer (NMIBC) patients. The secondary aim was to examine the risk factors leading to psychological distress.
Methods
A total of 104 NMIBC patients were enrolled for interviews, and the Hospital Anxiety and Depression Scale (HADS) questionnaire survey was administered 1 month after their operation. Their cystoscopy results were followed up. The risk factors affecting their 1-year recurrence rate were evaluated through univariate analysis, Cox regression and Kaplan-Meier analysis. The risk factors causing depressive and anxiety symptoms were evaluated through univariate analysis and logistic regression.
Results
In addition to American Urological Association risk stratification, depressive symptoms were another independent risk factor for recurrence in NMIBC patients (HR: 2.493, 95% CI: 1.048–5.930, p=0.039), and the increase in the recurrence rate was highly significant in intermediate-risk patients (HR: 8.496, 95% CI: 2.178–33.138, p=0.019). Anxiety symptoms were not an independent risk factor for recurrence (HR: 1.655, 95% CI: 0.714–3.837, p=0.240). We also observed that the burden of medical expenses of NMIBC on the family was an independent risk factor for depressive symptoms (p=0.029) and anxiety symptoms (p=0.048); chronic pain was an independent risk factor for anxiety symptoms (OR: 3.447, 95% CI: 1.182–10.052, p=0.023).
Conclusion
Depression symptoms are an independent risk factor for recurrence in NMIBC patients. Moreover, the burden of medical expenses on the family is an independent risk factor for depressive and anxiety symptoms in NMIBC patients. Additionally, chronic pain is a risk factor for anxiety symptoms in NMIBC patients. This study provided a theoretical foundation for clinical oncologists to pay more attention to the mental health of NMIBC patients.
INTRODUCTION
Bladder cancer is the 10th most common cancer in the world, accounting for 3% of all malignant tumors. Almost 550,000 people are diagnosed with bladder cancer, and 210,000 people die of bladder cancer every year [1]. Ninety percent of all bladder cancers are urothelial carcinomas pathologically. Among newly diagnosed urothelial carcinoma patients, NMIBC accounts for 70% [2]. NMIBC includes Ta, T1 and Tis stage cancer, which is routinely treated by transurethral resection of bladder tumor (TURBT) with postoperative intravesical treatment. TURBT is the standard choice for NMIBC because of its low trauma and low influence on quality of life. However, NMIBC patients need to undergo a series of invasive examinations and treatments after surgery, including 1) intravesical treatments, such as chemotherapy or BCG; 2) cystoscopy (2–4 times in the first year); 3) re-TURBT as appropriate; and 4) abdominal pelvic imaging as appropriate [3]. It is clear that NMIBC patients need to return to the hospital for reexamination and treatment frequently after TURBT, which may result in mental burden. Moreover, the expense of medical services for NMIBC patients is a problem. In a country where the healthcare system does not cover all medical expenses (such as China), a patient needs to pay partly for repeated TURBT, repeated cystoscopy and biopsy and expensive pharmaceuticals that need to be utilized for years, which may bring a family into an economic crisis. NMIBC patients may have poor mental health, despite the acceptable survival rate due to their mental and economic burden. Two prospective studies have confirmed that the mental health of NMIBC patients is significantly worse than that of the general population using the SF-36 measurement tool [4,5]. Several cross-sectional studies explored the association between bladder cancer and mental health and demonstrated that bladder cancer patients had decreased emotional functioning, social functioning and role functioning and an increased incidence of depressive (78%) and anxiety (71%) symptoms [6]. Meanwhile, bladder cancer patients have a higher suicide rate than other GU malignancy patients [7].
Quite a few studies have been conducted to determine the relationship between depression and anxiety disorders and malignant tumors. An increasing number of studies have indicated that the prevalence of depression and anxiety disorders in cancer patients is significantly higher than that of the general population. Meanwhile, depression and anxiety disorders also lead to an increase in the adverse prognosis of patients with malignant tumors [8,9]. For bladder cancer, it has been confirmed that the diagnosis of a psychiatric disorder results in significantly worse overall survival and cancer specific survival [10]. However, although few bladder cancer patients can reach the criteria of clinical diagnosis of major depressive disorder or anxiety disorder, some of them have various levels of depression or anxiety symptoms, which may also result in a worse prognosis, but there are few relevant studies [11].
Our team proved the association between the growth of bladder cancer and chronic psychological stress in a nude mouse model [12]. Therefore, we designed a prospective investigation based on previous animal experiments to identify the psychological condition of patients and followed up on the prognosis of patients to analyze the impact of depressive and anxiety symptoms on the prognosis of NMIBC patients.
At the same time, we tried to determine the risk factors that promote depressive or anxiety symptoms in NMIBC patients, hoping to identify, screen and intervene in high-risk patients with psychological distress, ultimately improving the prognosis of NMIBC patients.
METHODS
This article is based on data from the medical history system, interviews 1 month after surgery and cystoscopy results 3, 6, 9, and 12 months after TURBT.
Patients
The sample was recruited from patients who underwent TURBT in Huashan Hospital Affiliated with Fudan University between January 1, 2018 and August 31, 2019 with a diagnosis of non-muscle invasive bladder urothelial carcinoma confirmed by pathology. Patients were eligible for study participation if they met the following criteria: 1) 18 years of age or older; 2) able to speak Chinese; 3) denial of a history of other serious somatic disease; 4) denial of a history or a family history of mental disease before the diagnosis of bladder cancer; and 5) Han nationality and living in China.
During the recruitment period of the study, a total of 331 eligible patients were invited to participate, and 104 patients (31.4%) were enrolled, whereas other patients refused to participate in this study.
Eligible patients joined the cohort after consenting to form a consecutive cohort. One month after TURBT, the patients were asked to return to the hospital to participate in an interview and to complete the HADS questionnaire. All patients underwent regular cystoscopy at 3, 6, 9, and 12 months after TURBT. Additionally, all patients indicated their willingness to participate in the study and gave written informed consent. The study was approved by the relevant ethics committees (IRB approval number: KY2020-1112).
Measures
We obtained the following information from the medical history system: patient age, gender, medical insurance type, initial tumor or recurrent tumor, cancer stage, histopathological grade, size of tumor, multiplicity and whether the tumor occurred with carcinoma in situ (CIS).
We obtained the following information from the interview 1 month after the surgery: patients’ marital status, education level, chronic pain, how much they knew about the disease, support from their family, burden of medical expenses of NMIBC on the family and symptoms before their surgery (including hematuria, bladder irritation and dysuria).
We obtained depressive and anxiety symptoms from the paper-pencil version of the HADS questionnaire during the interview. Zhiyu Qian and Qidong Zhou were responsible for the interview and questionnaire.
We determined whether and when the tumor reoccurred from the results of regular cystoscopy.
“Age” was defined as the age at the time of surgery. “Medical insurance type” was divided into urban medical insurance, rural medical insurance, other medical insurance (including commercial insurance) and self-paying. “Marital status” was divided into unmarried, married, divorced and widowed. “Education level” was divided into primary school, secondary school, junior college and undergraduate or above.
As we also aimed to explore which factors affect the occurrence of depressive and anxiety symptoms, in our interviews, we collected the following information: “chronic pain” [13-15], “support from the family” [16,17] and “burden of medical expenses on the family” [18], which have been found to be related to depression and anxiety in previous studies. In addition, given that the diagnosis of malignant tumors is often concealed from elderly individuals in China, we also added the question “how much do you know about your disease?” to the interview to determine the relationship between awareness and psychological symptoms. “Chronic pain” was defined as yes or no; “support from the family” was defined as good, intermediate or bad; “burden of medical expenses on the family” was defined as heavy, intermediate or light; “how much do you know about your disease?” was defined as understanding, intermediate or not understanding.
The disease was evaluated according to the clinical stage criteria recommended by the AUA Risk Stratification for NMIBC [3]: “histopathological grade” was defined as G1, G2, and G3 according to the WHO 1973 criterion; “cancer stage” was defined as Ta and T1 according to the TNM classification system; “size of tumor” was defined as <3 cm and ≥3 cm; “multiplicity” was defined as 1, 2–7 and >7; “CIS” was defined as tumor with CIS or without CIS.
Evaluation of depressive and anxiety symptoms
The depressive and anxiety symptoms of the patients were assessed by the Hospital Anxiety and Depression Scale (HADS), which included two subscales: anxiety (HADS-A) and depression (HADS-D). There are 7 questions on each subscale, 0–3 points for each question, and a total score of 0–21 points separately. The higher the score is, the more significant the anxiety or depressive symptoms are [19]. The HADS is one of the most widely used depressive and anxiety symptom scales, and there is a mature and reliable Chinese version [20]. Although there is no consensus on the interpretation of the HADS score [21], it is generally considered that “≥8” as the presence of depressive and anxiety symptoms is the best threshold for both sensitivity and specificity [22].
Outcome
We followed the results of regular cystoscopy of the patients 12 months after the operation. All patients were given intravesical chemotherapy according to the guidelines. The outcome of other patients was defined as “recurrence” or “no recurrence”. All “recurrence” patients were confirmed by pathology. All “no recurrence” patients were confirmed by cystoscopy after surgery. Recurrence-free survival was defined as the interval between the day of surgery and recurrence.
Data entry
Two fixed personnel were responsible for data entry. The data are from the results of interviews and the HADS questionnaire of patients and the medical history system. The data entry software used was “epidata.”
Statistical analysis
“SPSS” was used to compute all statistics. Our statistical analysis included the following three aspects: which factors were related to the recurrence of NMIBC patients, which factors were related to depressive symptoms, and which factors were related to anxiety symptoms. In each aspect, univariate analysis was used to determine the variables significantly related to the dependent variable, and then these variables were included in multiple regression analysis (including Cox regression, Kaplan-Meier survival analysis and logistic regression) to determine the independent influencing factors. The confidence interval was 95%.
RESULTS
Patients’ information
Table 1 shows the information for the NMIBC patients. In total, 104 patients were enrolled in the study. One patient died of another disease 6 months after the operation, which was defined as loss to follow-up. The other 103 patients were followed up to 12 months after their operation. Seventy-six of them lived without recurrence, whereas 27 patients’ tumors reappeared. Then, we calculated the recurrence rate of NMIBC patients by Kaplan-Meier survival analysis: the 1-year recurrence-free survival rate of the 103 patients was 73.9% (Figure 1).

Sociodemographic and clinical characteristics and clinical anxiety and depressive symptoms of the samples
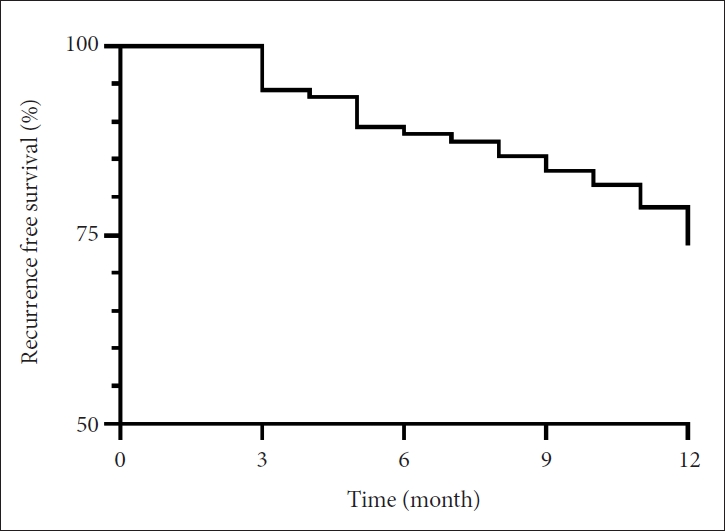
The 1-year recurrence-free survival of 103 patients by Kaplan-Meier analysis.
Meanwhile, the prevalence of depressive and anxiety symptoms of the 104 patients was calculated: 33% of the NMIBC patients had depressive symptoms, and 28% of them had anxiety symptoms.
Univariate analysis, cox regression and Kaplan-Meier analysis of recurrence of NMIBC
We included personal information, clinical information and depressive and anxiety symptoms in univariate analyses to observe whether the variables were related to recurrence.
In Table 2, among the several items in the AUA risk stratification, “initial tumor or recurrent tumor,” “histopathological grade,” and “cancer stage” were significantly related to the recurrence rate of the patient. Among the other variables, preoperative bladder irritation and depressive and anxiety symptoms were also significantly related to recurrence.

Univariate analysis of variables and recurrence
Therefore, we included AUA risk stratification, bladder irritation and depressive and anxiety symptoms in the Cox regression (Table 3). The results showed that a higher risk grade of AUA (p=0.026) and depressive symptoms (HR: 2.493, 95% CI: 1.048–5.930, p=0.039) were independent risk factors for recurrence. That is, the recurrence risk of NMIBC patients with depressive symptoms was 2.49 times higher than that of patients without depressive symptoms.

Cox regression of variables and recurrence
In addition, we analyzed the relationship between recurrence-free survival and AUA risk stratification (Figure 2) and between recurrence-free survival and depressive symptoms (Figure 3).

Association between recurrence-free survival and AUA risk stratification. AUA: American Urological Association.
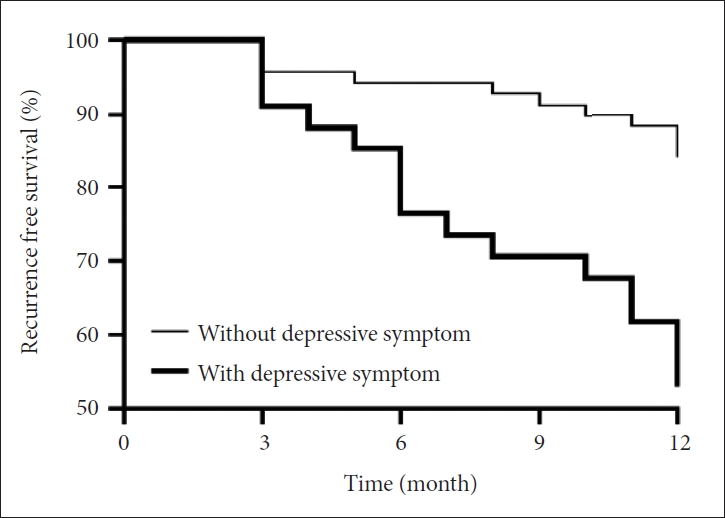
Association between recurrence-free survival and depressive symptoms.
After that, we divided the patients into three groups according to the AUA risk stratification. Subgroup survival analysis based on depressive symptoms was performed (Figure 4), indicating that the recurrence of intermediate-risk patients was worsened the most by depressive symptoms. The HR of depressive symptoms in the intermediate-risk group was 8.496 (95% CI: 2.178–33.138, p=0.019).
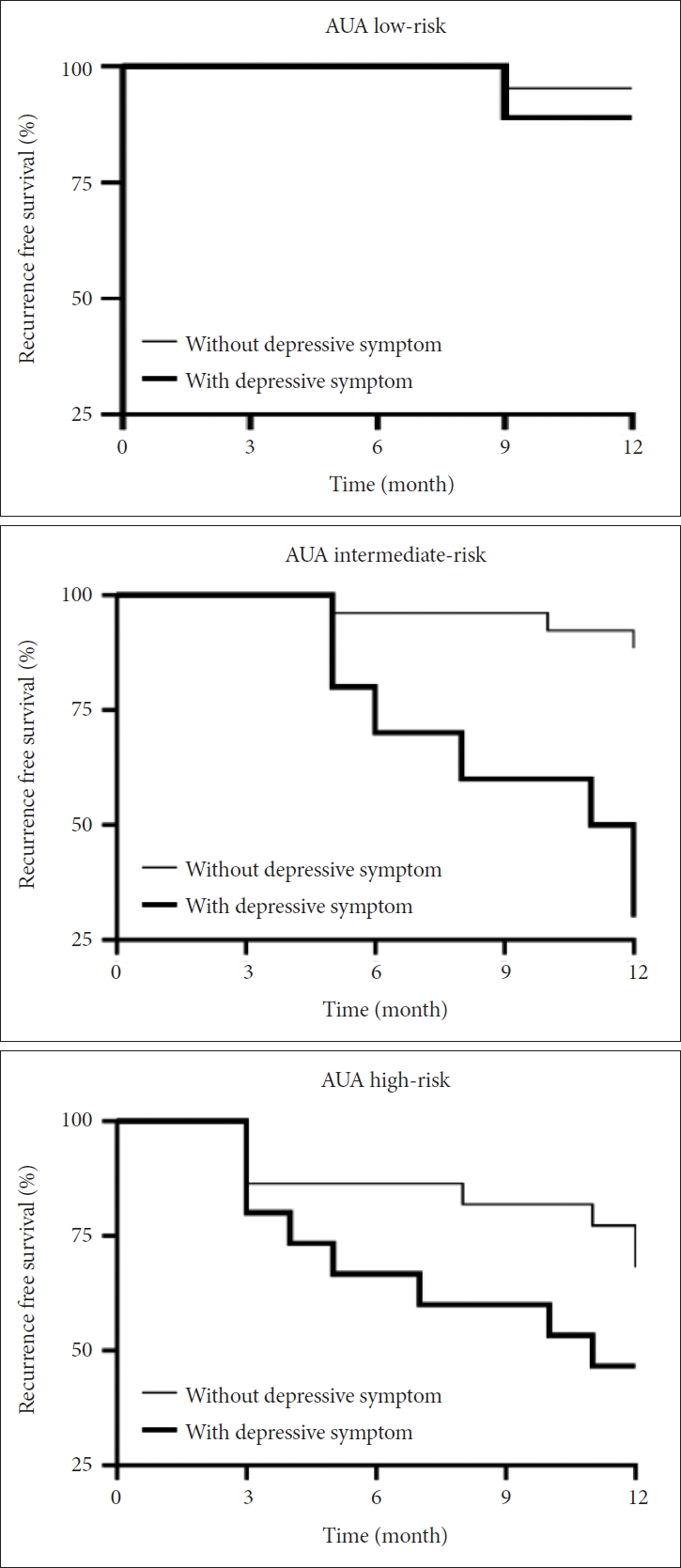
Survival analysis of low-risk, intermediate-risk, and high-risk NMIBC patients. NMIBC: non-muscle invasive bladder cancer, AUA: American Urological Association.
Univariate analysis and logistic regression of depressive and anxiety symptoms
To identify which factors may be associated with depressive and anxiety symptoms, variables were included in the univariate analyses and logistic regression of depressive or anxiety symptoms.
In Table 4, “Less understanding of the disease,” “heavier burden of medical expenses on the family,” “later cancer stage,” and “having bladder irritation before operation” were significantly correlated with having depressive symptoms. After putting the above variables into logistic regression, we found that a “heavier burden of medical expenses on the family” (p=0.029) was an independent risk factor for depressive symptoms (Table 5).

Univariate analysis of depressive symptoms

Logistic regression of depressive symptoms
Univariate analyses of anxiety symptoms were also performed.
In Table 6, “Less understanding of the disease,” “heavier burden of medical expenses on the family,” “chronic pain,” and “having bladder irritation before operation” were significantly correlated with anxiety symptoms. After putting the above variables into logistic regression, we found that “heavier burden of medical expenses on the family” (p=0.048) and “chronic pain” (OR: 3.447, 95% CI: 1.182–10.052, p=0.023) were independent risk factors for anxiety symptoms (Table 7).

Univariate analyses of anxiety symptoms

Logistic regression of anxiety symptoms
DISCUSSION
This current study prospectively examined the role of depression on recurrence in NMIBC patients. The results demonstrated that depressive symptoms are an independent risk factor for an increased 1-year recurrence rate in NMIBC patients. Despite the short follow-up period (12 months), the high recurrence rate of NMIBC showed a clear association between depressive symptoms and the recurrence rate. In addition, we found that the increase in the recurrence rate caused by depressive symptoms was particularly significant in the intermediate-risk group, which led to the recurrence rate of intermediate-risk patients with depressive symptoms being similar to that of the high-risk group.
Meanwhile, this study also explored the prevalence of depressive and anxiety symptoms in patients with bladder cancer and its risk factors. In our NMIBC patients, 28% had anxiety symptoms, and 33% had depressive symptoms. The prevalence was obviously higher than that of normal people in China [23], indicating that NMIBC brings additional psychological distress to patients. Among many individual and disease variables, the burden of medical expenses on the family is an independent risk factor for both depressive and anxiety symptoms, and chronic pain is an independent risk factor for anxiety symptoms. The findings can provide help for the detection of NMIBC patients with depressive or anxiety symptoms.
Regarding the mechanism of how depression affects the prognosis of cancer patients, the current mainstream views include directly affecting physiological function and influencing behavioral mode.
According to classical theory, at the cellular level of a patient with depression, the number of NK cells, proportion of T cells, proportion of CD8+ T cells, proliferation ability of lymphocytes, phagocytosis of neutrophils, function of T cells and NK cells and activity of monocytes are decreased [24-26]. At the molecular level, the basal cortisol of patients with depression is increased, and the HPA axis is disordered, leading to immune dysfunction [22,23].
Depression can also affect the prognosis of cancer patients in terms of lifestyle. Patients with depressive symptoms tend to have unfavorable lifestyles (e.g., more smoking [27], more energy intake [28], lack of vitamins [29], and lack of exercise [30]), inferior sleep quality and poor treatment compliance [31].
Immune function plays an important role in the recurrence of bladder cancer [32]. Poor lifestyle (especially smoking, obesity and lack of exercise) is a direct risk factor for bladder cancer [33]. These factors may jointly result in an increased recurrence rate of NMIBC patients with depressive symptoms.
Psychological therapy is an effective treatment for depression in cancer patients and should be considered for NMIBC patients with depressive symptoms [34,35], whereas there is no strong evidence on the effect of pharmaceutical therapy on depression in cancer patients [36]. Clinicians can identify high-risk patients with depressive symptoms with the abovementioned high-risk factor (burden of medical expenses of NMIBC on the family) and screen them. Then, psychological intervention can be utilized on the diagnosed cases to prevent them from a poorer quality of life and prognosis. Although we did not find that anxiety symptoms are an independent risk factor for recurrence, anxiety symptoms can also affect the quality of life of patients, so patients with high risk factors for anxiety can also be screened and receive intervention as appropriate.
This study has many advantages. First, it is a prospective study that is more compelling. In addition, all the patients underwent TURBT and cystoscopy in the same hospital, so their hospitalization environment, medical service level and cost of disease were similar, which could have balanced some confounding factors. Meanwhile, our patients did not receive psychotherapy or pharmacotherapy within 12 months after the first TURBT, so this study can better reflect the impact of untreated depressive or anxiety symptoms.
Second, there are few studies on the relationship between the recurrence rate of NMIBC patients and psychological symptoms, not to mention how to identify such patients clinically. A large amount of research has focused on the role of psychological factors in the prognosis of cancer, but researchers have tended to focus on the association between psychological disorders and the survival rate but not the recurrence rate. This may be because in many malignant tumors, recurrence often indicates that the patient is difficult to cure, which can be reflected in the survival period. However, the recurrence rate of NMIBC patients is high, whereas the mortality rate is relatively low; therefore, this study mainly focused on recurrence, which may be more meaningful.
Third, there were few patients whose mental symptoms were serious enough to be diagnosed with major depressive disorder or anxiety disorder. These disorders may be so serious that their adverse effect on patient outcomes is irreversible, and it is also much more difficult to cure their mental disease. Our research was aimed at patients with depressive or anxiety symptoms. It is more common to see such patients, and their psychological symptoms are relatively less serious. Depressive or anxiety symptoms may affect their quality of life and prognosis, but they are easier to treat comparatively, so they are of more clinical significance.
There are also a few limitations in this study. First, our sample size at present is small, and it is a single-center study. Therefore, the association between depressive symptoms and recurrence of NMIBC found in our study is preliminary, and so is the conclusion that the influence of depressive symptoms on the recurrence rate is most significant in the AUA intermediate-risk group. We hope to expand it into a multicenter large sample study to increase the persuasiveness of the conclusion.
Second, the patients in the study were volunteers. Only 31.4% of the eligible patients chose to participate, which might have caused selection bias: patients in extreme pain may be less likely than others to volunteer for the study. If this is the case, this study might have underestimated the overall depressive and anxiety symptoms of NMIBC patients, so the results may only be applicable to those who voluntarily join a psychological oncology study.
In conclusion, we found that NMIBC patients’ depressive symptoms, in addition to AUA risk stratification, were an independent risk factor for the 1-year recurrence rate. Meanwhile, we found that the increase in the recurrence rate caused by depressive symptoms was most significant in the intermediate-risk group. The intermediate-risk NMIBC patients had a similar recurrence rate to the high-risk group because of psychological distress, which suggests that we may consider adopting the strategy of postoperative examination and treatment of the high-risk group. Personal information for these patients was also collected to identify the variables that may influence their depressive and anxiety symptoms, and we found that the “burden of medical expenses on the family” was an independent risk factor for depressive symptoms. The effectiveness of psychological interventions on psychological distress is clear. Therefore, we suggest that clinicians pay close attention to the mental health of patients with NMIBC in their work. Patients can be regarded as a high-risk population with depressive or anxiety symptoms if they have the above risk factors, which can help to identify and screen them earlier and apply proper treatment in time to avoid an undesirable prognosis. We also suggest that a superior and interhospital medical history system should be established in China, which not only helps to carry out multicenter large sample research but also helps doctors obtain patients’ information more conveniently, identify patients with high-risk factors for depression and anxiety and provide screening, consultation and treatment for patients with psychological distress.
Depressive symptoms are an independent risk factor for recurrence in NMIBC patients. A heavier burden of medical expenses on the family is an independent risk factor for both depressive and anxiety symptoms in NMIBC patients. Additionally, chronic pain is a risk factor for anxiety symptoms in NMIBC patients. This study provided a theoretical foundation for clinical oncologists to pay more attention to the mental health of NMIBC patients.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are not publicly available due [REASON(S) WHY DATA ARE NOT PUBLIC] but are available from the corresponding author on reasonable request.
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Chuanyu Sun, Ke Xu. Formal analysis: Zhiyu Qian. Investigation: Zhiyu Qian, Qidong Zhou. Project administration: Weihong Ding. Resources: Weihong Ding. Software: Shengyang Ge. Supervision: Ke Xu. Visualization: Qidong Zhou. Writing: Zhiyu Qian.
Funding Statement
This study is funded by the Science and Technology Commission of Shanghai Municipality (grant no. 19ZR1408000).