Psychopathologic Profiles and Clusters in Tertiary Clinic Referred Patients with Adult Attention Deficit Hyperactivity Disorder: A Person-Centered Analysis
Article information

Abstract
Objective
Adult attention deficit hyperactivity disorder (ADHD) has a heterogeneous clinical presentation with patients showing very frequent emotional problems. In the present study, patients with adult ADHD were subtyped based on their psychopathology using a person-centered approach.
Methods
In the present chart review study, detailed findings of psychological evaluation conducted as part of routine care were utilized. A total of 77 subjects with adult ADHD were included in the analysis. Detailed ADHD symptoms, psychiatric comorbid Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnoses, and severity of mood and anxiety symptoms were evaluated in the person-centered analysis.
Results
Three clusters were generated using clustering analysis. DSM comorbid conditions did not significantly impact the clustering. Cluster 1 consisted of ADHD combined presentation (ADHD-C) with less mood symptoms, cluster 2 of ADHD predominantly inattentive presentation and cluster 3 of ADHD-C with significant mood symptoms. Patients in cluster 3 had adulthood functional impairment more frequently compared with patients in cluster 1. Patients in cluster 3 showed recurrent thoughts of death and suicidal ideation more frequently compared with patients in cluster 1.
Conclusion
Further studies are needed to confirm the relationships observed in the present study.
INTRODUCTION
Adult attention deficit hyperactivity disorder (ADHD) is common but remains an under-recognized mental illness [1]. In recent studies, the reported rate of adults who have persistent ADHD symptoms from childhood ranged from 15–80%, depending on the definition used for symptom persistence [2,3]. In a population study, the estimated prevalence of ADHD in adults ranged from 2.5–3.4% [4]. However, few patients with adult ADHD receive proper treatment [5]. Many patients do not visit clinics for treatment and the vast majority of patients are treated for other psychiatric conditions [6]. Undertreated ADHD is associated with poorer performance at work, poorer quality of life, worse interpersonal/marital relationships, and increased suicide risk [7,8]. Adult ADHD is considered a heterogeneous condition with frequent comorbid psychiatric conditions [9]. In particular, the vast majority of patients with adult ADHD have co-occurring emotional problems. Although not listed in DSM criteria for adult ADHD, in previous studies, approximately 27–58% of patients with adult ADHD had co-existing anxiety and mood disorders [6,10,11]. Subthreshold mood and anxiety symptoms are also very common [12]. Co-existing mood symptoms worsen patient clinical courses and psychosocial outcomes [13]. Mood dysregulation, which is considered a core feature of various mood and anxiety disorders, is also very common in patients with ADHD [14].
However, whether emotional problems are a core feature of adult ADHD remains controversial. In the Diagnostic and Statistical Manual of Mental Disorders-fifth edition (DSM-5), the diagnosis of adult ADHD includes only inattention, hyperactivity, and impulsivity, whereas emotional dysregulation is listed as a characteristic feature of ADHD, supporting the diagnosis [15]. However, emotional dysregulation has consistently been shown a core feature of ADHD in recent studies [16,17].
To determine the classification of adult ADHD when considering the emotional problem as a core feature, we aimed to conduct person-centered analysis of psychopathology of patients with adult ADHD. We hypothesized the adult ADHD population will be separated in several clusters depending on emotional symptoms and ADHD symptom pattern. We also compared suicide risk among clusters. Considering emotional symptoms are closely related to suicide risk, we hypothesized that suicide risk could differ by severity of emotional symptoms.
METHODS
Study population
Data were obtained from retrospective chart review of patients who visited the outpatient clinic of Samsung Medical Center between January 1, 2018 and December 31, 2019. As part of routine care, all patients who visited the outpatient clinic of the Department of Psychiatry at Samsung Medical Center underwent a standardized evaluation process to confirm their DSM diagnosis and symptom severity. After an initial interview with a board-certified psychiatrist, patients between 18 and 65 years of age were referred to a psychologist for a comprehensive psychological evaluation. Patients suspected of psychosis or intellectual disability or those who required emergency admission were not referred for the evaluation. The psychological evaluation was designed to confirm the clinical diagnosis of subjects based on the DSM-IV-TR and evaluate symptom severity. The psychologist who conducted the evaluation had more than 2 years of clinical experience. The test results of the comprehensive psychological evaluations were analyzed. A total of 77 subjects completed the evaluations.
The study protocol was approved by the Institutional Review Board of Samsung Medical Center (IRB no. 2018-11-019). The study was performed in accordance with the ethical standards stated in the 1964 Declaration of Helsinki. All identifying data were removed from the clinical database prior to analyses. Patient consent was waived because this was a retrospective chart review study.
Applied measures
Psychiatric diagnoses
The diagnoses of subject were evaluated using the Korean version of the Mini International Neuropsychiatric Interview’s (MINI) [18] during the psychological evaluation. Comorbid psychiatric conditions based on DSM diagnoses were included for the analysis.
Lifetime ADHD symptoms
The MINI requires individuals to meet 6 of 10 criteria in childhood before the age of 7 years, and 9 of 14 criteria during adulthood. Of the 10 criteria in childhood, 5 items assess hyperactivity symptoms, 4 items inattention symptoms, and 1 item functional impairment during childhood. Of the 14 items in adulthood, 5 items assess hyperactivity symptoms, 3 items inattention symptoms, and 6 items functional impairment during adulthood. The number of items positively answered in each domain was used in the analyses.
Emotional symptoms
The Hamilton Depression Rating Scale (HAM-D; Hamilton, 1967) and Beck Depression Inventory II (BDI-II) were used to evaluate current depressive symptoms in subjects. The Hamilton Anxiety Rating Scale (HAM-A) [19]; and the Beck’s Anxiety Inventory (BAI) [20]; were used to evaluate anxiety symptoms. The Anxiety Sensitivity Index-3 (ASI-3) [21]; was used to evaluate anxiety sensitivity. The ASI-3 consists of 3 subscales (physical, cognitive, and social concern) [22]. The Albany Panic and Phobia Questionnaire (APPQ) [23]; was used to assess fear of situations and activities that are commonly avoided by individuals with agoraphobia and social anxiety disorder. The APPQ consists of 3 subscales: agoraphobia, social phobia, and interoceptive fear [24]. The Penn State Worry Questionnaire (PSWQ) [25]; was used to evaluate severity of worry. Obsessive Compulsive Inventory-Revised (OCI-R) [26]; was used to evaluate obsessive compulsive symptoms. The Mood Disorder Questionnaire (MDQ) [27]; and the Hypomania Symptom Checklist-32 (HCL-32) [28]; were used to evaluate the subthreshold hypomania.
Suicidality
Suicidality was measured using the MINI suicide-item modules and the HAMD suicide-item scores. The MINI suicide module is a 6-question, yes-or-no interviewer-administered questionnaire used to evaluate suicidality and current risk of suicide. The MINI suicide module assesses experiences of recurrent thoughts of death, idea of self-harm, presence of suicide ideation, plans and (current and past) attempts. The single score is generated after summing weighted scores. Suicide risk score is categorized as low risk (<9), medium risk (9–16), or high risk (≥17) of future suicide attempts [29].
Statistical analyses
Prior to the person-centered analysis, variables were clustered using factor analysis for dimension reduction. Mood and anxiety symptoms were clustered into 2 factors: factor 1 comprised depressive and anxiety symptoms (measured using ASI-3, APPQ, BDI-II, BHS, BAI, PSWQ, LSAS, and OCIR scores), and factor 2 comprised lifetime hypomanic symptoms (measured using MDQ and HCL-32) (Supplementary Table 1 in the online-only Data Supplement). DSM comorbid diagnoses were also clustered into 2 factors (Supplementary Table 2 in the online-only Data Supplement): factor 1 comprised comorbid anxiety disorder and absence of alcohol use disorders. Lifetime ADHD symptoms were entered into person-centered analysis after clustering into childhood 1) inattention, 2) hyperactivity, and 3) functional impairment symptoms and adulthood 1) inattention, 2) hyperactivity, and 3) functional impairment symptoms.
To determine the distinct subtypes of adult ADHD, clustering analysis was performed with 12 psychological variables including 2 factors for mood and anxiety symptoms, 2 factors for DSM comorbid diagnosis, 6 lifetime ADHD symptoms, HAM-A, and HAM-D scores. Model solutions were determined based on the Cubic Clustering Criterion (CCC) and R squared. CCC is a commonly used and reliable method for model fit determination with higher CCC values representing better fit [30]. We considered numbers of clusters between two to five due to small sample sizes, and chose the best model with the local peak of CCC. Higher probability value indicates more accurate classification. Comparisons between classes were conducted using ANOVA or Kruskal-Wallis test for continuous variables and χ2 tests or Fisher’s exact test for categorical variables. Analyses were performed using the SAS version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Based on the cubic clustering criterion value, 3 clusters were identified (Table 1). Among variables entered in the analysis, DSM diagnoses did not significantly contribute to cluster formation. Cluster 1 comprised 38% of patients (n=29) and who had ADHD combined type with less emotional symptoms. Cluster 2 comprised 13% of patients (n=10) with ADHD inattentive dominant type. Cluster 3 comprised 50% of all patients (n=38) who had ADHD combined type with severe emotional symptoms. Age and sex were not significantly different among the 3 clusters. Subjects with ADHD combined type in adulthood had ADHD combined type in childhood, and subjects with ADHD inattentive type in adulthood had ADHD inattentive type in childhood.

Best fit model determining indices for two, three, four, and five class clustering model identifying subtypes of adult ADHD (N=77)
Significant difference was observed in the area of functional impairment among clusters (Figure 1). Patients in cluster 3 had adulthood functional impairment more frequently than patients in cluster 1 (post-hoc p=0.001). Patients in cluster 3 showed a significantly greater number of childhood functional impairments than patients in cluster 2 (post-hoc p=0.002).
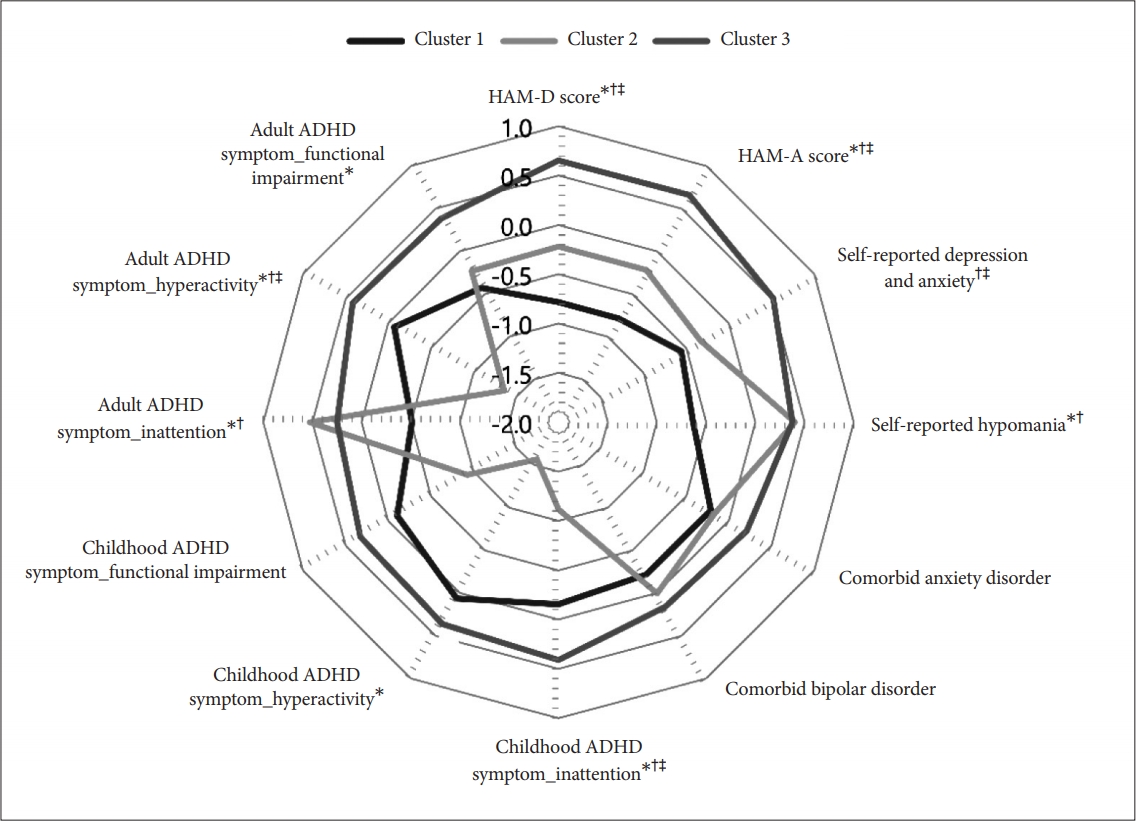
Comparison of factor scores among groups. *Post hoc analysis: 1 vs. 2 <0.05, †1 vs. 3 <0.05, ‡2 vs. 3 <0.05. ADHD: attention deficit hyperactivity disorder, HAM-D: Hamilton Depression Rating Scale, HAM-A: Hamilton Anxiety Rating Scale.
Figure 1 shows comparisons of factor score of each domain among clusters. As stated above, patients in cluster 1 had more severe emotional symptoms with greater ADHD combined type symptoms. Patients in cluster 2 had prominent lifetime hypomanic symptoms and ADHD inattentive symptom. Patients in cluster 3 had less emotional symptoms and ADHD combined type symptoms than patients in clusters 1 and 2.
Significant difference was not observed among sociodemographic cluster characteristics (Table 2). Patients in cluster 3 had greater depressive and anxiety symptoms across all measurements compared with patients in cluster 1 (post-hoc p<0.001) (Table 3). Patients in cluster 2 also had greater HAMD, HAMA, ASI social subscale score, APPQ social subscale score, APPQ total score, BDI-II, BHS, and LSAS scores compared with patients in cluster 1. Patients in cluster 2 did not show significant differences in ASI social, APPQ social score, APPQ total score, BHS, and LSAS scores compared with patients in cluster 3. In other measurements, patients in cluster 3 showed greater symptom severity compared with patients in cluster 2. Regarding lifetime hypomanic symptoms, patients in cluster 3 had greater MDQ and HCL-32 scores compared with patients in cluster 2. Significant difference was not observed between cluster 1 and cluster 3.

Sociodemographic characteristics of participants

Comparisons of depressive and anxiety symptom severity among clusters
Regarding DSM comorbid diagnoses, patients in cluster 3 had major depressive disorder and anxiety disorder more frequently than patients in the other clusters. Patients in cluster 1 also had greater HCL-32 score than patients in cluster 2 (Table 4). Among patients included in our study, only 11 (14.3%) did not have any DSM comorbid conditions. Notably, all patients in cluster 3 had at least one DSM comorbid condition. Anxiety disorder (n=33) was the most common DSM comorbid condition, followed by major depressive disorder (n=24), bipolar disorder (n=20), and alcohol use disorder (n=14). Among anxiety disorders, generalized anxiety disorder (n=20) was the most common, followed by social phobia (n=14) and panic disorder (n=5) (Supplementary Table 3 in the online-only Data Supplement). In post-hoc analysis, patients in cluster 3 had major depressive disorder more frequently than patients in cluster 1 (13.8% vs. 44.7%, post-hoc p=0.024).

Comorbid DSM diagnoses of clusters generated using person-centered analysis
Regarding suicide risk evaluation, patients in cluster 3 had recurrent thoughts of death and suicidal ideation more frequently than patients in other clusters (Table 5). No significant difference was observed in MINI suicide scores between clusters.

Comparisons of suicide risk evaluated using MINI suicide module among clusters
DISCUSSION
In the present study, we aimed to subtype adult ADHD population using person-centered analysis. Three clusters were identified; adult ADHD inattentive type independently existed, and ADHD combined type was subdivided into 2 groups depending on presence of mood symptoms. The presence of emotional symptoms in ADHD combined type were associated with greater functional impairment and more frequent suicidal ideation.
The results of the present study need to be interpreted within the context of the study design. Because the study included patients referred to a tertiary hospital, bias in terms of symptom severity could have occurred. In the present study, ADHD hyperactivity subtype was not detected and the majority of patients were ADHD combined type. In addition, all patients included in the study had a history of childhood ADHD. In previous studies in which developmental trajectories of ADHD symptoms were evaluated, hyperactivity symptoms reportedly decreased with time [31,32]. In a recent epidemiological study, most subjects with adult ADHD did not show any childhood ADHD symptoms [33,34]. Contradictory findings from the present study are likely due to the recruitment setting. However, similar results to the present study were reported in a study conducted using a similar clinical setting [35].
Emotional symptoms were quite frequent across the 3 clusters in the present study. In particular, ADHD hyperactivity type was divided into 2 clusters depending on severity of emotional symptoms. Patients in cluster 3 had greater emotional symptoms compared with patients in other clusters. In a prior study by Hirsch and colleagues [36] using person-centered analysis, 2 clusters were identified in patients with ADHD based on severity of negative mood and elevated psychological distress. Clusters with greater depressive symptoms mainly included combined type ADHD, which corroborates the findings in the present study [36]. Patients in cluster 3 also had frequent functional impairment both in childhood and adulthood. In addition, all subjects in cluster 3 had at least one DSM comorbid condition. In prior studies, high psychiatric comorbidity and severe functional impairment were reportedly associated with persistent hyperactivity [34,37]. Childhood hyperactivity is associated with adverse experiences including social refusal and isolation, which eventually affects personality, rendering an individual vulnerable to depression [38,39]. In a previous longitudinal study, the ADHD combined type and inattentive type predicted depression in adolescence compared with the ADHD hyperactivity type. In addition, the ADHD combined type and hyperactivity type was a predictor for suicide attempts compared with the inattentive type [40]. Therefore, emotional symptoms in ADHD might arise from hyperactivity symptoms.
However, patients in cluster 3, which was mainly composed of ADHD combined type, generally showed little emotional symptoms except self-reported hypomania symptoms compared with patients in other clusters. Considering self-reported hypomania symptoms are often associated with ADHD even in patients who do not experience true hypomanic symptoms [41,42], cluster 3 might include subjects who mainly experience pure ADHD symptoms. Patients in cluster 3 also showed less severe suicidality than patients in cluster 1. The association between ADHD and suicide has been consistently reported [43,44]. In previous studies, high impulsivity and emotional instability were postulated to mediate the association [45,46]. In a systematic review, the psychiatric comorbid conditions were suggested to possibly mediate the association, which is in agreement with the findings in the present study. Thus, emotional disturbance in ADHD needs to be thoroughly evaluated in adult ADHD subjects to prevent suicide.
Due to the limited sample size in the present study, whether ADHD inattention type only forms one cluster is difficult to conclude. Patients in cluster 2 had less severe emotional symptoms and less suicidality than patients in other groups. In prior studies, less suicide risk in ADHD inattention type compared with ADHD combined/hyperactivity type was suggested [47].
Notably, patients in cluster 2 generally showed high social anxiety compared with patients in cluster 1, which is consistent with results from previous studies showing ADHD inattentive type is associated with social anxiety disorder [48,49]. In the reports on peer relationship of ADHD, ADHD inattentive type showed passive social participation and avoidance, and ADHD combined types showed defiant and aggressive behaviors [50]. In addition, anxiety was reported to play a mediating role between ADHD symptoms and functional impairment in a previous study of adult ADHD [51].
Shaw et al. [52] suggested 3 different models that explain the relationship between ADHD and emotional problems. In the first model, emotional problems are postulated as a core symptom of ADHD that shares the same neurocognitive deficit with ADHD symptoms. In the second model, emotional problems and ADHD are correlated but located within distinct dimensions. In the third model, co-existing ADHD and emotional problems exist as a separate disease entity. Because emotion dysregulation was not directly assessed in the present study, the hypothesis suggested above cannot be directly examined in the context of our findings. However, the emotional symptoms based on ADHD symptomatology were observed as distinct differences among clusters, and the degree of emotional symptoms was different between clusters with the same symptomatology (cluster 1 vs. cluster 3) in the present study, indicating emotional problems and ADHD are correlated but located within distinct dimensions. Further studies in which the emotional dysregulation in ADHD is directly examined are needed to confirm the results of the present study.
Several limitations should be considered when interpreting the present study results. First, the sample size may be insufficient for subtyping. Second, all participants were recruited from a single tertiary care center, limiting generalizability. In particular, as stated above, the study population had more ADHD combined type, which is contrary to findings in prior studies. Third, cross-sectional evaluation was conducted. Fourth, recall bias can impact lifetime ADHD symptom evaluation. Fifth, executive function was not evaluated.
Despite the limitations, the clinical subtypes of adult ADHD were determined in the present study using person-centered analysis. Adult ADHD was subdivided into 3 groups based on depressive and anxiety symptoms and lifetime ADHD symptom presentation. ADHD combined type was divided into 2 groups based on the presence of mood symptoms, which showed associations with greater functional impairments and experience of suicide idea. ADHD inattentive type comprised a separate group that was characterized by high social anxiety and less emotional symptoms. Further studies are needed to determine the validity of subtypes generated in the present study.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.30773/pi.2020.0331.
Acknowledgements
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2019R1G1A 1091679).
Notes
The authors have no potential conflicts of interest to disclose.
Authors’ contribution
Conceptualization: Yunhye Oh, Ji Hyun Baek. Data curation: Yunhye Oh, Hyewon Park, Ji Hyun Baek. Formal analysis: Yunhye Oh, Seonwoo Kim, Hye Seung Kim, Ji Hyun Baek. Funding acquisition: Ji Hyun Baek. Investigation: Yunhye Oh, Ji Hyun Baek. Supervision: Yoo-Sook Joung, Kyung Sue Hong. Writing—original draft: Yunhye Oh, Yoo-Sook Joung, Kyung Sue Hong, Ji Hyun Baek. Writing—review & editing: Yunhye Oh, Ji Hyun Baek.