Association between Dialysis Adequacy and Cognition in Patients with Peritoneal Dialysis
Article information

Abstract
Objective
Cognition of peritoneal dialysis patients is influenced by various factors including dialysis adequacy such as fractional urea clearance (Kt/V) and relative overhydration (RelOH). This study aimed to discover the potential contribution of dialysis adequacy to cognitive function in patients undergoing peritoneal dialysis.
Methods
Fifty-nine patients undergoing peritoneal dialysis were recruited. Demographic information, comorbidities, and clinical lab findings were retrospectively collected, and dialysis adequacy was determined by the Kt/V and RelOH calculation. Cognition and depression were measured with Digit Symbol Substitution Test, Hopkins Verbal Learning Test, Wechsler memory scale (spatial span), Wisconsin Card Sorting Test, and Beck’s depression inventory. Partial correlation test was used to explore the correlation of dialysis adequacy with cognitive function.
Results
RelOH showed significant correlation with some of the Wisconsin Card Sorting test results. The categories achieved showed negative correlation (r=-0.32, p=0.02) and trials to complete first category showed positive correlation (r=0.31, p=0.02) with RelOH. Other tasks showed no significant correlation with RelOH. Kt/V.
Conclusion
Our study demonstrates that peritoneal dialysis adequacy, measured by RelOH, seems to be significantly correlated with the occurrence of cognitive impairment. The outcome suggests that RelOH may have the potential to clarify the role of cognitive impairment in peritoneal dialysis patients.
INTRODUCTION
Patients with end-stage renal failure undergoing peritoneal dialysis (PD) have various psychiatric symptoms such as depression, cognitive impairment, anxiety, suicide, and delirium [1,2]. Cognitive impairment occurs in dialysis patients at more than twice the rate observed in the general population, and 70% of hemodialysis patients over 55 years have moderate to severe cognitive impairment [3].
Cognitive impairment in dialysis patients increases mortality and hospitalization rates [4-6]. It also makes it difficult for patients to take decisions regarding treatment due to negative effects on the patient’s decision making and self-management skills [7]. Cognitive impairment is known to adversely affect quality of life and mental health [8].
There are a number of factors that affect cognitive impairment in PD. In PD patients, cognitive impairment is affected by depression, hyponatremia, vitamin D deficiency, cardiovascular risk factors, inflammation, and treatment compliance [9,10]. Recent studies have shown a significant relationship between mental health and dialysis adequacy in PD patients [11-14].
Kt/V [(dialyzer clearance×time)/Volume], an indicator of dialysis adequacy, is a ratio of urea clearance and time to the distribution of urea and has been used to measure the effect of dialysis on waste removal [15]. The association between Kt/V with depression and cognitive impairment is controversial [11-14,16-18]. Several studies using different cognitive measurements showed no significant association [11,13]. In contrast, one study showed that Kt/V values greater than 1.2 were associated with severe cognitive impairment. Other studies showed significant relation between cognition and Kt/V [12,19].
Relative overhydration (RelOH), another way of measuring dialysis adequacy, is the ratio of absolute volume overhydration to extracellular water. PD patients are known to have higher body water content than hemodialysis patients, which affects their cognitive function [20]. However, there are only a few studies on the relationship between RelOH and cognition compared to Kt/V in PD patients. One study measured Health related quality of life over 12 months in PD patients and found that the cognitive domain scale of this test was significantly associated with changes of RelOH [14].
To date, previous studies have shown controversial results regarding the association between dialysis adequacy and cognitive function in PD patients. Moreover, there are only a few studies on its relationship with RelOH. Therefore, this study aimed to investigate the association between cognitive function and dialysis adequacy in PD patients.
METHODS
Participants
Our cross-sectional study included all prevalent end-stage renal disease patients who underwent PD from September 2018 to February 2019. All subjects provided written informed consent. The study was approved by the Institutional Review Board of Busan Paik Hospital, Inje University College of Medicine (IRB No. 18-0131). The subjects included patients who were more than 90 days from initiation of PD, were more than 19 years old, and had no proven psychiatric disorder. Eightyfive PD patients were eligible. In the first 6 months of the study period, three patients transferred from PD to hemodialysis, two underwent kidney transplantations, four died, and 14 refused to participate in the study. Sixty patients met the conditions and one of them failed to complete the test and was excluded. Finally, the study included 59 PD patients.
Clinical and laboratory characteristics
Demographic and comorbidity conditions including age, sex, PD vintage, body mass index, blood pressure, and primary kidney disease, were recorded. Biochemical data including serum albumin, blood urea nitrogen, serum calcium, phosphate, hemoglobin, and C-reactive protein (CRP) were collected.
Body composition measurements were made with the Body Composition Monitor (Fresenius Medical Care, Bad Homburg, Germany). Measurements were taken after the emptying of peritoneal dialysate with the patients in a relaxed, supine position in an isolated room. All measurements were performed by a trained renal nurse. To assess the fluid status, we used RelOH, which was defined as the ratio of absolute volume overload [OH(L)] to extracellular water (ECW) [21]. Kt/V was defined as peritoneal Kt/V urea and creatinine clearance based on residual renal function [22,23].
Measurement of depression and cognitive impairment
Depression was measured by the Beck Depression Inventory (BDI), which is a self-assessment instrument designed to evaluate the presence and severity of depressive symptoms. It consists of 21 questions. The higher the total score, the more severe the depression. In this study, patients were diagnosed with depression if their scores were equal to or greater than 10 [24].
Language learning, language memory, working memory, short-term memory, long-term memory, agility, and visual motor coordination abilities were measured through various tests (Digit Symbol Substitution Test, Hopkins Verbal Learning Test, Wechsler memory scale-spatial span, Wisconsin Card Sorting Test). The Digit Symbol Substitution Test is used to measure short-term memory, agility, and visual motor coordination abilities. In this study, we conducted a transposition test included in the Korean Wechsler Adult Intelligence Scale-IV (K-WAIS-IV) guideline [25]. It consists of seven exercises and 93 main tests, with a time limit of 90 s. The Hopkins verbal learning test (HVLT) is used to assess language learning and language memory and consists of immediate recall, delayed recall, and reexamination. In this study, we used the Korean version of the HVLT [26]. The Wechsler memory scale-III, in which spatial span is used to assess working memory, is a nonverbal test. The score of this test is measured by adding the forward and backward spatial spans. The higher the score, the better the working memory [27]. The Wisconsin Card Sorting Test (WSCT) is a representative test to measure executive function and it mainly evaluates the number of completed categories, error rate, rate of repetition, rate of error in secular rate, rate of nonspeed error, and the number of attempts to acquire the first category [28].
Statistical analysis
Sex and comorbidities were expressed as percent (%), and continuous variables such as demographic information and biochemical test values were presented as mean and standard deviation. To examine the association of Kt/V and RelOH with cognition, partial correlation analysis was used. To avoid bias by cofounding variables, we controlled age, education, and depression which are known to affect cognitive impairment [29-31].
The level of significance was set at 0.05 and the correlation coefficient r was calculated. All analyses were performed with the Statistical Package for the Social Sciences 24.0 (IBM Corp, Armonk, NY, USA).
RESULTS
Baseline characteristics
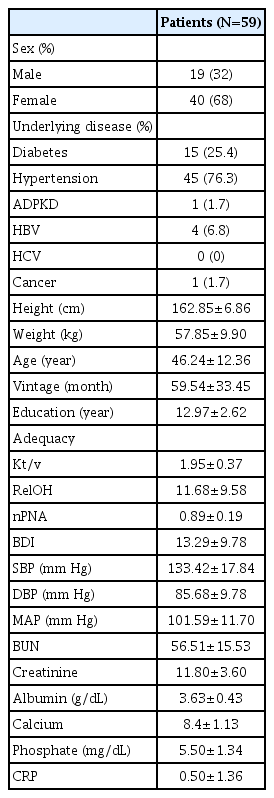
Demographic and clinical assessment data are presented in Table 1 and 2.
Characteristics in peritoneal dialysis patients

Cognition in peritoneal dialysis patients
Of the 59 PD patients, 40 (68%) were female, 15 (25.4%) had diabetes, 45 (76.3%) had hypertension, and 1 (1.7%) had cancer. The mean values of age and dialysis vintage of the subjects were 46.24 years and 59.54 months, respectively. None were diagnosed with any cerebrovascular accident and/or myocardial infarction.
Depression and clinical characteristics
Thirty-three patients (56%) showed mild to severe depression and the mean BDI score was 13.3. The following values were found: mean serum albumin, 3.63 q/dL; creatinine, 11.8 mg/dL; CRP, 0.50 mg/dL; mean total Kt/V, 1.95; mean RelOH, 11.7; and the normalized protein nitrogen appearance (nPNA), 0.89 q/kg/day.
Correlation between dialysis adequacy and cognition
Kt/V was not significantly correlated with cognitive function in PD patients. However, Kt/V had a tendency for positive correlation with categories achieved (r=-0.25, p=0.07) and a negative correlation with trials to complete first category (r= -0.24, p=0.08) (Table 3).

Correlation between cognition and Kt/V (N=59) in peritoneal dialysis patients
RelOH was negatively correlated with categories achieved (r=-0.32, p=0.02) and positively correlated with trials to complete first category (r=0.31, p=0.02) (Table 4) [32].
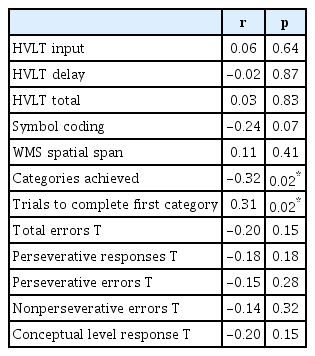
Correlation between cognition and RelOH (N=59) in peritoneal dialysis patients
DISCUSSION
In this study, we examined the association between dialysis adequacy and cognitive function in PD patients. Kt/V, an indicator of dialysis adequacy, was not significantly correlated with cognitive function. However, another indicator, RelOH, was significantly correlated with WCST which is a task known to represent executive function. RelOH was positively correlated with the number of categories completed and negatively correlated with the number of attempts to acquire the first category, which means that higher RelOH is related to lower cognitive function.
These results are consistent with previous findings that Kt/V is not associated with global cognition impairment. However, some studies have shown a significant association between Kt/V and cognitive function. One study showed a negative correlation between dialysis adequacy and short-term memory [11]. In this paper, the authors hypothesize that patients undergoing intensive dialysis have higher sensitivity to toxicity, resulting in various comorbidities that lead to cognitive impairment. The average Kt/V of our study (1.95) is higher than the standard suggested by the US National Kidney Foundation-Kidney Disease Outcomes Quality Initiative, and therefore shows no significant correlation with cognitive impairment. Another study of hemodialysis patients showed a negative correlation between Kt/V and the Trail Making Test B, which indicates executive function [33]. This difference is presumed to be attributed to the use of different measures for memory and executive functions in the current and previous studies. The WCST used in this study is known to cover a wider range of executive functions than the Trail Making Test B [34]. In previous studies, stroke and cardiovascular accidents are mentioned as major factors of cognitive impairment in dialysis patients [2,3,12]. In this study, there were no patients with cerebrovascular disease or stroke, which seems to have made a difference in previous studies.
Previous studies have shown that executive function and concentration, in chronic renal failure patients who do not receive dialysis, are further impaired than memory [35]. There was also a study showing that executive function and concentration improved, especially in the PD group, on comparing the function across 12 months in the group that received PD [36]. Consistent with these previous results, our study shows that high RelOH is associated with low executive function. Moreover, the low correlation with RelOH (categories achieved; r= -0.32, trials to complete first category; r=-0.31) seems to be due to its role in improving executive function.
In patients with chronic renal failure undergoing dialysis, cognitive impairment is explained by cardiovascular abnormalities such as hypertension, hyperlipidemia, and cerebral infarction and non-cardiovascular abnormalities such as aging, chronic inflammation, neurotoxicity, and oxidative stress [2,10,20,37]. Changes in body fluids during dialysis can lead to edema and decreased blood pressure and blood flow in the brain, which may increase the risk of transient ischemic attacks and cerebral infarction, causing cognitive impairment [3]. However, in a study comparing PD patients with non-dialysis chronic renal failure patients, there was no difference in cognitive function even when blood pressure and pro-brain natriuretic peptide were corrected [20]. This finding is consistent in our study due to the fact that there is no significant association between hypertension, systolic blood pressure, and cognitive function.
It is hypothesized that hyponatremia can be easily predicted by RelOH in dialysis patients, and that its neurotoxicity causes cognitive decline. In a study using the Trail Making Tests B, the authors suggest that hyponatremia is particularly associated with executive function [38]. This is consistent with our study due to the fact that RelOH was significantly associated with low executive function.
This study has some limitations. First, past history of cerebrovascular accidents is known to be one of the mechanisms leading to cognitive impairment in dialysis patients, but patients who participated in our study did not have any history of cerebrovascular accidents [2]. Second, cognitive function and dialysis adequacy of the patients in our study were comparatively well maintained. Since patients with severe disease tend to have lower participation rates in studies, the 14 patients who did not participate in this study may have had severe symptoms [39]. Third, cognitive function may be affected by some medical conditions such as diabetes mellitus or hypertension, however these were not included as control variables in our analysis. Finally, this study is cross-sectional in nature and does not clearly identify the cognitive changes of patients undergoing dialysis.
In this study, we investigated the relationship between dialysis adequacy and cognitive function in PD patients. Although, there was a significant association between executive function and RelOH, the former had no significant association with Kt/V. These results suggest a new role of RelOH as a tool to assess cognitive function in PD patients.
Acknowledgements
The authors thank the staff of the Peritoneal Dialysis Center of the Busan Paik Hospital for their assistance with the process of this study.
This work was supported by a grant from 2018 Inje University Busan Paik Hospital research grant.
Notes
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Dong Jin Shin, Taehee Kim, Do-Un Jung. Data curation: Dong Jin Shin, Sung-Jin Kim, Yunmi Kim. Formal analysis: Dong Jin Shin, Taehee Kim, Do-Un Jung. Funding acquisition: Taehee Kim. Investigation: Dong Jin Shin, Sung-Jin Kim, Yunmi Kim. Methodology: JungJoon Moon, Dong-Wook Jeon, Yeong Hoon Kim, Sun Woo Kang. Project administration: Taehee Kim, Do-Un Jung. Resources: Jung-Joon Moon, Dong-Wook Jeon, Yeong Hoon Kim, Sun Woo Kang. Writing—original draft: Dong Jin Shin. Writing—review & editing: Taehee Kim, Do-Un Jung.