INTRODUCTION
Somatic symptoms commonly include cardiopulmonary, gastrointestinal, pain, and general symptoms [1-3]. Somatic symptoms in psychiatry include underlying depression, anxiety, or other psychiatric disorders [4-6]. People with such somatic symptoms often visit the department of internal medicine rather than visiting the department of psychiatry first. Specifically, after patients visit the department of internal medicine and are told that they have no specific abnormal finding, they finally visit the department of psychiatry. When examining such patients, psychiatrists may consider the section on ŌĆ£Somatic Symptom and Related DisordersŌĆØ in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) from a diagnostic perspective [7]. In particular, doctors in charge needs to find out what somatic symptoms their patients have. In this case, the Patient Health Questionnaire-15 (PHQ-15) can be very useful [8].
The PHQ is a tool that can easily screen depression, anxiety, alcohol, eating, and somatic symptom-related mental disorders when diagnosing patients. The PHQ has been translated into over 20 languages, and is widely used worldwide [9,10]. In particular, the PHQ-15 is a PHQ version that can detect somatic symptoms, and is a tool for measuring the type and severity of somatic symptoms that patients are currently complaining of. In South Korea, the PHQ-15 was assessed in a validation study by Han and his colleagues, and has being utilized usefully so far [11]. The Somatic Symptoms Scale-8 (SSS-8), which is intended to be verified in this study is a short form of the PHQ-15.
The SSS-8 is composed of a total of 8 items excluding items regarding menstrual problems, sexual problems, and fainting contained in the PHQ-15. It was originally developed by Kroenke et al. [8], and known as the PHQ-Somatic Symptom Short-Form [12]. However, the validation study for this tool was conducted by Gierk et al. [13] in Germany, and its name was changed to SSS-8, accordingly. That study proved that the internal consistency of SSS-8 was suitable, and revealed that it consisted of a 4-factor structure (gastrointestinal, pain, fatigue, and cardiopulmonary). In addition, that study classified severity into 5 categories, and proposed severity categories to easily check the severity of symptoms. Following this, a validation study for a Japanese version of the SSS-8 was conducted, and also verified its reliability and validity [14]. Furthermore, that Japanese study verified the known-group validity, and explained somatic symptoms according to group. As found in the aforementioned previous studies, the SSS-8 is a useful tool to assess somatic symptoms and severity of patientsŌĆÖ complaints in a short time in the clinical settings. Despite the clinical usefulness of the SSS-8, the translation and validation of the SSS-8 has not been conducted in South Korea.
This study aimed to conduct a validation study of a Korean version of the SSS-8 (K-SSS-8), and to utilize the K-SSS-8 effectively in clinical settings.
METHODS
Development of the Korean version of the Somatic Symptom Scale
Before developing the K-SSS-8, we first obtained permission from the original authors of the SSS-8 for the validation study of the Korean version. Subsequently, 3 psychiatrists and 1 clinical psychologist translated the SSS-8 into Korean, and an individual with a doctorate degree in the US, who are fluent in both English and Korean, back-translated the Korean version. After 2 psychiatrists and a psychologist with a PhD in psychology conferred, the K-SSS-8 was finalized (Supplementary Materials in the online-only Data Supplement).
Participants
The study period was from March 2017 to March 2019. The participants consisted of healthy controls and patients. The healthy controls included 188 public officers working in small- and medium-sized cities in Jeollabuk-do, South Korea. Data from a total of 167 public officers, except for 11 with insufficient responses and 10 with serious medical conditions, were used for analysis. Among them, a total of 31 were retested for test-retest reliability testing after 3-4 weeks. In the case of the patient group, the participants were 32 patients who visited the Department of Psychiatry at our hospital and complained of somatic symptoms. Among them, data from a total of 23 patients, except for those with a high degree of psychosis and underlying serious and obvious medical conditions, were used for analysis. This study was approved by the Institutional Review Board of Wonkwang University Hospital (No. WKUH 2017-04-007-001), and all the participants provided written informed consent before starting the study.
Measures
The EuroQol 5 Dimension (EQ-5D), the PHQ-15, and the PHQ-2 scales were used to test the reliability and validity of the K-SSS-8.
EuroQol 5 Dimension
The EQ-5D was developed to measure general health status [15]. The EQ-5D consists of a total of 5 items regarding mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, with responses measured using a 1-3 point-Likert scale. A higher score indicates poorer health status. A validation study of the Japanese version of SSS-8 found that there was positively significant correlation between the EQ-5D and the Japanese version of the SSS-8 [14].
Patient Health Questionnaire-15
The PHQ-15 is a scale that consists of 15 items only related to somatic symptoms among all the items contained in the PHQ. Each item is rated on a 0-2-point scale, and the total score ranges from 0 to 30 points. In this study, the Korean version of the PHO-15 translated by Han et al. [11], was used. The internal consistency of PHQ-15 was 0.834 in this study, showing a ŌĆ£goodŌĆØ internal consistency.
Patient Health Questionnaire-2
The PHQ-2 consists of two items regarding depression among the items contained in the PHQ-9. The two items ask about depression and anhedonia respectively. As in a study regarding the Japanese version of the SSS-8, a binary response consisting of ŌĆ£yesŌĆØ or ŌĆ£noŌĆØ was used in this study. If anyone responds with ŌĆ£yesŌĆØ to at least one item, he or she is considered to have depression. Using this, the participants were divided into three groups according to the degree of depression (group 1: depression-positive for two items; group 2: depression-positive for one item; and group 3: depression-negative for two items), and the degree of somatic symptoms according to the group was analyzed.
Statistical analysis
First, frequency analysis was performed for descriptive statistics of the participants. Internal consistency and test-retest were used to validate reliability. Internal consistency was tested using CronbachŌĆÖs alpha. Pearson correlation analysis was performed to verify test-retest. Construct validity and concurrent validity verification were performed to test validity. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were performed to verify construct validity, and correlation analysis was performed to verify concurrent validity. The Maximum Likelihood (ML) and Oblique rotation (Direct Oblimin) methods were used for the EFA, while Tucker-Lewis Index (TLI), Comparative Fit Index (CFI), and Root Mean Square Error of Approximation (RMSEA) among goodness-of-fit indices were used for the CFA. When TLI and CFI are 0.90 or higher, it is ŌĆ£acceptable,ŌĆØ [16,17] and when RMSEA is 0.08 or lower, it can be deemed ŌĆ£acceptable.ŌĆØ [18]
Known-group validity was verified, and the participants were classified into three groups according to the responses to the PHQ-2 items (group 1: those who responded with ŌĆ£yesŌĆØ to both of the two items; group 2: those who responded with ŌĆ£noŌĆØ to any of the two items; and group 3: those who responded with ŌĆ£noŌĆØ to the two items). Jonckheere-Terpstra test, a nonparametric test, was performed to verify the mean difference between the groups [19]. Finally, frequency analysis according to score range was performed to classify the severity of the K-SSS-8. All statistical analyses were conducted with SPSS and AMOS 18.0 for windows (SPSS Inc., Chicago, IL, USA). The set level of significance was 5%.
RESULTS
Descriptive statistics of the sample
Table 1 shows the demographic characteristics and descriptive statistics of the participants. The mean age of the healthy control group was 41.67 years. The age ranges from 26 to 63. Of the participants, 23.4% were male, and 76.6% were female. The mean duration of education was 15.83 years. In addition, 28.1% were unmarried, and 69.5% were married. In terms of income level, the proportion of those with income of between KRW 2 million and KRW 3 million were the highest with 36.5%. The proportions of smokers and non-smokers are 90.4% and 9.6%, respectively.
Meanwhile, the mean age of the patient group was 55.95 years old, and 39.1% were male and 60.9% were female. The age ranges from 21 to 73. The mean duration of education was 11.39 years. Among them, 8.7% were unmarried, and 73.9% were married. In terms of income level, the proportion of those with income of between KRW 1 million and KRW 2 million was the highest with 26.1%. The proportions of smokers and non-smokers were 52.2% and 47.8%, respectively.
The variables of age, years of education, gender, marital status, income level, and smoking status showed significant differences between the two groups [t (188)=6.55, p<0.001 for age; t (188)=13.25, p<0.001 for years of education; Žć2=15.39, p<0.001 for marital status; Žć2=15.39, p<0.001 for income level; Žć2=15.39, p<0.001 for smoking]. Since the purpose of this study is not a study for verifying the mean difference between the two groups, it is considered to be a study on the reliability and validity of the scale, so it seems that the differences in the demographic data does not have a significant effect on the validation study for the scale.
Internal consistency and test-retest reliability
The results of investigating internal consistency among reliability showed that the CronbachŌĆÖs alpha of the K-SSS-8 was 0.85. The verification of test-retest reliability was also found to be suitable (r=0.777, n=31, p<0.001).
Concurrent validity
Table 2 shows the results of the correlation analysis between K-SSS-8 and EQ-5D, PHQ-2, and PHQ-15 to verify the concurrent validity of K-SSS-8. The K-SSS-8 showed significant correlation with all the three scales (For EQ-5D, r=0.493, n=167, p<0.001; for PHQ-2, r=-0.226, n=167, p<0.01; for PHQ-15, r=0.857, n=167, p<0.001).
Construct validity
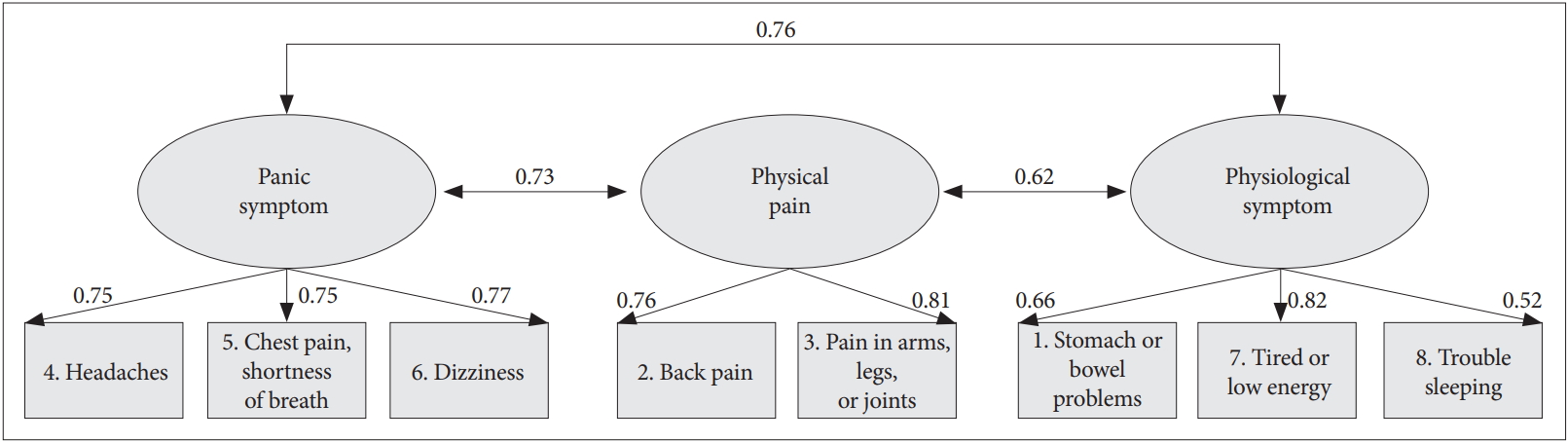
First, it was found that factor analysis can be performed through Kaiser-Meyer-Olkin (KMO) values and BartlettŌĆÖs test of sphericity [KMO=0.863; Žć2 (df=28, n=167)=476.348, p<0.001] [20]. The result of exploratory factor analysis showed that the 3-factor structure was found to be the most valid. The explanatory power of the 3-factor structure was 71.59%, and the RMSEA value was found to be suitable with 0.00. The results of performing CFA to verify the goodness-of-fit of the 3-factor structure showed that the 3-factor structure was found to be suitable with TLI of 1.022, CFI of 1.000, and RMSEA of 0.00. Table 3 shows the results of verification according to the number of factors. The first extracted factors included item #6 (ŌĆ£DizzinessŌĆØ), item #4 (ŌĆ£HeadachesŌĆØ), and item #5 (ŌĆ£Chest pain or shortness of breathŌĆØ). The authors of this study named the first factor as ŌĆ£Cardiopulmonary.ŌĆØ The second extracted factor was item #2 (ŌĆ£Back painŌĆØ), and item #3 (ŌĆ£Pain in your arms, legs, or jointsŌĆØ), which were named as ŌĆ£Pain.ŌĆØ Lastly, the third factor extracted included item #1 (ŌĆ£Stomach or bowel problemsŌĆØ), item #7 (ŌĆ£Feeling tired or having low energyŌĆØ), and item #8 (ŌĆ£Trouble sleepingŌĆØ), which were named as ŌĆ£Gastrointestinal and Fatigue.ŌĆØ Table 4 shows each item and factor loading value according to factors, and Figure 1 shows items according to each factor name.
Known-group validity
The number of those who responded with ŌĆ£yesŌĆØ to both items of the two of the PHQ-2 was 87, accounting for 52.10%. The number of those who responded with ŌĆ£noŌĆØ to any item of the two was 22, accounting for 13.2%. In addition, the number of those who responded with ŌĆ£noŌĆØ to both items was 58, accounting for 34.7%. The results of verifying the difference in the total score of K-SSS-8 between the three groups also showed significant difference (for Jonckheere-Terpstra test, J-T statistic=-2.510, p<0.05). Table 5 shows the results of verifying the mean difference in the total scores of the K-SSS-8, the PHQ-15, and the EQ-5D between the three groups.
Severity categories
As in previous studies, severity categories were set (a total of 5 categories), and the percentiles according to severity categories are shown in Table 5. A score of 0 to 3 points were classified as ŌĆ£no to minimalŌĆØ severity, a score of 4 to 7 points as ŌĆ£low,ŌĆØ a score of 8 to 11 points as ŌĆ£medium,ŌĆØ a score of 12 to 15 points as ŌĆ£high,ŌĆØ and a score of 16 points or higher as ŌĆ£very high.ŌĆØ In the case of the healthy control group, more than half of the participants had ŌĆ£no to minimalŌĆØ and ŌĆ£lowŌĆØ severity, and those with ŌĆ£highŌĆØ and ŌĆ£very highŌĆØ severity accounted for about 20%. In the case of the patient group, the participants with ŌĆ£no to minimalŌĆØ and ŌĆ£lowŌĆØ severity accounted for about 35%, and those with ŌĆ£highŌĆØ and ŌĆ£very highŌĆØ severity accounted for about 43% (Table 6).
DISCUSSION
In this study, the SSS-8 was translated into Korean language for local adaption, the reliability and validity of its Korean version, the K-SSS-8 was verified, and its clinical utility was investigated. The implications of the results are as follows.
First, the reliability analysis revealed that internal consistency and test-retest reliability were reliable. The internal consistency reliability of the K-SSS-8 was slightly better compared to previous studies (CronbachŌĆÖs alpha=0.81 in a study by Gierk et al.) [13]. Test-retest reliability could not be compared because it had not been verified in previous studies [13,14]. However, in this study, the test-retest reliability of the K-SSS-8 was found to be a statistically reliable level [21]. Taken together, the reliability of the K-SSS-8 can be judged to be reasonably high.
Next, the results of verifying the goodness-of-fit of the number of factors in the validity analysis showed that the 3-factor model was the most suitable. The explanatory variance explained by the three factors in the 3-factor model was also more than 70%, and the RMSEA value was less than 0.05, indicating ŌĆ£excellent.ŌĆØ [18] In the EFA analysis, the 4-factor model showed an adequate goodness-of-fit, but in the CFA verifying the goodness-of-fit of the entire model, its goodness-of-fit was not satisfied. The reason is presumably thought to be due to the fact that when one factor was added from the 3-factor structure to the 4-factor structure, one item was assigned to the added factor. Because one factor can usually contain at least 2-3 items [5,22], the authors judged that it was not good in terms of economic feasibility and goodness-of-fit of the model when one item was generated as one factor [23]. Meanwhile, this same problem occurred in the previous study by Gierk et al. [13], but it seems that they selected a higher-order structure added with a general factor to solve with a 4-factor model. However, the authors of this study judged that the 3-factor model is adequate and concise for 8-item classification based on statistical theories. The implications of each factor in the 3-factor model are as follows.
The first factor was named as ŌĆ£Cardiopulmonary,ŌĆØ and included item #6: ŌĆ£Dizziness,ŌĆØ item #4: ŌĆ£Headaches,ŌĆØ and item #5: ŌĆ£Chest pain or shortness of breath.ŌĆØ In the study of Gierk et al. [13], items #5 and #6 were grouped and expressed as cardiopulmonary symptoms. In this study, those 3 items were considered to be included in 13 types of Panic attack specifier in the DSM-5, and were thus named as ŌĆ£Cardiopulmonary.ŌĆØ Recently, the number of people complaining of panic-like symptoms is increasing, and the number of patients with panic disorder in hospitals is also increasing. The first factor ŌĆ£CardiopulmonaryŌĆØ is thought to be very useful in predicting people who are likely to develop panic disorder. So the first factor is likely that the mental health professionals will be able to identify symptoms easily, directly, and quickly. In particular, the items ŌĆ£Chest pain or shortness of breathŌĆØ and ŌĆ£DizzinessŌĆØ correspond to Panic disorder diagnosis criteria, so the factor can serve as evaluation items for diagnosis. On the other hand, the ŌĆ£HeadachesŌĆØ question is included, which is not consistent with the question of diagnose for the Panic disorder, but is a symptom that is often followed with Panic disorder. Unlike the findings of Gierk and his colleagues, the ŌĆ£HeadachesŌĆØ question was included in the ŌĆ£CardiopulmonaryŌĆØ factor, perhaps due to differences in cultural background. When complaining of cardiopulmonary function problems, Koreans tend to complain of dizziness and headaches. It would be better to conduct a replication study on this part.
The second factor ŌĆ£PainŌĆØ included item #3: ŌĆ£Pain in your arm, legs, or joints,ŌĆØ and item #2: ŌĆ£Back pain.ŌĆØ The second factor literally means physical or body pain, and is thought to be common in patients with physical illness. In the study by Gierk et al. [13], it was also named ŌĆ£PainŌĆØ factor. The second factor, ŌĆ£PainŌĆØ is thought to be very useful for detecting symptoms which appear on the surface of the body, such as the back and joints. The second factor includes pain in the back and joints, and when responding to questions related to ŌĆ£Pain,ŌĆØ it seems that physical of surgical problems may be considered first. If the patient complains of symptoms related to the ŌĆ£PainŌĆØ factor even after excluding physical or surgical problems, the mental health professionals may consider ŌĆ£Somatic Symptoms and Related Disorders.ŌĆØ
Finally, the third factor, ŌĆ£Gastrointestinal and FatigueŌĆØ included item #1: ŌĆ£Stomach or bowel problems,ŌĆØ item #7: ŌĆ£Feeling tired or having low energy,ŌĆØ and item #8: ŌĆ£Trouble sleeping.ŌĆØ The third factor is mainly related to physiological symptoms, which are often accompanied by complaints of somatic symptoms. This factor is thought to be closely related to digestive problems, sleep problems, and decreased vitality which are commonly observed in patients with depressive disorder, anxiety disorder, somatic symptoms, and related disorders. It is thought that the third factor enables us to quickly detect the presence or absence of physiological symptoms through the third factor. The third factor includes stomach and fatigue problems. From a psychiatric perspective, these problems are often accompanied by depression and anxiety. Therefore, there may be cognitive and emotional depression and anxiety at the basis of patients with gastrointestinal symptoms and fatigue, and in this case, it is recommended to conduct an additional scale related to depression and anxiety. Unlike Gierk et al. [13] findings, the ŌĆ£stomach and bowel problemsŌĆØ item was included in the ŌĆ£fatigueŌĆØ factor, which may be due to differences in cultural background. Koreans are known to be primarily accompanied by fatigue and gastrointestinal problems when stressed. Also, it would be better to have a replication study on this part.
In this study, Known-group validity was also verified using a Jonckheere-Terpstra test. According to the participantsŌĆÖ responses (depression) to the PHQ-2, the participants were divided into three groups (group 1: depression-positive for both items; group 2: depression-positive for one item; and group 3: depression-negative for both items). The verification showed that there was a significant difference in the total K-SSS-8 score according to the degree of depression. Similarly, in terms of PHQ-15 and EQ-5D, there was a significance difference in the total scores between the groups. These results suggest that depression may be closely related to the complaint of somatic symptoms [6,24]. It is known that 50-70% of patients with somatic symptoms and related disorders have a comorbid mental disorder, usually accompanied by depression and anxiety [7]. Therefore, for patients complaining of somatic symptoms, it may be necessary to examine more thoroughly through interviews or measurements whether they have underlying depression or anxiety [25].
In addition, frequency analysis according to the severity of the K-SSS-8 was performed for healthy control and patient groups in this study. In the case of the healthy control participants, the proportion of those who had higher than ŌĆ£mediumŌĆØ severity was 43.2%, which is twice as high as in Japan (20.6%) [14]. These results may be due to the fact that the participants were limited to public officers as the healthy control population, and it is thought that about half of these participants had at least 2-3 somatic symptoms.
In the case of the patient group, the proportion of those who had higher than ŌĆ£mediumŌĆØ severity was 65.1%, unlike the control group, and about 2/3 of the participants in the patient group complained of at least 2-3 somatic symptoms. Diagnostically, more than 90% of them had been diagnosed with depression or anxiety-related disorders, and had no medical abnormalities. It is known that a significant number of patients who complained of somatic symptoms without a medical condition initially visited the internal medicine departments [26]. This suggests that consultation between internal medicine and psychiatry departments is required, and the importance of consultation [27].
Taken together, in terms of clinical utility, the K-SSS-8 can be useful for exploring symptoms such as panic symptoms, physical pain, and physiological symptoms experienced by patients in a short time. In addition, the K-SSS-8 is expected to be very useful for determining the current severity by using the severity categories and for establish additionally required assessment plans for depression and anxiety symptoms. In particular, a K-SSS-8 score of 12 or higher is common in the patient group, but not common in the healthy control group. Therefore, ŌĆ£severe complaints of somatic symptomsŌĆØ should be considered when establishing treatment plans.
The K-SSS-8 is also thought to be useful in therapeutic aspects. Since the K-SSS-9 was divided into three factors (Cardiopulmonary, Pain, Gastrointestinal and Fatigue), it is thought that it will help to establish a pharmacotherapy or psychotherapy plan based on main symptoms. For example, it is known that the effect size of combined therapy (pharmacotherapy plus cognitive behavior therapy) is high for panic symptoms, and that when physiological symptoms are dominant, it is appropriate to consider pharmacotherapy first [28-30].
Lastly, the limitations and future research directions of this study are as follows: First, the factor analysis revealed that the number (n=167) of the participant of this study was within an appropriate range, but it is recommended that the number (n) of participants is more than 200 participants to improve the power of a test [31]. In addition, frequency analysis was performed with the data from the patient group, but it seems that it is desirable for the numbers of participants to be more than 50 so as to increase the power of a test. Second, severity levels could be identified using severity categories. However, cut-off scores are always used valuably in clinical settings. Therefore, it is considered that future studies are needed to investigate the total K-SSS-8 scores for patients with somatic symptoms and related disorders and to present cut-off scores through the receiver operating characteristic (ROC) analysis. Third, if complaints about somatic symptoms are common in patients with depression and anxiety disorders, it is considered necessary to perform K-SSS-8 analysis according to such disorders. With regard to depression and anxiety disorders, related study findings such as the distribution of total scores, distribution of scores for each factor, and cut-off score estimation for each disorder through ROC analysis are thought to be very useful in actual clinical settings.