The Factors Affecting the Relationship between Remission Status and Employment in Chronic Schizophrenia Patients
Article information

Abstract
Objective
Symptomatic remission have substantial effects in long-term schizophrenia outcome, but exact determinants of the employment. In this study, the relationship between employment and symptomatic remission in chronic schizophrenia patients and other factors related to employment were investigated.
Methods
100 patients interviewed were evaluated by the Positive and Negative Syndrome Scale (PANSS), Functional Recovery Scale in Schizophrenia (FROGS), Global Assessment of Functioning (GAF), Quality of Life Scale (QoL) and Subjective Recovery Assessment Scale (SubRAS). Sociodemographic variables, clinical features, antipsychotic dose and past working history obtained from patient interviews were investigated.
Results
The patients of 40% who participate in the study were symptomatic remission, but only 53.5% of these patients weren’t employed. Young age, especially, -regardless of the onset of illness- working a job in the past, low and moderate use CPED (equivalent doses according to chlorpromazine), shorter disease duration, symptomatic remission was found to be closely related to employment. While QoL, FROGS, GAF, and SubRAS total scores of employment group were higher than the unemployment group, PANSS total scores in the unemployment group were higher than that of the employment group. There was a high correlation between the scales and employment status.
Conclusion
Employment status was closely related with the remission status. This study supports that symptomatic remission alone is not decisive for employment. It was found that younger age, past working history (before or after the disease), low and intermediate CPED antipsychotic use and shorter duration of disease were closely related to employment with symptomatic remission.
INTRODUCTION
The long-term results of schizophrenia treatment have been evaluated by examining different clinical concepts including symptomatic remission, social and functional recovery [1-5]. Functional remission, which is firstly defined by Schizophrenia Working Group (SWG) including Andreasen, and many studies have shown clinical validity [6]. According to SWG, functional remission criteria based on Positive and Negative Symptoms Scale (PANSS) scores and remission duration [1]. No doubt, the functional outcome has a strong correlation with symptomatic remission and better subjective life satisfaction in patients with schizophrenia but not necessarily accompanied with functional remission in all domains [4,5,7].
However, many studies have shown that, even when symptomatic remission is reached, a significant proportion of patients still do not have social and vocational functioning [5,7-9]. Reach to employment plays a key role in the recovery and functioning of people with schizophrenia [10]. However, employment is not considered within the criteria of remission [1]. At this point, the question of whether the employment situation should have a place in even evaluating remission comes to mind. Because many patients with schizophrenia can not reach the recovery state, but the state of remission [1,5,9,10].
Some authors argue that employment is the most important goal of treatment in patients with schizophrenia because it provides economic independence, improves quality of life and self-esteem. Unfortunately, employment rates in patients with schizophrenia are reported at a low rate from 8% to 35% in various countries [11]. The most frequently reported factors associated with employment were negative symptoms and cognitive impairment, the age at onset, marital status, gender, youth, education, experience of employment, remission duration, often and longer previous hospitalizations, presence of comorbid physical health problems, working history, public support/disability income duration and course of the illness [12-15]. In addition, some authors reported that patients who recovered from schizophrenia had received lower antipsychotic dosages than those who did not recover [16]. These findings can be interpreted to important clues for identifying improvable employment related factors in patients with schizophrenia [11]. Furthermore, environmental factors such as welfare rights and the availability of vocational support programs are said to increase employment rates [17].
However, these are mostly independent factors, the number of studies involving approaches related to dynamic factors that can be changed by inclusion in the disease-related treatment program is still few [11].
The aim of this study is to investigate factors that may be associated with employment and relationship between remission and employment status, thus, it is necessary to identify the points that need to be focused on providing employment in treatment program.
We hypothesized that the social and functional remission especially subjective recovery feelings, quality of life might be more as important as the remission concept on employment. Furthermore, we examined whether antipsychotic doses used in treatment, past working history, duration of illness, number and duration of hospitalization in last two years and totally and the socio-demographic factors were related to employment status in patients with chronic schizophrenia.
METHODS
Procedure
During the survey period, which was performed between January 2015 and January 2016, there were approximately 350 chronic patients diagnosed with psychotic disorder who were following up by Community Mental Health Center (CMHC). The inclusion criteria of the study were being diagnosed with schizophrenia or schizoaffective disorder (according to the DSM-IV-R), being between 18–65 years old and had given informed consent. A written informed consent was obtained from each participant before their involvement in the study. All patients received a pharmacological and regular psychosocial support program at CMHC for the last two years. Comorbid neurological problems, having Electro Convulsive Therapy (ECT) for the last six months, being hospitalized in the last three months, having mental retardation diagnosis, having current alcohol or drug addiction and being illiterate were the exclusion criteria. According to exclusion criteria, 242 of patients were excluded. Since this study was designed as cross-sectional, the time criterion (remission should last at least six months) was not applied [5]. This study was conducted in accordance with the Declaration of Helsinki. Further, the study protocol was approved by the Kocaeli University Clinical Research Ethics Committee (Date/Decision Number: 2014/212).
Sociodemographic variables
The socio-demographic data collect form included information about age, gender, marital status, educational level, past and present employment status, social support, living conditions, diagnosis, hospitalization, antipsychotic treatment.
All patients treated with atypical antipsychotics. We classified antipsychotic equivalent doses according to chlorpromazine (CPED). If the required dose is lower than 600 mg/day we called as ‘low dose’, equivalent to 600 mg/day dose as ‘moderate dose’ and more than 600 mg/day as ‘high dose’ [11,18].
Measures
Symptoms of the patients were evaluated by the PANSS [19]. Functioning of the patients was assessed with the Functional Recovery Scale in Schizophrenia (FROGS). The FROGS is a specific scale designed for the measurement of functional remission in schizophrenia [20]. General functioning of the patients was assessed with Global Assessment of Functioning (GAF). The scale is a widely used scale independent of cross-cultural differences and has been reported to be reliable [21]. Life quality of the patients was assessed by Quality of Life Scale (QoL). QoL is a 21-item scale that assesses the quality of life in persons with schizophrenia [22]. Subjective recovery feeling of the patients was assessed with the Subjective Recovery Assessment Scale (SubRAS) that was designed to evaluate subjective recovery in patients with schizophrenia based on self-rating score [23].
PANSS
The PANSS was originally designed as a clinician rating scale that represents positive, negative and general psychopathology [19]. The reliability and validity of the Turkish version of the scale were studied by Kostakoğlu et al. [24] In our study, we used PANSS for assessing symptomatic remission in patients as proposed by Andreasen. In the PANSS, if P1, P2, P3 items from positive symptoms, N1, N4, N6 items from negative symptoms, and G5 and G9 items from general psychopathology symptoms scores were 3 or below, we assumed these scores appropriate for symptomatic remissions [1,5,6].
FROGS
FROGS was designed for the assessment of functional remission in schizophrenia. The scale was originally published under ‘‘FROGS’.’ It has been developed for the use of clinical outcome studies and patient evaluations [20]. The Turkish reliability and validity study of the scale was conducted by Emiroğlu et al. [25]
QoL
The QoL assesses four different domains in functioning: intra-psychic foundations, interpersonal relations, instrumental role, and common objects and activities [22]. The Turkish reliability and validity study of the scale was conducted by Soygür et al. [26]
SubRAS
SubRAS is a culturally sensitive instrument developed for the assessment of subjective recovery based on the self-rating evaluation. The scale has 17 items with one factor. The scale evaluates the person’s ideas about their personal and social life, ability to cope with stressful situations, having hopes and aims, and the ability to reach personal goals. The reliability and validity study of the scale was conducted by Yildiz et al. [23]
GAF
GAF is a widely used scale independent of cross-cultural differences, which has been reported to be reliable. The numeric scale (0 through 100) is rated by clinicians to assess the psychological, social and occupational/school functioning of individuals with schizophrenia [21,27].
Statistical analysis
We used Statistical Package Software Program 23.0 (IBM Corp., Armonk, NY, USA) for statistical analysis. The data were evaluated by the Kolmogorov-Smirnov test for normal distribution and normal distributions were observed. Employment and unemployment group were compared for age, education level, life style, age of onset, duration of illness, duration of hospitalization and measures scores by student-t test. The same groups were compared for gender, marital status, hospitalization in the last two years, history of working, employment status and CPED by chi-square test. The relation between measures scores were assessed by Spearman correlation test. Statistical significance was defined as p<0.05.
RESULTS
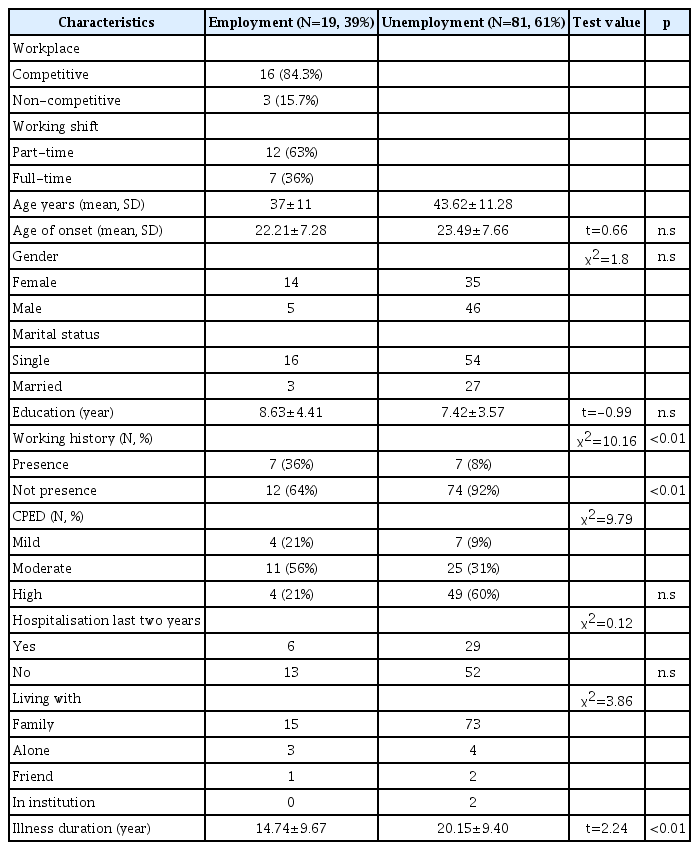
Patients consist of 40% were women. Most of the participants were single and having a long-term illness duration. Patients have an average disease duration of 19.12±9.65 years (Table 1).
Demographic and clinical characteristics of participant
Employed and unemployed groups were compared in terms of age, the age of illness onset, duration of illness, CPED, working history, marital status, education, life style, duration of education (years), number of hospitalizations for the last two years (Table 1).
Symptom severity measurement by PANSS total score and subscale scores), and scores on scales assessing including QLS, FROGS, GAF and SubRAS. CPED was significantly lower in the employment group. Additionally, although the retirees and students were assumed not to be working, patients with employment group had significantly more working history in the past. The mean age of the employed group was six years younger than the unemployment group, and their mean illness duration was nearly six years shorter than the unemployment groups too. In the employment group, having a working history was about four times more than non-employed group. Approximately 16% of the employees work in the non-competitive workplaces. Indeed 36% of employees were placed in a full-time work place by entering the state entrance exams (Table 1).
Forty patients were in symptomatic remission according to Andreasen remission criteria, except time period. Although it was not in remission, 7% of the patients were working (Table 2).

Comparison of remission and non-remission status between employment and unemployment groups (N±SD)
Regarding the QLS, FROGS, GAF, and SubRAS scores, the mean values of employment group were higher than unemployment group. Total PANSS scores in unemployment group was higher than the employment group (Table 3).
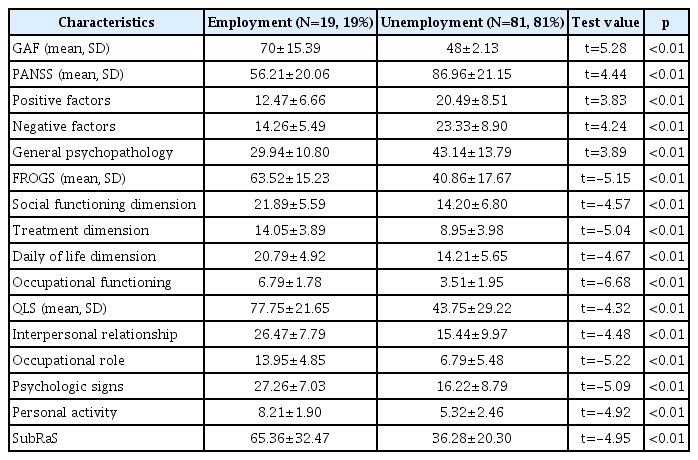
Comparison of scales between employment and unemployment groups
Spearman correlation was performed by using Total PANSS, FROGS, QLS, SubRaS, and GAF scales in the groups with and without employment. There was various and moderate correlation between the scales scores and employment status. In addition, all correlations were significant. You can see correlation coefficient and p values in Table 4.

Correlations of the PANSS, FROGS, GAF, QLS and SubRAS in employed patients (pearson correlation) (N=19)
DISCUSSION
We hypothesized that social and functional remission, especially subjective recovery feelings and quality of life might as more as important the remission concept determinant by symptomatic remission on employment. This study confirmed part of our hypotheses.
We found that social and functioning improvements (measured by FROGS, QoL, GAF, SubRAS) effective as symptomatic remission concept on schizophrenia except time criteria (measured by PANSS Total and Subscales) for employment status. In this context, we have not found any evidence that subjective well-being and quality of life for employment is determinative.
In our sample, nearly 20 percent of patients with chronic schizophrenia worked in different job types (Table 1). But only 37.5% of patients were able to work even though symptomatic remission occurred. Furthermore 7% of patients were employed even though being not symptomatic remission (Table 2). This result could be supporting the hypothesis that factors other than symptomatic remission also plays a role in the employment-related model. On the other hand, according to another study conducted in our country (they found employment rate in remission status were 47.5%), our employment rates are lower for having symptomatic remission patients [28]. However, it should not be overlooked that the patients in the sample in this study were younger and the disease duration was lower. Also, considering the multiple hospitalization and duration of disease, we should expect severe loss of functionality for our sample. Because of the deterioration in one or more of the main functional areas of the study or interpersonal relationships is expressed not only in chronic, multiple-episode schizophrenic patients, but also in patients with first episodes and even in ultra-high-risk (UHR) individuals for psychosis [29,30].
Our employment rate was twofold lower compared to the average employment rate in population studies in Turkey. The employment rate in the general population was reported as 46.3% at that time [31]. Similarly, in a European study, the highest rate of employment in patients with schizophrenia was reported by Germany at 30.3%, at the same time, the employment rate of the general population in that country was 65.4% [14,32]. In a nutshell, as in our study, there were twofold differences. However, the huge reduction in working time and decreased desire to work in patients with longer disease duration is remarkable in a recently study that examined the working lives of schizophrenic patients in Turkey [33]. For a sample of patients like ours, suffering from relatively older and longer-term illnesses, this result may support our low rate of employment result.
Most of the employed patients were in part-time jobs (%63), some of them working in supported/non-competitive workplaces (%15) (Table 1). Another multicenter study in our country included patients when the students were excluded, they found employment rate around 17%, rate of who working fulltime were 13.5% [14]. These results are very close to our results. The authors concluded that supported employment evidencebased practice and appears to be the most effective type of work rehabilitation [34]. A recent large-scale meta-analysis shows that due to the tremendous impact of schizophrenia in various areas of daily functioning, participation in rehabilitation therapy targeting employment outcomes is not sufficient to achieve labor stability. In addition, it’s another remarkable issue that our patients who work were full-time employed by special cadre examination in their institutions. This is a finding that supports the employment of schizophrenia patients as a social responsibility project of state [15,17].
In this study, a comprehensive approach that considers the dynamic interaction between unemployment rates, personal characteristics and professional rehabilitation results and a coordinated effort between health services, employment services and social services is indicated to be necessary for addressing unemployment. Coupled with targeted interventions, neurocognitive therapy and work-related social skills training seem to carry the key to successfully addressing the multidimensionality of work disability [10].
Employment rate increases with the advanced level of education [13,17]. In addition, it is reported that the increase in the level of education is also related to better psychopathology level [35]. Unfortunately, the mean education level of the patients in our study is 7.65±3.75 years. However, it should not be forgotten that the rate of participation in non-formal education in our country is only 22.7% in the same period [36]. No difference was found between the two groups in terms of educational level, which may be due to the fact that the patients in our sample consist of patients with similarity in terms of many sociodemographic data.
Additionally, it’s clear that women in our society are more disadvantaged than men for employment. In Turkey, the ratio of working women in the general population is 25.9% [36]. Culture, gender roles, religion, and family structure might change the female employment rate [16]. However, in this study, we could not find a significant difference in gender between the employment and non-employment groups (12.5% of female patients had employment) as was the other multi-center study [14]. Also, in multi-center study which investigated socio demographic characteristics of schizophrenia patients in Turkey, there was no difference between men and women in terms of study [37]. This is actually an entertaining finding. This may be interpreted as stigmatization due to schizophrenia may have a stronger impact even more than gender roles. It is known that even if the general course of the disease is good and symptoms improve, these people are still disadvantaged in terms of employment, they cannot get rid of social stigma, and this situation increases in competitive workplaces, especially in economic crisis situations [34,38].
High employment rate finding in young age patients is common in similar research population [12,14,17]. However, there were no differences between the two groups in terms of the age of onset of the disease, the number of hospitalizations in the last two years, education level and lifestyle. This may be related to the relatively homogeneous nature of the disease in terms of onset and course of disease. It may make our results more generalizable too.
Our patients received atypical antipsychotic treatment during the last two years of the regular psychosocial treatment program at the CMHC. In CMHC, we apply some psychosocial interventions such as cognitive remediation, psychoeducation, social skills training which have been found to be more effective in schizophrenia rehabilitation. While 53% of our patients were using high dose antipsychotics, only 11% were taking low doses (Table 1). In addition, there is no data available in this issue for our country about whether it is a traditional attitude as it is stated in East Asia [39].
There are controversial findings about the use of high and / or low dose antipsychotics. Interestingly, the relationship between high-dose antipsychotic treatment and lower overall mortality was demonstrated in a large-scale Swedish cohort study [40].
Differently some researcher reported that patients who recovered from schizophrenia had received lower antipsychotic dosages than those who did not recover [11,15]. Our findings also supported these results. There was a significant difference between the two groups in terms of lower dose antipsychotic usage, and it was also one of the factors determining employment. Because there is a significant relationship between high dose antipsychotic use and cognitive impairment, cognitive capacity is known to be an important factor for employment [41-45]. Both positive and negative symptom’s severity had a substantial effect on employment status and reasonable medical treatment increased daily life activities [46,47].
In this study, when the patients have longer illness duration, their employment rate decreased. As expected, we also found that the duration of disease of the working group was significantly less [10,11,14,32,34]. Other investigators found the similar decreased employment rate in a different culture [32]. Disease duration may decrease cognitive and social skills in patients with chronic schizophrenia just as antipsychotic dosage [14,34,42].
One of the important results of our study is that the existence of the previous working life has a significant relationship with employment. Previous work history was also found as a predictor of employment too [14,16,17]. The previous working life may also be a guide for social and functional skills that may be seen as an indicator of premorbid functionality.
As expected, total PANSS score and all subscales decreased in the patients employed in this study. In addition to other subscales, the prominent difference in the negative symptom subscale of functionality in literature has also been found in our study (Table 3) [11]. Our results supported the conclusion that symptoms severity decreases employment rate as seen in some previous studies [5,14,30,34]. Therefore, the results of previous studies suggesting a positive relationship between remission and employment are also repeated here. Because of the relationship between remission and employment is still unclear, but remission and employment have strong ties to each other. However, the remission status was not found to be a predictor of employment, which is similar to a recent study [5,14]. Whereas, functional recovery was predictor for employment. Functional remission critics overlook subjective feelings, the satisfaction of life and sustain social functioning [48]. In this study, we found nearly 30% higher employment rate in the remitted patients than in non-remitted ones. However, the employment rate was found to be nearly ten-fold higher in remission group. We have also seen that remission situation assessment cannot explain the whole group for employment status. In our study, the QLS, FROGS, and SubRAS points were significantly higher in the employee patients. This study also shows that remission, quality of life, and subjective recovery have strong correlation both in remitted and employment group. Our results indicate that subjective recovery feelings and employment status may play a vital role in a better long-term outcome in schizophrenia [14,34,47]. A recent study showed that increased self-perceived recovery is related to the quality of life [48,49]. They believe that high-level of socialization and active community involvement in patients with schizophrenia can lead to high self-perceived recovery even though they have substantial psychotic symptoms. Nevertheless, subjective recovery feelings were not found as a decisive factor for employment. This may also be due to the fact that common evaluation areas between SubRAS and FROGS, QoL. It has also been reported that there is a high correlation between these scales in the validity reliability study of the scale [23].
This study tried to determine the factors that may be related to employment in patients with schizophrenia. The results of this research underlined the concept of low dose antipsychotic use and functional recovery which may change within the treatment program besides static factors such as age and previous work life.
Although many studies suggest that symptomatic remission status affect functionality, in a broader concept, the employment rate is a predominant factor for subjective well-being and quality of life. We believe that employment as well as symptomatic remission will contribute significantly to social and functional recovery in daily life. For this reason, we believe that more projects, training programs and large-scale studies are needed to support the existence of our patients by producing within the society.
Limitations
Our study design is cross-sectional that may explain why we could not use time criteria in remission definition, which is typical in the cross-sectional studies. Study participants were in advanced age, and they had longer illness duration, had a history of multi-hospitalizations, relatively low level of education, and lack of social support, as well as, shorter duration of remission. Because of these factors listed above, our study results may not be generalizable to all patients with chronic schizophrenia. On the other hand, due to the fact that our sample large is not appropriate, regression analysis has not been applied in statistical method.
Notes
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Burcu Rahsan Erim. Data curation: Burcu Rahsan Erim. Formal analysis: Ersin Uygun, Hamid Boztas. Methodology: Burcu Rahsan Erim. Writing—original draft: Burcu Rahsan Erim. Writing—review & editing: Ersin Uygun, Hamid Boztas, Mustafa Yıldız.