Development of Brief Post-Traumatic Stress Disorder Rating Scale for Sexual Violence Victims
Article information

Abstract
The purpose of this study was to develop a brief rating scale of post-traumatic stress disorder (PTSD) symptoms among sexual violence victims. We analyzed the data from 195 victims and 220 non-victims to select meaningful items from the original PTSD rating scales. We also examined the validity of the brief scale by assessing internal consistency and ROC curves. The optimal cutoff scores for each brief scales were obtained. The results showed that a different approach may be required for early intervention in different age groups.
INTRODUCTION
Early screening of the post-traumatic stress disorder (PTSD) for sexual violence victims is crucial to prevent further adverse consequences. PTSD is one of the most distinguishing mental health problems among sexual violence victims [1]. It is also a risk factor for revictimization, especially for child victims [2]. Furthermore, high PTSD level at an early stage after the occurrence of sexual violence does not easily decrease even as time goes by [3]. Thus, more research that focus on detecting victims who experience PTSD symptoms in early stages following sexual violence are needed.
There have been efforts to develop brief scales for early assessment of PTSD symptoms. Lang and Connell [4] developed a brief trauma screening for children. Houry and colleagues [5] developed a brief mental health screening tool for the emergency department, although it is not a tool specific for PTSD. However, these scales do not fully cover the broad age group of sexual violence victims and are not designed as PTSD specific screening tools. Therefore, in this study, we aimed to develop a brief PTSD rating scale for each age group of sexual violence victims.
METHODS
Participants and procedures
From December 2016 to November 2018, we recruited female victims who have experienced sexual violence within the past 3 months. Recruitment took place at eight Sunflower Centers located across seven provinces in South Korea, which are support centers for sexual violence victims. Once victims who met the inclusion criteria visited the center, we explained the research and proceeded with data collection for those who agreed to participate. For children and adolescents who considered as vulnerable subjects, we received consent from one of their parents or a primary guardian. The control group was gathered through online advertisement and community boards.
This study was approved by the institutional review board for human subjects at the Seoul National University Hospital (IRB No. 1506-073-680).
A total of 470 subjects participated in the study. We used the data obtained from 415 participants after deleting the cases with missing values. The number of participants for each age group and their mean age were as follows: 1) adults: 107 victims; mean age 23.3 (SD=5.3, range: 18–48), 126 control group; mean age 24.8 (SD=7.9, range: 18–55), 2) adolescents: 55 victims; mean age 15.0 (SD=1.7, range: 13–18), 67 control group; mean age 14.5 (SD=1.0, range: 13–18), 3) children: 33 victims; mean age 9.5 (SD=2.1, range: 5–13), 27 control group; mean age 8 (SD=1.8, range: 5–13).
Measure
We used Post Traumatic Diagnostic Scale for the DSM-5 (PDS5) for adults, Child PTSD Symptom Scale (CPSS-V) for adolescents and Parent Report of Posttraumatic Symptoms (PROPS) for children.
Post Traumatic Diagnostic Scale for the DSM-5
PDS5 is a 24-item self-report measure based on diagnostic criteria of DSM-5, developed to measure the severity of PTSD symptoms in adults [6]. This is a 5 point Likert scale, rating from 0 to 4. The total score is the sum of responses of the 20 questions. The cut-off score is 28. Mean score (SD) among the victim group reached 42.32 (16.66) while only 5.75 (8.81) in the control group. Internal consistency of the scale in this research was 0.94.
Child PTSD Symptom Scale
CPSS-V is a 20-item scale devised to measure child and adolescent PTSD symptoms [7]. We used this scale only to adolescent. The scale uses a 5 point Likert scale, and responses are based on the severity and frequency of symptoms related to traumatic events. The cut-off score for this scale is 31. Mean score (SD) in the victim group was 36.43 (17.79) in contrast to 8.16 (12.08) in the control group. The internal consistency of the scale in this research was 0.93.
Parent Report of Posttraumatic Symptoms
PROPS is a 32-item scale developed for parents to assess their children’s behavior after a traumatic event [8]. Children’s self-report was also measured in this study, but we only included the parent report scale for the analysis because there was no significant difference in self-reports between victims and control groups. The cut-off score is 16. Mean score (SD) in the victim group was 17.27 (13.98) while only 6.04 (6.44) in the control group. Cronbach’s alpha was 0.96 in this study.
Statistical analysis
For item selection, we adopted two levels of analysis: itemlevel and factor-level. During the item-level analysis, we examined the item-total correlation. Also, we assessed discrimination and difficulty parameters using item response theory (IRT) analysis. Items showing higher difficulty solely react to the responders with more symptoms, while items with higher discrimination distinguish the symptom severity of responders better [9]. Thus, we prioritized discrimination score over difficulty score in IRT analysis. In cases where discrimination could not be calculated due to monotonous score distributions, we only included the difficulty results. Meanwhile, in factor-level analysis, we conducted varimax rotation. Factors in each scale were extracted until they have more than three items per each factor and showed acceptable internal consistency. Then, we checked the corrected item-factor correlation within each factor.
Items with scores above the cut-off values were primarily considered for selection. We adopted strict cutoff values for each analysis to discriminate meaningful items: 0.7 for item-total and corrected item-factor correlation [10], 1.3 for discrimination and 0.5 for difficulty from IRT analysis [11], and 0.6 for factor loading [12]. Items showing scores above the cutoff values across different types of analysis were our targets for selection.
To validate the brief scales constructed from selected items, we used two methods: internal consistency and receiver operating characteristics (ROC) analysis. In ROC analysis, we examined whether the brief-version have a diagnostic function parallel to the original version, and screening ability to distinguish victims from non-victims. In addition, we determined the optimal cutoff values for each brief-version scale. The areas under the ROC curves (AUCs) were considered together in scale validation. SPSS ver. 23 (IBM Corp., Armonk, NY, USA) was used for all analysis.
RESULTS
Items selected
We selected 7 items from PDS5 (24 items), 7 items from CPSS-V (20 items), and 10 items from PROPS (32 items). Results from the data analysis along with item contents are provided in Table 1.

Items Selected from PDS5, CPSS-V, and PROPS
Brief-scale validation
Each brief PTSD scale for different age groups showed high internal consistency. Cronbach’s α was 0.96 for brief PDS5 within adult victims, 0.94 for brief CPSS-V among adolescent victims, and 0.92 for brief PROPS in child victims.
The ROC analysis showed that a score of 7.5 is the optimal cutoff value for brief PDS5 in adult victims, with a sensitivity of 0.97 and a specificity of 0.94. The AUCs were 0.99 (p<0.001). The AUCs of the curve distinguishing victims and non-victims were 0.97 (p<0.001). In the adolescent victims, a brief CPSS-V showed that the optimal cutoff value is 10.5, with a sensitivity of 0.97 and a specificity of 0.95. The AUCs were 0.99 (p<0.001) and 0.87 (p<0.001), respectively. Lastly, in the child victims, 3.5 was found to be the optimal cutoff value for brief PROPS, with a sensitivity of 0.88 and a specificity of 0.71. The AUCs were 0.90 (p<0.001) and 0.74 (p<0.01) respectively as shown in Figure 1.
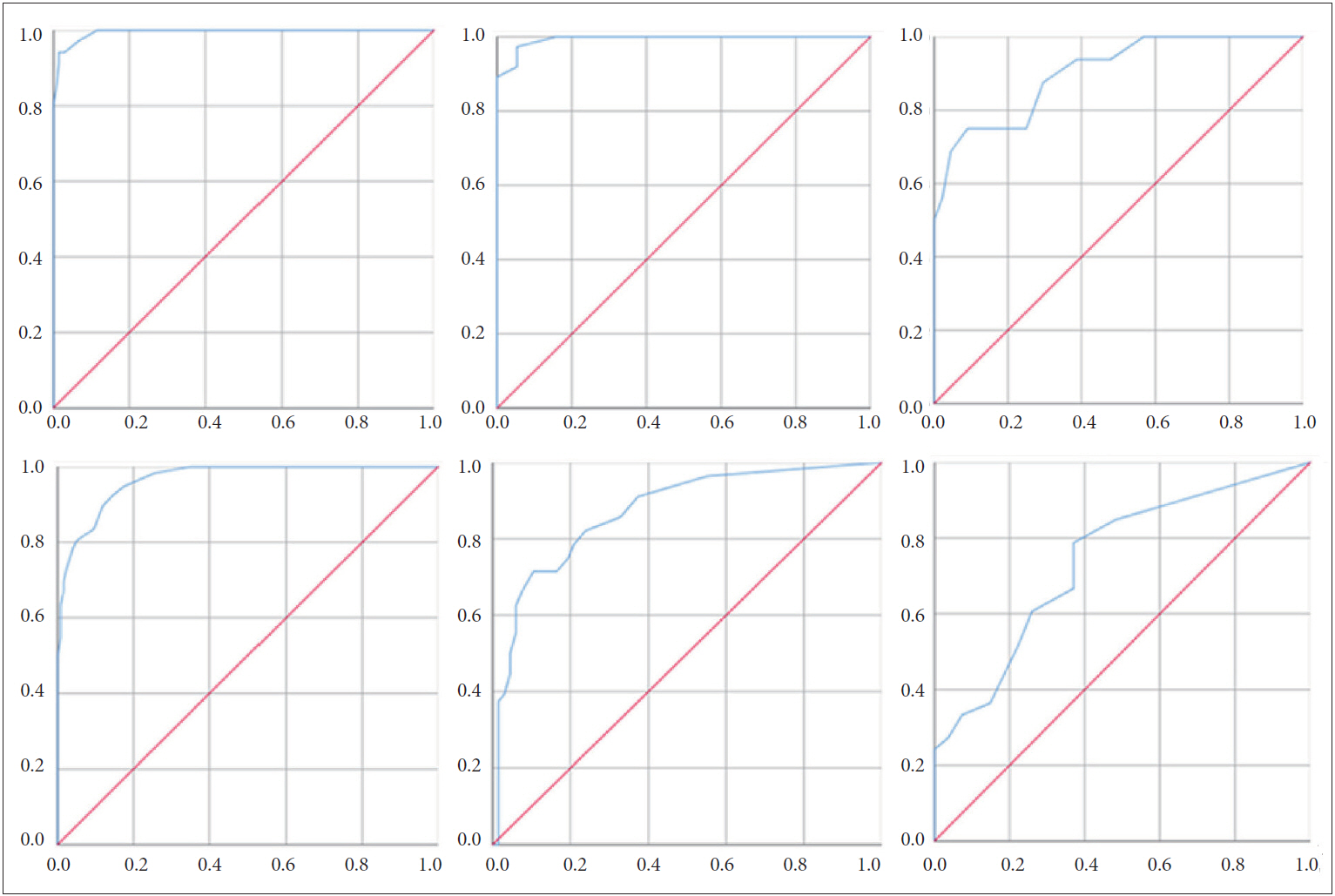
ROC Curves of Brief PDS5, CPSS-V, and PROPS. x: sensitivity, y: 1-specificity; adults (left), adolescents (middle), and children (right); comparison between brief/original scale (top) and victim/non-victim (bottom). ROC: Receiver Operating Characteristics, PDS5: Post Traumatic Diagnostic Scale for the DSM-5, CPSS-V: Child PTSD Symptom Scale, PROPS: Parent Report of Posttraumatic Symptoms.
DISCUSSION
The brief PTSD scales showed high internal consistency and wide AUCs. The results suggest that these scales could replace the original scales, and can be used with the optimal cut-off scores provided in this research. Also, given the contents of the items we chose for each age group, developing a customized intervention for the different age groups could amplify the effects of early intervention for PTSD [13]. Lastly, considering that only parental report showed a significant difference between child victims and control groups, it is especially important that parents or primary guardians carefully observe their child after the traumatic event.
Although victims may have different traumatic events other than sexual violence, the types of the traumatic events were not measured in this study. Thus, in future research, the different types of traumatic events need to be examined.
The strength of this study is that it was conducted on a large number of actual sexual violence victims. The development of brief scales would enable quick and efficient assessment of PTSD symptoms in primary care settings for victims.
Acknowledgements
This research was funded by Korea Mental Health Technology R&D Project (ID: HM15C1107).
We cooperated with eight Sunflower Centers: Seoul, Gwangju (Child), Gwangju (Crisis), Northwestern Gyeonggi, Gyeongnam, Busan, Jeonbuk, Chungnam.
English proofread by Daeun Suh.
Notes
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Jae-Won Kim. Data curation: Jihye Kwon, Bee Ryou. Formal analysis: Halin Chung. Funding acquisition: Jae-Won Kim, Kihyun Kim. Investigation: Jihye Kwon. Methodology: Halin Chung. Project administration: Jihye Kwon, Bee Ryou, Hee Jeong Ryu. Resources: Jae-Won Kim. Software: Halin Chung. Supervision: Jae-Won Kim, Kihyun Kim. Validation: Halin Chung. Visualization: Halin Chung. Writing—original draft: Halin Chung. Writing—review & editing: Halin Chung, Jae-Won Kim.