INTRODUCTION
Over 800,000 people die due to suicide every year, which is one person every 40 seconds. Based on current trends and WHO estimates for 2020, the global annual suicide fatalities could rise to approximately 1.53 million. Globally, suicide is one of the three leading causes of death among those aged 15-44 years and was ranked as the second leading cause of death among 15-29 year olds in 2012 [1,2]. In South Korea, suicide rates (per 100,000 deaths) increased from 13.6 in 2000 to 25.6 in 2016 [3]. This is well above the suicide rate of 12.0 per 100,000 deaths for countries of Organization for Economic Cooperation and Development (OECD) from 2012 to 2015, and is the highest among the OECD countries. South Korea had the second highest suicide rate in the world in 2015 [4].
It is known that the major risk factors for suicide are prior suicide attempts and depression [5,6]. Depressive disorder is the most common psychiatric disorder and its prevalence also affects the overall burden of the disease [7,8]. The suicide mortality rate in patients with depressive disorder is higher than the general population because patients with depressive disorder are more likely to attempt suicide using more fatal methods [9,10]. The risk factors of suicide in patients with depressive disorder include severity of depression, comorbidity with personality disorder, substance use disorder, etc [11]. Depressive disorder is frequently comorbid with borderline personality disorder (BPD). Previous findings state 40% of the inpatients with depression at a mental hospital in the USA were also reported to have BPD [12].
BPD is the most common personality disorder with a lifetime prevalence of 10% in the patients at the American Psychiatric Outpatient Clinic [13]. BPD is characterized by impulsiveness, aggressiveness, the use of primitive defense mechanisms such as splitting, projective identification, and denial, and engaging in self-harm and suicide attempts. Hence, this makes BPD a difficult disorder to treat [14,15]. BPD is the only personality disorder that includes suicide attempt or self-harm behavior in the diagnostic criteria [16]. Previous research on suicide attempts in patients with BPD revealed a suicide rate of 10%, which is about 50 times higher than the suicide rate of the normal population [17]. Moreover, patients with comorbid depressive disorder and BPD have a higher mortality rate than patients with only depressive disorder since the former tend to attempt suicide using more lethal ways [18]. The government of Netherlands estimated to spend approximately €87.5 million annually for suicide in patients with BPD [19].
Worldwide, the demand for suicide prevention continues to increase due to the increasing deaths by suicide and burden of associated social costs. Therefore, researchers have extensively studied the risk factors and prevention of suicide. In clinical settings, various attempts have been made as well to identify the risk factors for suicide [20-22]. A study based on the association between suicide and defense mechanisms revealed that the use of immature defenses such as passive-aggression, somatization, and projection was highly associated with suicide [23]. Psychiatric interview, self-report psychological tests, and clinician’s evaluation scales have been used to identify the psychological characteristics of suicide attempters. Each method has advantages and disadvantages. Whereas psychiatric interview is able to obtain more in-depth information, self-report psychological tests is simple, more economical, and easier to open up their subjective feelings [24]. Self-report psychological tests have been extensively used in studies investigating the psychological characteristics of suicide attempters with depression [24,25].
However, despite the high prevalence and high association with suicide, research on BPD has been mainly limited to biological causes, medication, and psychotherapy [26,27]. There have been few studies on defense mechanisms, and psychological characteristics associated with suicide attempt in patients with BPD. Therefore, we investigated psychological, symptomatic, and personality characteristics including defense mechanisms in suicide attempters and non-suicide attempters among patients with BPD using self-report psychological tests.
METHODS
Participants
The subjects were drawn from a pool of 18-65 year old inpatients and outpatients being treated at the psychiatric department of a Korean university hospital from October 2006 to December 2016. Patients who had filled the Symptom Checklist-90-Revised (SCL-90-R), the Minnesota Multiphasic Personality Inventory-2 (MMPI-2), the Personality Disorder Questionnaire-4+ (PDQ-4+), and Defense Style Questionnaire (DSQ) were shortlisted. The preliminary data sheets included the basic demographic data, comorbid conditions, the number and methods of suicide attempts, life stress, and other clinical data needed to conduct this study. All included patients met the criteria for BPD as per the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) and Diagnostic and Statistical Manual of Mental Disorder, 4th edition, test-revised (DSM-IV-TR) [28,29]. Patients with other personality disorders, intellectual disability, pervasive developmental disorder, autism spectrum disorder, psychotic features, and secondary psychiatric problem caused by organic problem or medications were excluded. Primary diagnoses were made on the basis of clinical assessments conducted by an experienced, board certified psychiatrist, which was then re-evaluated during an investigators’ meeting with four psychiatrists with chart review. Diagnoses and inclusion of the patients were then confirmed in this meeting. Finally, 125 patients with BPD were included in the sample. Forty-two patients with a history of one or more suicide attempts formed the suicide attempters group, while the remaining 83 patients with no history of suicide attempt formed the non-suicide attempters group. Since this was a retrospective study, it is exempted from obtaining participants’ consent. This study was reviewed and approved by the Institutional Review Board of the university hospital (YUMC 2015-12-020).
Assessments and measures
The SCL-90-R is a self-reporting, multidimensional, 90-item questionnaire consisting of nine symptom scales and three global scales [30]. Each item represents a psychological symptom, and each response ranges from not at all (0), a little bit (1), moderately (2), quite a bit (3), and extremely (4). Nine symptom scales consist of somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The global indexes are scores obtained by dividing total score by the total number of items. The global indexes consist of a general symptomatic index (GSI), a positive symptom total, and a positive symptom distress index [31-33]. The mean score of the GSI for functional population is 0.33, and the cutoff score between the functional and the moderately symptomatic is 0.60 [34]. The SCL-90-R is a tool which can be easily performed by non-experts within 20 minutes. Research has documented high reliability and validity of the SCL-90-R [35]. The Korean version of the SCL-90-R was used in this study [36,37].
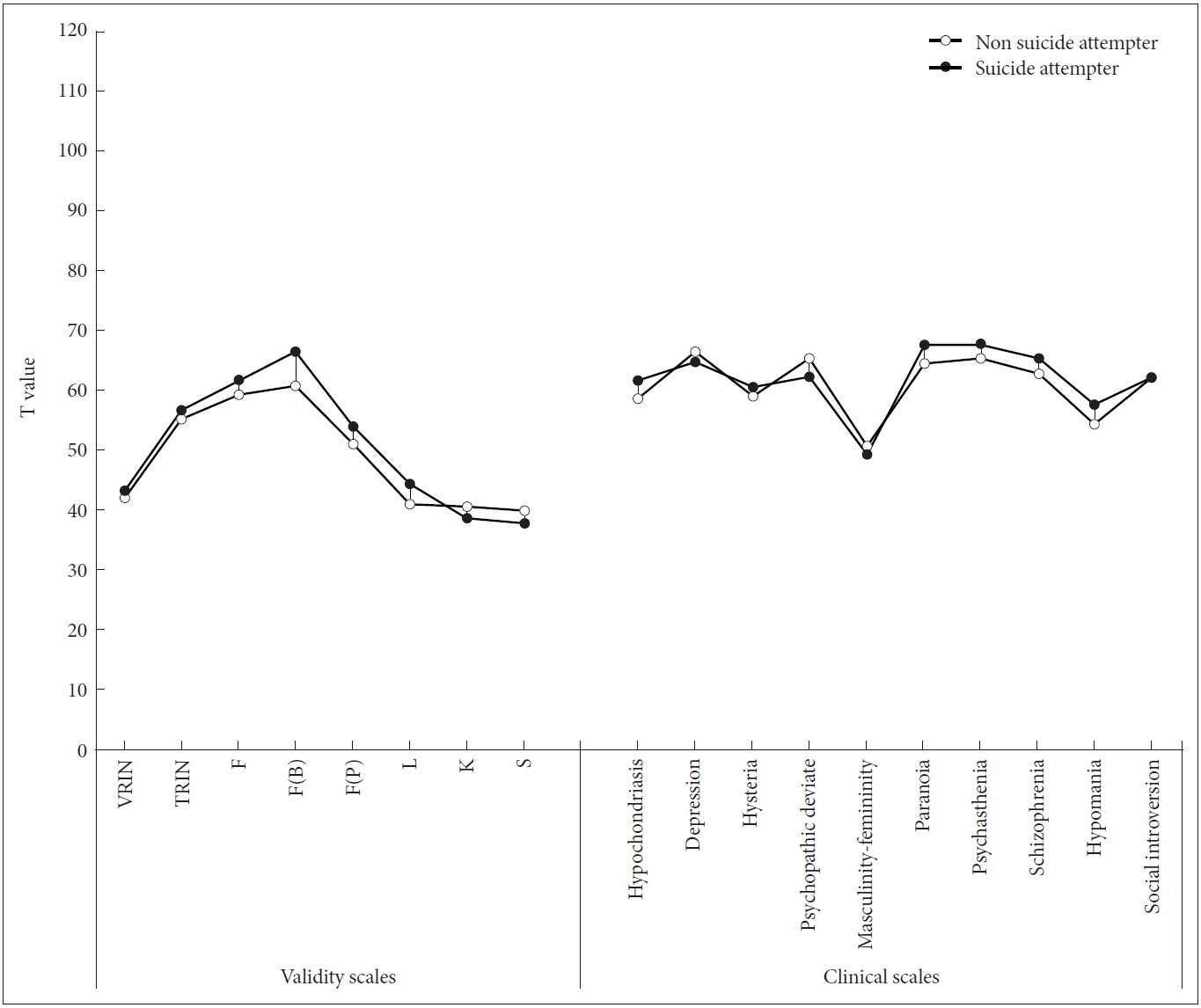
The MMPI was the first tool to objectively measure abnormal behavior and to classify psychiatric diagnosis. The MMPI-2, revised in 1989 by Butcher et al. [38], consists of a total of 576 questions. The MMPI-2 has been widely used in various fields including clinical settings [39]. The Korean version of the MMPI-2, standardized for the Korean population, was used in the current study [40]. Validity scales, are used to evaluate the examinee’s attitude in terms of consistency in responses (VRIN and TRIN scales), under-reporting trends (L, K, and S scales), and overreporting trends [F, F(B), F(P) scales]. The clinical scales are used to examine the status and severity of psychiatric symptoms, and personal characteristics. They consist of Hypochondriasis (Hs), Depression (D), Hysteria (Hy), Psychopathic deviate (Pd), Masculinity-femininity (Mf), Paranoia (Pa), Psychasthenia (Pt), Schizophrenia (Sc), Hypomania (Ma) and Social introversion (Si). Clinical scales except Mf and Si use uniform T scores. Clinical scales generally interpret scales with high T scores above 70, and scales with too low T scores and typically analyze the shapes of scales rather than single scale scores. In this study, the validity scales and 10 clinical scales of the MMPI-2 were used to identify the differences in psychological characteristics between suicide attempters and non-suicide attempters among patients with BPD.
The PDQ-4+ was developed by Hyler et al. [41], to evaluate personality disorders. The PDQ-4+, a 99-item self-report questionnaire, is based on the DSM-IV criteria for personality disorders. The Korean version of PDQ-4+ standardized in Korea by Kim et al. [42] was used in this study. The PDQ-4+ is designed to evaluate 12 personality disorders, including depressive personality disorder and negativistic personality disorder outlined in the appendix of DSM-IV, which were previously not included in the PDQ-4. All questions are true-false type (yes/no) and ‘yes’ means a pathological reaction. It includes four ‘too good’ questions to prevent subjects from undermining problems and two ‘suspect questions’ to figure out whether subjects are lying, or answering without sincerity. Except for the four ‘too good’ and the two ‘suspect questions’, a response of ‘yes’ to remaining 93 questions are regarded as pathological responses and counted as 1 point each. More than 3 points in each category of personality disorder indicates signs of specific personality disorder. Total score of normal people is usually 20 points or less, and total score of 30 or more usually highlight signs of personality disorders [42].
The DSQ, designed by Bond and Vaillant in 1986, is a self-reporting test measuring defense mechanisms [43]. The DSQ consists of 78 items that describe the conscious outgrowth of various defense mechanisms and 11 false items. The DSQ showed high validity and reliability and is widely used in the study of dynamic theory of personality. According to the DSQ, the defense styles consists of several defense mechanisms, which are classified into maladaptive, image-distorting, self-sacrificing and adaptive defense types according to the maturity of the defense. The DSQ also measures specific defense mechanisms such as projection and displacement [44].
Statistical analysis
Demographic data for both the groups was analyzed using frequency and descriptive analyses. Since the frequency analysis revealed a significant difference in gender between both groups, the multivariate analysis for the scores on SCL-90-R, MMPI-2, PDQ-4+, and DSQ was performed keeping gender constant. Clinical variables and psychological characteristics including comorbid conditions affecting suicide attempts were analyzed by binary logistic regression analysis. All statistical analyses were performed on IBM SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was indicated by p<0.05.
RESULTS
Demographic and clinical characteristics
Data for 125 subjects diagnosed with BPD at a Korean university hospital was analyzed. Table 1 and 2 summarize the demographic and clinical characteristics of the subjects. The analysis of the demographic data (Table 1) revealed a significantly higher number of females in the suicide attempters group. The analysis of the clinical characteristics (Table 2) for both groups revealed the highest comorbidity of BPD with depressive disorder. The methods of attempting suicide included the use of tools (15), intoxication (14), hanging (6), falling down (4), and others (2). Four patients did not respond. Among the suicide attempters group, 28 patients attempted suicide once, 7 patients attempted suicide twice, and 7 patients attempted suicide 3 or more times.
Psychological characteristics and defense mechanisms
SCL-90-R
As compared to the non-suicide attempters group, the suicide attempters group scored significantly higher on the hostility and the paranoid ideation subscales (p=0.021, p=0.038) (Table 3).
MMPI-2
The suicide attempters group scored significantly higher on the F, F(B), and L validity scales (p=0.026, p=0.003, p=0.001) and significantly lower on the S validity scale (p=0.037) in comparison to the non-suicide attempters group. The suicide attempters group scored significantly higher on the Pa, Pt, and Sc clinical scales (p=0.025, p=0.011, p=0.024) and significantly lower in the Mf clinical scale (p=0.002) as compared to the non-suicide attempters group (Table 4, Figure 1).
PDQ-4+
The suicide attempters group scored significantly higher on paranoid personality disorder (p=0.033) and significantly lower in antisocial personality disorder in comparison to the non-suicide attempters group (p=0.012) (Table 5).
DSQ
The suicide attempters group scored significantly higher on maladaptive, self-sacrificing and adaptive defense styles than the non-suicide attempters group (p=0.006, p=0.033, p=0.045). The suicide attempters group also scored higher on splitting, projective identification, and affiliation defense mechanisms than the non-suicide attempters group (p=0.021, p=0.005, p=0.003) (Table 6).
Regression analysis of clinical characteristics and psychological tests in the suicide attempters group
Factors that significantly influenced the tendency to attempt suicide were gender (p=0.006), the F(B) (p<0.001) and L (p=0.008) scales on the MMPI-2, and ‘splitting of other’s image’ defense mechanism on the DSQ (p=0.043) (Table 7). Females were 3.799 times more likely to attempt suicide than males. The number of suicide attempts increased by 1.067 times as the T score of F(B) on the MMPI-2 increased by 1, and the number of suicide attempts increased by 1.160 times as ‘splitting of other’s image’ defense mechanism on the DSQ increased by 1. The classification accuracies for these factors were 41.5% for the suicide attempters group, 87.8% for the non-suicide attempters group, and 72.4% for both groups combined.
DISCUSSION
This study aimed to investigate the differences in defense mechanisms, clinical symptoms, and psychological characteristics between suicide attempters and non-suicide attempters among patients with BPD.
The analysis of the demographic and clinical characteristics of the subjects showed a difference in terms of gender between the suicide attempters group and non-suicide attempters group. The proportion of females in the suicide attempters group was significantly higher, remaining consistent to the phenomenon that the worldwide suicide mortality was higher among males and suicide attempt rates were higher in females [45,46]. In addition, this result confirms the finding that females have a higher tendency to attempt suicide and to use more diverse methods than males among patients with BPD [14]. Hence, the statistical analysis was performed keeping the effect of gender differences between the two groups controlled. There was no significant difference between the suicide attempters group and non-suicide attempters group in terms of relevant life events. This was inconsistent with previous studies that suggest a higher tendency to attempt suicide behaviors when experiencing stressful life events [5,47]. However, other studies have also shown that stressful situations and suicide attempts are not always correlated [48,49]. Therefore, this result is consistent with previous findings that state an individual’s coping style with stressful life events affects their tendency to attempt suicide [50,51]. In other words, the inner world of the patient affected by stress is supposed more important to suicide attempt than the external stress itself.
The results of SCL-90-R revealed that patients in the suicide attempt group scored significantly higher on the hostility and paranoid ideation subscales. This result is consistent with previous findings that suggest hostility is associated with suicide regardless of depression [52], and suicide attempters were more hostile than non-suicide attempters among patients with BPD [53]. Hostility is associated with the impulsive-aggressive dimension and encompasses emotional components such as anger or resentment [53]. Therefore, the results of this study suggest that suicide attempts in patients with BPD are associated with anger caused by internal hostility and frustration.
The profiles of MMPI-2 showed that patients in the suicide attempters group scored significantly higher than the non-suicide attempters group on F, F(B), and L validity scales. The comparatively higher scores on F and F(B) scales in the suicide attempter group suggest that the suicide attempters group experienced greater discomfort than the non-suicide attempters group. The difference in the scores on the L scale indicates a higher tendency of the suicide attempters groups to deny their symptoms as compared to the non-suicide attempters group. It could be assumed that suicide attempters experience severe discomfort due to their symptoms; however, the internal conflict caused by denial of these symptoms also affects an individual’s tendency to attempt suicide. The suicide attempters group scored significantly higher on the Pa, Pt, and Sc clinical scales and significantly lower on the Mf clinical scale than the non-suicide attempters group. It can be inferred that suicide attempters are more paranoid, suspicious, hostile, and tend to get angry easily even with minor triggers in relation to themselves. In addition, the presence of an obsessive trait is likely to cause severe anxiety, and a high Sc score may indicate a feeling of alienation from the surroundings and a tendency to avoid social environment. These results were consistent with previous studies depicting an association between high scores on Pd, Pa, and Sc scales and suicidal behavior [54]. However, it is necessary to pay attention to the interpretation of the results because the results of the MMPI may not always be identically repeated and reflect a various individual inner worlds [55].
The analysis of the scores on the PDQ-4+ revealed significantly higher scores on paranoid personality disorder scale in the suicide attempters group. This suggests that suicide attempters tend to be more paranoid and suspicious in interpersonal relations than non-suicide attempters. However, the suicide attempters group scored significantly lower on the antisocial personality disorder scale than the non-suicide attempters group. This result undermines evidence that suggests that the risk of attempting suicide increases with presence of antisocial personality trait in patients with BPD [18]. Antisocial personality disorder can be accompanied by impulsivity and anger like in BPD, however, the impulsivity and anger in antisocial personality disorder is more likely to be controlled in order to benefit oneself or control others [56]. Therefore, the characteristics of antisocial personality disorder may be assumed to play a role in reducing the tendency to attempt suicide. Additional studies may be required to confirm this assumption.
The analysis of the scores on the DSQ revealed significantly higher scores for the suicide attempters group than the non-suicide attempters group on maladaptive and self-sacrificing defense styles. Previous studies have depicted a positive correlation between maladaptive and image-distorting defense styles with the degree of personality disorder (Johnson, Bornstein, and Krukonis 1992). Furthermore, maladaptive action is an immature defense style that is associated with most personality disorders, whereas self-sacrificing defense style is associated with neurotic symptoms [43].
The results of this study suggest that patients with severe BPD who are more likely to use maladaptive defense style are more likely to attempt suicide. This also confirms previous findings that suggest that the number of suicide attempts made by patients with major depressive disorder in their life span is associated with the use of both immature and neurotic defense styles [57]. The analysis indicated no difference in the use of image-distorting between the two groups, because the image-distorting defense style is a common defense mechanism in patients with personality disorders, and both groups comprise of patients with BPD. In detail, the suicide attempters group showed a significantly higher tendency to use splitting, projective identification, and affiliation defense mechanisms than the non-suicide attempters group. It can be inferred that the experience of being frustrated due to negative impact on interpersonal relationship when patients with BPD using affiliation simultaneously uses projective identification and splitting (immature and primitive defense mechanisms) may cause a greater emotional response to the patients. This also supports previous findings that the person who has tried more suicide attempts tends to use more detailed defense mechanisms such as projections and splitting [23].
On the other hand, although the level of significance was not high, there was a difference in the adaptive defense style between the suicide attempters group and non-suicide attempters group. There were some previous studies that the suicide attempters group had higher in mature defense style than non-suicide attempters group [23,57]. It is estimated that a group high on adaptive defense style and maladaptive and self-sacrificing defense styles together, experiences more discomfort. Similarly, people who use affiliation and primal defense mechanisms such as splitting, projective identification and etc. together, experience more discomfort in reality. In addition, splitting, the most basic defense mechanism of borderline personality disorder, may be related to the tendency of patients to wax and wane between pathological and normal conditions. Therefore, it might be necessary to explore the ratio of healthy defense mechanisms to psychopathological immature defense mechanisms rather than focusing on one dominant defense style.
In this study, these factors predicted non-suicide attempters group more accurately than the suicide attempters group. Considering that the number of non-suicide attempters was twice as large as that of suicide attempters, the psychological characteristics of non-suicide attempters group may have been biased. In conclusion, female, severe discomfort due to symptoms and denial of symptoms at the same time, increased use of immature defense mechanisms such as splitting may constitute the risk factors for suicide attempts in patients with BPD. Further evaluation of the above findings might be necessary to confirm these conclusions.
This study has several limitations. Firstly, since this study focused only on patients at one university hospital, it may be difficult to assess the extent to which these findings can be generalized. Secondly, all psychological characteristics were measured using self-report tools. Finally, as a retrospective study, it is not possible to determine whether the differences between the suicide attempters group and non-suicide attempters group are the cause or the result of suicide attempts. Future research must focus on prospective studies to confirm the causal relationship. Despite these limitations, this study examined the psychodynamic aspects, clinical features, psychological characteristics, and defense mechanisms in a relatively larger sample of patients than samples previously studied. Therefore, this study may aid in understanding the psychological characteristics of suicide attempters among patients with BPD, and in estimating the risk factors for suicide attempt in patients with BPD.